Page 5 of 14
SU9.2 | Early Cancer Detection and Multidisciplinary Care — SDL Guide (Part 2)
From Detection to Multidisciplinary Management
Detecting a cancer early only helps if it is then managed well, and modern cancer care is explicitly a team activity rather than the decision of any single doctor — this is the clinical and applied significance of early detection. Once a cancer (or precursor) is found and the diagnosis confirmed on tissue and the disease staged, the case is taken to a multidisciplinary team (MDT), also called a tumour board. Its purpose is to bring every relevant expert to the same table so that one coordinated, evidence-based, stage-appropriate plan is agreed. The core members are the surgeon, the medical oncologist (chemotherapy, targeted and immunotherapy), the radiation oncologist (radiotherapy), the radiologist (imaging and staging), the pathologist (tissue diagnosis, grade, margins and biomarkers), and a specialist cancer nurse, with palliative-care, psychological and other support as needed. Together they integrate the diagnosis, stage and the patient's fitness and wishes to choose among the treatment modalities — surgery, chemotherapy, radiotherapy, targeted/immunotherapy, and palliative and supportive care — often in combination. The earlier the detection, the more often this plan can be curative and the less aggressive it needs to be: a small, early, localised cancer may need surgery alone, whereas advanced disease requires multimodal or purely palliative treatment. Warning-sign awareness and screening therefore feed directly into the MDT pathway, which is where a timely diagnosis is finally converted into the best achievable outcome for the patient.
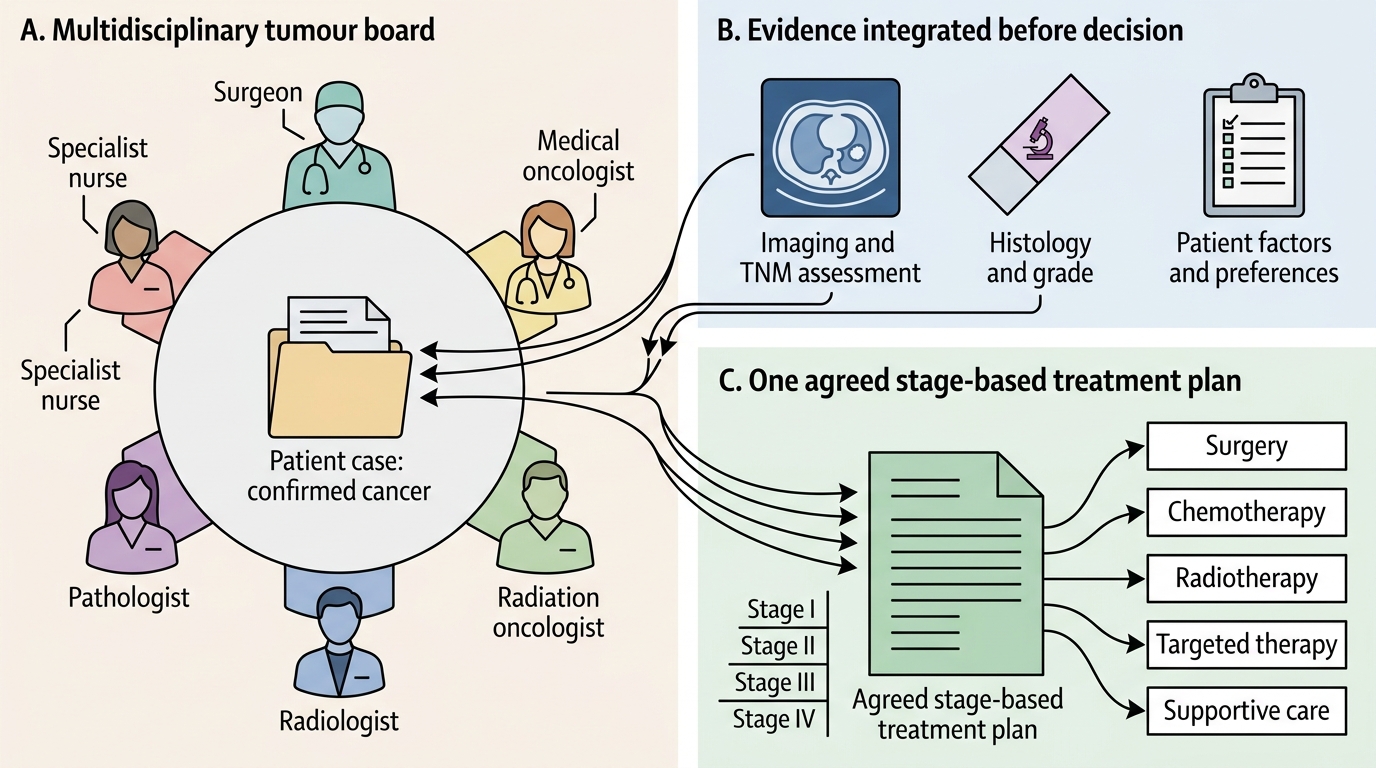
Multidisciplinary Tumour Board and Stage-Based Cancer Treatment Planning
Check Your Understanding
Consolidate the foundation as a single chain of reasoning. Start from the biology: most carcinomas evolve through dysplasia and carcinoma-in-situ (confined above the basement membrane) before becoming invasive, and this slow natural history creates a detectable pre-clinical window — the reason early detection is even possible, and the reason removing a precursor (an adenomatous polyp, treated CIN) can prevent cancer outright. Distinguish the two routes to early detection: screening tests the asymptomatic population and is justified only when the Wilson-Jungner criteria hold (the established programmes being cervical Pap/HPV, breast mammography, and colorectal FOBT/FIT then colonoscopy), while early diagnosis acts promptly on warning signs in symptomatic people. Keep the caveats in mind: a programme is judged by reduced mortality, not cancers found, guarding against lead-time bias and overdiagnosis. Finally, once cancer is detected and staged, the multidisciplinary tumour board integrates surgeon, medical and radiation oncologist, radiologist, pathologist and specialist nurse to agree one stage-based plan across surgery, chemotherapy, radiotherapy, targeted therapy and supportive care. Self-test: can you explain the detection window biologically; can you state when screening is worthwhile and name the three programmes; can you list the key cancer warning signs; and can you describe who sits on a tumour board and why? The questions below check exactly these.
SELF-CHECK
What is the central purpose of a multidisciplinary team (tumour board) in cancer care?
A. To let the surgeon make the final decision alone after hearing others
B. To bring all relevant specialists together to agree one coordinated, stage-based treatment plan
C. To replace tissue diagnosis and staging with a committee vote
D. To screen the asymptomatic population for new cancers
Reveal Answer
Answer: B. To bring all relevant specialists together to agree one coordinated, stage-based treatment plan
The tumour board exists so that the surgeon, medical and radiation oncologists, radiologist, pathologist and specialist nurse can integrate the diagnosis, stage and patient factors into ONE coordinated, evidence-based, stage-appropriate treatment plan. It does not hand the decision to one person, does not replace tissue diagnosis or staging, and is a management forum, not a screening activity.