Page 7 of 17
SU10.3 | Observing and Assisting Surgical Procedures — SDL Guide
Learning Objectives
- Describe the roles of the operating-theatre team (sterile and non-sterile members) and the governing principles of being a surgical assistant (SU10.3).
- Outline the technique of scrubbing in and the core assisting tasks — retraction, exposure, suction, suture-cutting and camera-holding — while maintaining the sterile field (SU10.3).
- Observe common and emergency lifesaving surgical procedures and assist in minor procedures, reading the operative field and communicating safely with the team (SU10.3).
INSTRUCTIONS
Watching and assisting at operations is how every surgeon begins, and it is far from passive: a good assistant gives the operating surgeon a clear, exposed, bloodless field and keeps the sterile field intact, while a careless one contaminates the field or obscures the view. This module teaches you the theatre team and its rules, the technique of scrubbing in and assisting, and how to read the operation as it unfolds — so that when you observe and assist under supervision you add to the operation's safety, not its risk.
References
- Bailey & Love's Short Practice of Surgery, The Operating Theatre and Basic Surgical Skills (textbook)
- SRB's Manual of Surgery, Operation Theatre, Asepsis and Surgical Skills (textbook)
- Sabiston Textbook of Surgery, Principles of Operative Surgery (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A student is invited to scrub in for the first time. Keen to help, she leans across the instrument trolley to get a better view, drops her hands below her waist while waiting, and turns her back on the field to look at the monitor. In under a minute she has contaminated the sterile gown three times over — and every time, the scrub nurse has to stop the operation to re-establish a sterile field. The surgeon was not slowed by a difficult dissection; he was slowed by an assistant who did not yet know the rules of the room. Assisting is not about knowing the operation; it is about knowing how to be useful and safe in a sterile, high-stakes environment. The best first assistants are quiet, anticipatory and disciplined — they hold the retractor exactly where it is needed, keep the field dry and exposed, and never break the sterile barrier. Those habits are learnt before you ever pick up an instrument.
WHY THIS MATTERS
Observing and assisting is the gateway to all of operative surgery and a safety-critical role in its own right. As a student and junior doctor you will spend many hours in theatre, and what you contribute — good exposure, a dry field, an intact sterile barrier, anticipation of the next step — directly affects how safely and quickly the operation goes. Conversely, an assistant who contaminates the field, obscures the view or fails to communicate adds real risk for the patient. Learning the theatre's roles, asepsis and assisting technique also lets you learn the operations themselves far faster, because you are inside the procedure rather than watching from the back. This competency is examined and is a prerequisite to progressing to performing procedures yourself. Building these habits now — sterile discipline, anticipation, clear communication — is what turns time spent in theatre into genuine surgical learning rather than passive attendance.
RECALL
Recall the asepsis foundation this skill depends on. Recall that sterilization destroys all microbes including spores, and that the operating field is kept free of microorganisms by combining sterile instruments, prepared skin and a maintained sterile field. Recall the technique of surgical hand antisepsis (a timed scrub or alcohol rub, hands kept above the elbows), donning a sterile gown touching only its inner surface, and closed gloving (keeping the hands inside the gown cuff until gloved so skin never touches the glove's outer surface). Recall too, from your perioperative learning, the WHO Surgical Safety Checklist and its three pause-points — the Time Out before incision is performed by the whole team and is something you will participate in. Assisting is the application of all of this discipline at the operating table, alongside the surgeon.
Why Learning to Observe and Assist Matters
The indication for learning to observe and assist is that it is the universal entry point to operative surgery and a genuine safety role, not merely spectating. Observing means watching an operation attentively to learn its steps, anatomy and decisions; assisting means actively helping the operating surgeon — most importantly by providing exposure and keeping the field clear — while preserving asepsis. Both are clinical skills with right and wrong ways to perform them. The reason they matter is twofold. First, the assistant materially affects the operation: good retraction and exposure let the surgeon see and work safely, suction and swabbing keep the field dry, and an intact sterile barrier protects the patient from infection — whereas a poor assistant obscures the view, contaminates the field or has to be repeatedly corrected, all of which add time and risk. Second, observing and assisting is how surgical knowledge is actually acquired: by being inside the procedure you learn anatomy as it is revealed, the sequence of steps, and the judgement behind them far better than from a textbook. The competency also has a defined scope — you will observe common and emergency lifesaving procedures and assist in minor ones — reflecting that more is asked of you as your competence grows. The rest of this module covers the theatre team and its rules, the technique of scrubbing in and assisting, how to read the operative field, and how you will practise under supervision.
The Operating Team and the Governing Principles of Assisting
Safe assisting begins with knowing who is in the room and the rule that divides them. The operating team has a sterile (scrubbed) team — the operating surgeon, the assistant(s), and the scrub nurse (or scrub practitioner) who manages the instruments — all of whom are scrubbed, gowned and gloved and may touch the sterile field. It also has a non-sterile team — the circulating (runner) nurse, who fetches supplies, connects equipment and documents but never touches the sterile field, and the anaesthetist, who manages the patient's anaesthesia and physiology at the head of the table. The governing principle that organises everything is the sterile field: a defined microbe-free zone made up of the sterile drapes around the operative site and the sterile parts of the team's gowns and gloves. You must know exactly which parts of yourself are sterile: the front of the gown from chest to waist and the sleeves to just above the elbow are sterile; the back of the gown, anything below the waist, and the area above the shoulders or below the table are not sterile and must be treated as contaminated. From this flow the rules of sterile discipline: keep your hands above waist level and in view at all times; never let the hands drop below the waist or be tucked away; never turn your back on or reach across the sterile field; gowned staff pass each other front-to-front or back-to-back with care; only sterile items touch sterile items; and any glove perforation or suspected contamination is corrected at once by re-gloving or re-gowning. Knowing the roles and the geometry of the sterile field is what lets you move in theatre without endangering the patient.
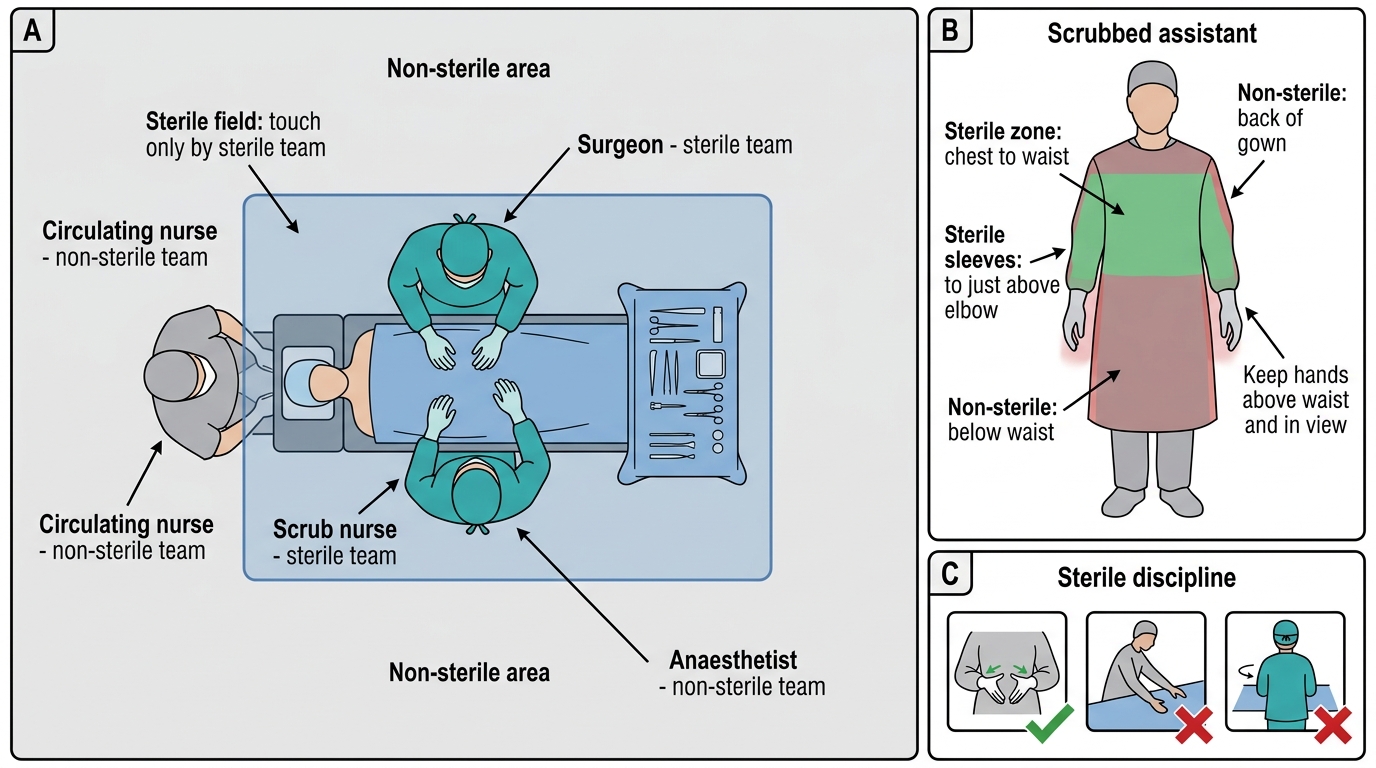
Sterile Team, Non-Sterile Team, and Gown Sterile Zone in the Operating Theatre
- Sterile team: surgeon, assistant(s), scrub nurse — scrubbed, gowned, gloved; may touch the field.
- Non-sterile team: circulating (runner) nurse and anaesthetist — never touch the sterile field.
- Sterile zone of the gown: front chest-to-waist and sleeves to just above the elbow only.
- Discipline: hands above waist and in view; never turn the back on or reach across the field; re-glove on any breach.
SELF-CHECK
Once you are gowned and gloved as a scrubbed assistant, which of the following is considered part of YOUR sterile zone?
A. The back of your gown
B. Anything below your waist
C. The front of your gown from chest to waist and your sleeves to just above the elbow
D. Your gloved hands wherever you place them, including by your sides
Reveal Answer
Answer: C. The front of your gown from chest to waist and your sleeves to just above the elbow
Only the front of the gown from chest to waist and the sleeves to just above the elbow are sterile. The back of the gown, anything below the waist, and the area above the shoulders are NOT sterile — which is why hands must stay above waist level and in view, and you never turn your back on the field.
The Technique of Scrubbing In and Assisting
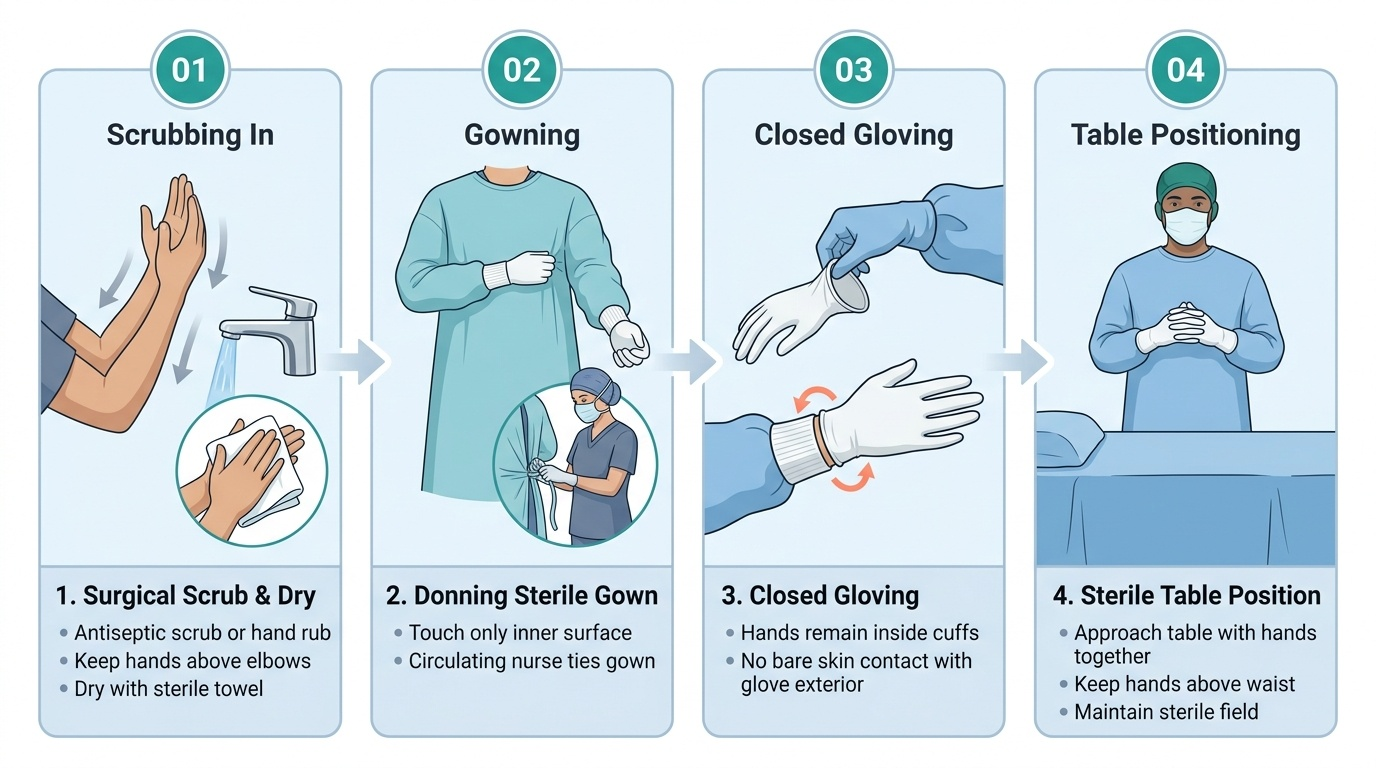
Assisting has a definite technique, and it begins before you reach the table. First, scrub in: change into theatre attire with cap and mask, remove jewellery and clean under the nails, then perform surgical hand antisepsis — a timed antiseptic scrub (chlorhexidine or povidone-iodine) or an alcohol-based hand rub — keeping the hands above the elbows so water runs from clean to less-clean, and dry with a sterile towel. Don the sterile gown touching only its inner surface, then glove using the closed technique so bare skin never contacts the glove's outer surface; have the circulating nurse tie the gown. Approach the table keeping hands together, above the waist and in view. Once positioned, your core assisting tasks are: retraction and exposure — holding retractors steady at the angle and tension the surgeon needs, providing countertraction on tissues to open up planes, without obscuring the surgeon's view or your own; keeping the field clear — suction of blood and fluid, and swabbing by dabbing (not wiping, which dislodges clot); cutting sutures to the length the surgeon specifies, cutting under direct vision with the tips of the scissors; assisting haemostasis by exposing a bleeding point so it can be controlled; and in minimal-access (laparoscopic) surgery, holding the camera steady, level and centred on the operative target, following the surgeon's instrument. Throughout, you pass and receive sharps safely (via a neutral zone, announced), keep instruments off the patient's body, and maintain the sterile field. Good assisting is unobtrusive, anticipatory and steady — the surgeon should barely have to ask.
Provided image
- Scrub in: attire/cap/mask → surgical hand antisepsis (hands above elbows) → sterile gown (inner surface only) → closed gloving.
- Expose: steady retraction and countertraction at the surgeon's angle; do not obscure the view.
- Keep the field clear: suction; swab by dabbing, not wiping.
- Assist: cut sutures to length under vision; expose bleeding points; hold the laparoscopic camera steady and centred.
- Safety: pass sharps via an announced neutral zone; maintain the sterile field throughout.