Page 1 of 17
SU10.1 | Principles of Perioperative Management — SDL Guide
Learning Objectives
- Describe the three phases of perioperative care — preoperative, intraoperative and postoperative — and why structured perioperative management reduces preventable surgical morbidity (SU10.1).
- State the governing principles of perioperative care: ASA physical status risk stratification, preoperative optimisation and fasting, VTE and surgical antibiotic prophylaxis, and the WHO Surgical Safety Checklist (SU10.1).
- Outline the perioperative sequence including the three WHO checklist pause-points and the ERAS approach, and recognise common postoperative complications (SU10.1).
INSTRUCTIONS
An operation is only as safe as the care that surrounds it. This module gives you the framework that turns a list of disconnected tasks — the consent, the fasting order, the antibiotic, the checklist, the postoperative round — into one coherent system that keeps patients safe from the decision to operate until they recover. Learn the three phases, the principles that govern each, and the safety systems (the WHO checklist, ERAS) that make modern surgery reliable.
References
- Bailey & Love's Short Practice of Surgery, Preoperative and Postoperative Care (textbook)
- SRB's Manual of Surgery, Preoperative Preparation and Postoperative Management (textbook)
- Sabiston Textbook of Surgery, Principles of Preoperative and Operative Surgery (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Two patients are scheduled for the same elective operation. The first arrives with an uncontrolled blood sugar that no one optimised, is starved from the previous midnight 'to be safe', receives no clot prophylaxis, and is wheeled to theatre while the team assumes someone else confirmed the consent and the side of surgery. The second has her diabetes tuned, drinks clear fluids until two hours before, wears compression stockings, and is greeted by a team that stops, reads a checklist aloud, and confirms her name, procedure and site before a single incision. Both operations are technically identical. Yet the first patient is the one who develops a wound infection, a chest complication and a deep-vein thrombosis. The difference was never the surgery — it was the management around it. Perioperative care is where most preventable surgical harm is won or lost.
WHY THIS MATTERS
Most of what determines whether a surgical patient does well happens outside the few minutes of actual cutting. Preventable complications — surgical site infection, venous thromboembolism, chest infection, wrong-site surgery, fluid and electrolyte errors — cluster in the hours before and after the operation, and structured perioperative management is the single most effective tool against them. As a junior doctor you will spend far more time managing patients before and after surgery than operating: clerking and optimising them, confirming consent and fasting, prescribing prophylaxis, participating in the safety checklist, and running the postoperative ward round. Getting these principles right is examined directly and, more importantly, is what keeps your patients alive and recovering. This module builds the mental map you will use on every surgical patient you ever see.
RECALL
Recall the foundations this skill builds on. From your asepsis learning, recall that surgical site infection is largely preventable by aseptic technique and correct antibiotic timing — perioperative care is where that timing is delivered. From anaesthesia (AS), recall the ASA physical status classification and the fasting guidance (clear fluids 2 h, breast milk 4 h, formula/light meal 6 h, fatty or fried solids 8 h), both of which the surgical team must respect. Recall too the physiology of the metabolic response to injury — surgery is a controlled injury that triggers catabolism, fluid shifts and a stress response — which is why optimisation, analgesia, early feeding and mobilisation matter. Perioperative management is the deliberate application of all of this around a single operation.
Why Perioperative Management Decides Surgical Outcome
The indication for structured perioperative management is every surgical patient, because outcome depends far more on the system of care than on operative skill alone. Perioperative management is the coordinated care of a patient across three phases — the preoperative phase (from the decision to operate until the patient enters theatre), the intraoperative phase (in theatre), and the postoperative phase (recovery until discharge and beyond). Its purpose is to anticipate and prevent harm: to enter the operation with the patient as fit as possible, to keep the operation itself safe, and to return the patient to function quickly. The logic is that surgical morbidity is dominated by a small number of recurrent, preventable problems — infection, thromboembolism, respiratory and cardiac events, fluid and metabolic derangement, and the rare but catastrophic wrong-patient or wrong-site error. Each has a known countermeasure that lives in the perioperative pathway: optimisation and prophylaxis before, checklists and asepsis during, and surveillance and early mobilisation after. Framing care as three linked phases, rather than isolated tasks, is what makes the countermeasures reliable. The rest of this module fills in the principles that govern each phase, the step-by-step sequence including the WHO Surgical Safety Checklist, how to interpret the deteriorating patient, and how you will apply all of it under supervision.
The Governing Principles: Risk, Optimisation and Safety Systems
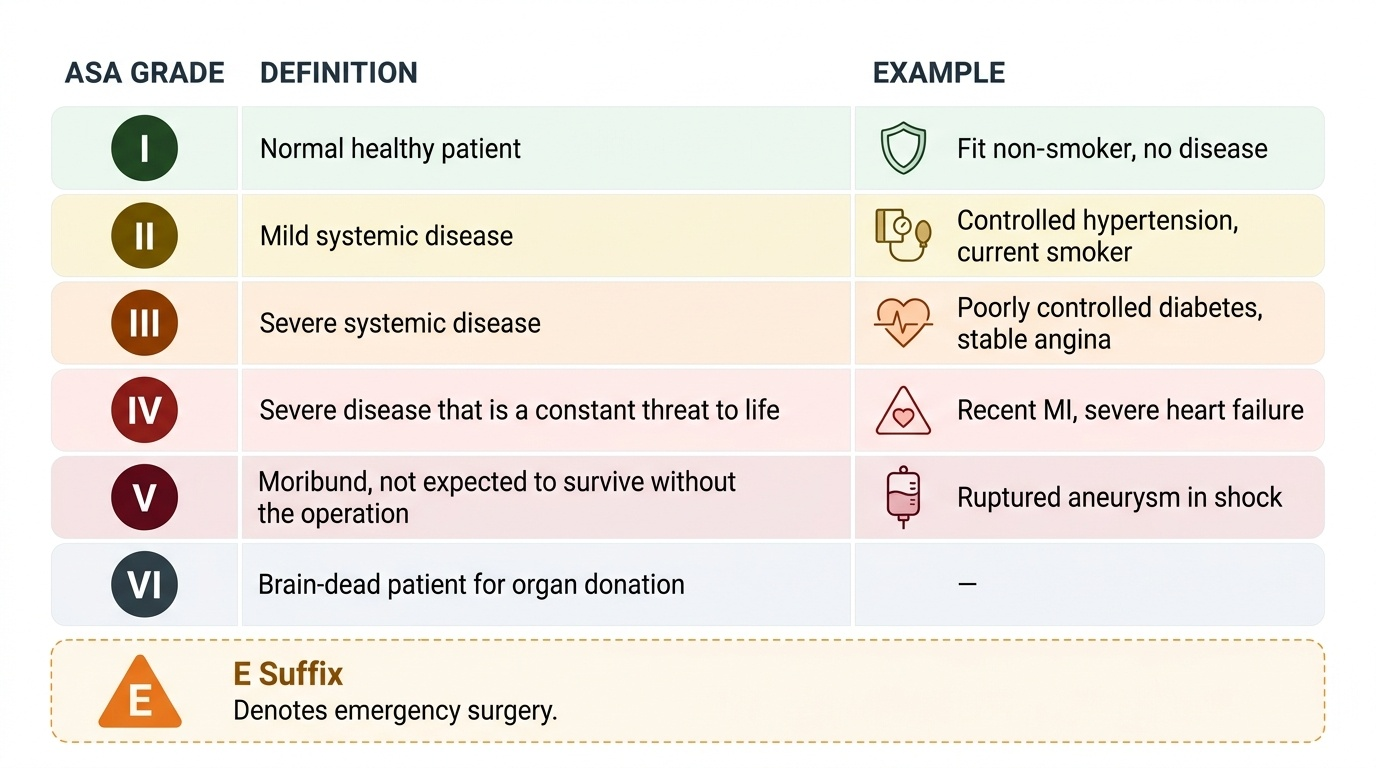
Sound perioperative care rests on a few principles that you apply to every patient. The first is risk stratification: before any operation, grade the patient's fitness so that risk is understood and shared. The most widely used tool is the ASA physical status classification, which grades the patient's systemic disease from ASA I (a normal healthy patient) to ASA VI (a brain-dead organ donor), with an E suffix for emergency surgery. A crucial caution: ASA grades the patient's systemic illness, not the difficulty or risk of the operation itself, and it is a different scale from the Mallampati airway grade — do not conflate them. The second principle is preoperative optimisation: correct what is correctable before surgery — control diabetes and hypertension, treat anaemia, manage cardiac and respiratory disease, and review anticoagulants and other drugs. The third is fasting to reduce aspiration risk, using the modern '2-4-6-8' rule (clear fluids 2 h, breast milk 4 h, formula or light meal 6 h, fatty or fried solids 8 h) rather than a blanket 'nil by mouth after midnight'. The fourth is prophylaxis against the two commonest preventable complications: venous thromboembolism (VTE), prevented by risk-assessing every patient and combining mechanical measures (graduated compression stockings or intermittent pneumatic compression) with pharmacological prophylaxis (low-molecular-weight heparin) where indicated; and surgical site infection, reduced by antibiotic prophylaxis given within 60 minutes before incision for the right operations. The final principle is the use of safety systems — standardised checks that catch human error — of which the WHO Surgical Safety Checklist is the keystone.
Provided image
| ASA grade | Definition | Example |
|---|---|---|
| I | Normal healthy patient | Fit non-smoker, no disease |
| II | Mild systemic disease | Controlled hypertension, current smoker |
| III | Severe systemic disease | Poorly controlled diabetes, stable angina |
| IV | Severe disease that is a constant threat to life | Recent MI, severe heart failure |
| V | Moribund, not expected to survive without the operation | Ruptured aneurysm in shock |
| VI | Brain-dead patient for organ donation | — |
| E | Suffix added for emergency surgery | ASA II E |
SELF-CHECK
A patient with poorly controlled diabetes and stable angina is being graded before elective surgery. What does the ASA physical status classification describe?
A. The technical difficulty of the planned operation
B. The patient's systemic disease and physical fitness
C. The predicted airway difficulty at intubation
D. The expected blood loss during surgery
Reveal Answer
Answer: B. The patient's systemic disease and physical fitness
ASA physical status grades the patient's systemic disease and overall fitness (I healthy to VI brain-dead, with E for emergency) — NOT the difficulty or risk of the operation, and NOT the airway (that is the separate Mallampati grade). This patient's poorly controlled diabetes and stable angina place them at ASA III.
The Perioperative Sequence — Preoperative, Intraoperative, Postoperative
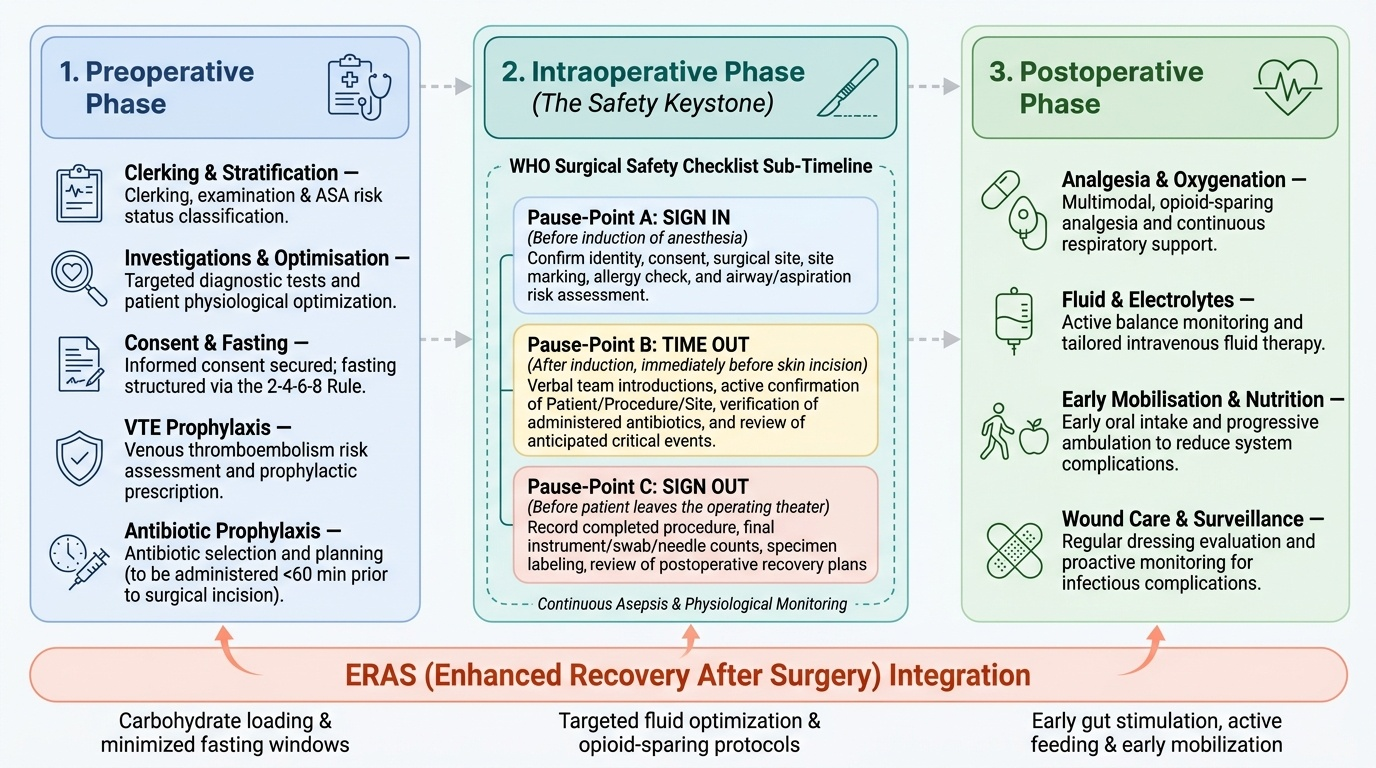
Applying the principles in order gives the perioperative sequence, which you should be able to walk through for any patient. In the preoperative phase, the patient is clerked and examined, risk-stratified by ASA status, investigated as appropriate, and optimised; informed consent is obtained and documented; fasting is ordered using the 2-4-6-8 rule; VTE risk is assessed and prophylaxis prescribed; and antibiotic prophylaxis is planned to fall within 60 minutes before incision. In the intraoperative phase, the keystone safety system is the WHO Surgical Safety Checklist, performed at three pause-points by the whole team. Sign In is done before induction of anaesthesia and confirms patient identity, the consented procedure and site, the marked site, allergies, airway and aspiration risk. Time Out is done after induction but immediately before skin incision: the team pauses, introduces themselves, and confirms aloud the patient, procedure, site, that prophylactic antibiotics have been given, and anticipated critical events. Sign Out is done before the patient leaves theatre and confirms the procedure recorded, the instrument, swab and needle counts, specimen labelling, and key recovery concerns. Around the checklist sit asepsis and continuous monitoring. In the postoperative phase, care focuses on analgesia (multimodal), oxygenation, fluid and electrolyte balance, early feeding and early mobilisation, wound care, and active surveillance for complications. The evidence-based protocol that ties all three phases together is ERAS (Enhanced Recovery After Surgery) — a multimodal pathway (carbohydrate loading, minimal fasting, opioid-sparing analgesia, early feeding and mobilisation, avoidance of routine drains and tubes) shown to shorten hospital stay and reduce complications.
Provided image
- Preoperative: clerk, risk-stratify (ASA), optimise, consent, fast (2-4-6-8), VTE prophylaxis, plan antibiotics.
- Intraoperative — WHO checklist: Sign In (before induction) → Time Out (before incision) → Sign Out (before leaving theatre); asepsis and monitoring throughout.
- Postoperative: analgesia, fluids, early feeding and mobilisation, wound care, complication surveillance — ERAS spans all three phases.