Page 1 of 11
SU8.1-3 | Surgical Ethics, Professionalism and Medico-Legal Practice — SDL Guide
Learning Objectives
- Describe the four principles of biomedical ethics and their operational derivatives — informed consent, confidentiality and truth-telling — as they apply to general surgery (SU8.1).
- Demonstrate the professional behaviours and empathic communication expected of a surgeon caring for a patient undergoing an operation (SU8.2).
- Discuss the principal medico-legal issues in surgical practice — negligence and the Bolam/Bolitho standard, valid consent in special situations, documentation, and the statutory backdrop (SU8.3).
INSTRUCTIONS
A surgeon can perform a technically flawless operation and still wrong the patient — by operating without a properly informed consent, by breaching a confidence, by lying about a complication, or by keeping a record so poor that no one can reconstruct what was done. Surgery, more than almost any other clinical activity, requires the deliberate violation of a person's bodily integrity, and that is only made lawful and ethical by consent, competence and good conduct. This module builds the ethical, professional and medico-legal foundation on which every later consent form, every difficult conversation and every operative record depends.
References
- Bailey & Love's Short Practice of Surgery, Ethics and the Surgeon / Medico-legal aspects chapters (textbook)
- SRB's Manual of Surgery, Medico-legal issues and consent in surgical practice (textbook)
- Sabiston Textbook of Surgery, Ethics in Surgery and the Surgeon-Patient Relationship (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 52-year-old woman is consented for a 'lump removal' from her breast and signs the form a few minutes before being wheeled in, mildly sedated, having been told only that 'it's nothing to worry about'. In theatre the lump proves malignant and the surgeon, acting in what he believes are her best interests, proceeds to a mastectomy she never discussed. The operation is technically perfect. She wakes to find a breast gone, a diagnosis she was never warned of, and a decision taken for her while she slept. Was anything done wrong? The scalpel never slipped — yet almost every ethical and legal safeguard that protects a surgical patient was. This module is about those safeguards: why they exist, and how a good surgeon honours them.
WHY THIS MATTERS
Ethics and medico-legal awareness are not an optional refinement bolted onto surgical skill — they are part of competent surgical practice itself. Surgery is the one branch of medicine in which we deliberately cut, remove and rearrange another person's body, so the duties of consent, honesty, confidentiality and care are sharper here than anywhere else. Get them right and your patients trust you, your team works openly, complications are disclosed and learned from, and the law leaves you alone. Get them wrong and the consequences are real: complaints, loss of trust, professional-conduct proceedings before the medical council, and civil claims for negligence under consumer-protection jurisdiction. Every consent conversation, every disclosure of a complication, every line in an operative note is simultaneously a clinical act and a legal one. Understanding the framework lets you act rightly by reason rather than by reflex, and protects both your patient and yourself.
RECALL
Before going further, recall three things you already know. First, the doctor-patient relationship is fiduciary — it is built on trust, and the balance of knowledge and power sits with the doctor, which is exactly why the patient needs protecting. Second, basic communication skills: listening, explaining in plain language, checking understanding, and responding to emotion are the everyday tools that turn an abstract principle such as 'autonomy' into a real conversation at the bedside. Third, that India has a body of law and professional regulation governing practice — the medical council's code of professional conduct, and statutes such as the Consumer Protection Act that bring medical services within consumer jurisdiction. Keep these three in mind: ethics tells you what you ought to do, professionalism is how you do it, and the law sets the enforceable floor beneath both.
Why Ethics and Professionalism Sit at the Centre of Surgery
The case above is unsettling precisely because the technical surgery was faultless — and yet the patient was wronged. This is the central lesson of surgical ethics: surgical excellence is necessary but not sufficient. Ethics is the systematic study of what we ought to do — the reasoned analysis of right and wrong conduct — while professionalism is the set of behaviours, attitudes and communication through which a surgeon actually lives out those obligations at the bedside. The two are not the same as the law: an action can be perfectly legal yet ethically wrong, and the law generally sets only the enforceable minimum. Surgery raises these questions with unusual force because the operation itself is, in law, a deliberate wounding that would be a criminal assault were it not authorised by a valid consent given by a patient who understands what is proposed. That single fact — that the surgeon's licence to cut comes entirely from the patient's informed permission — places autonomy, honesty and trust at the very centre of the discipline. The surgeon who masters the four principles, communicates with genuine empathy, and respects the legal framework does not merely avoid trouble; they practise better surgery, because openly consented, honestly disclosed and well-documented care is also safer care. This SDL works through the ethical principles first, then how they are operationalised in practice, and finally their medico-legal correlates.
Four Principles of Biomedical Ethics and Their Clinical Duties
The Four Principles and the Building Blocks of Surgical Ethics
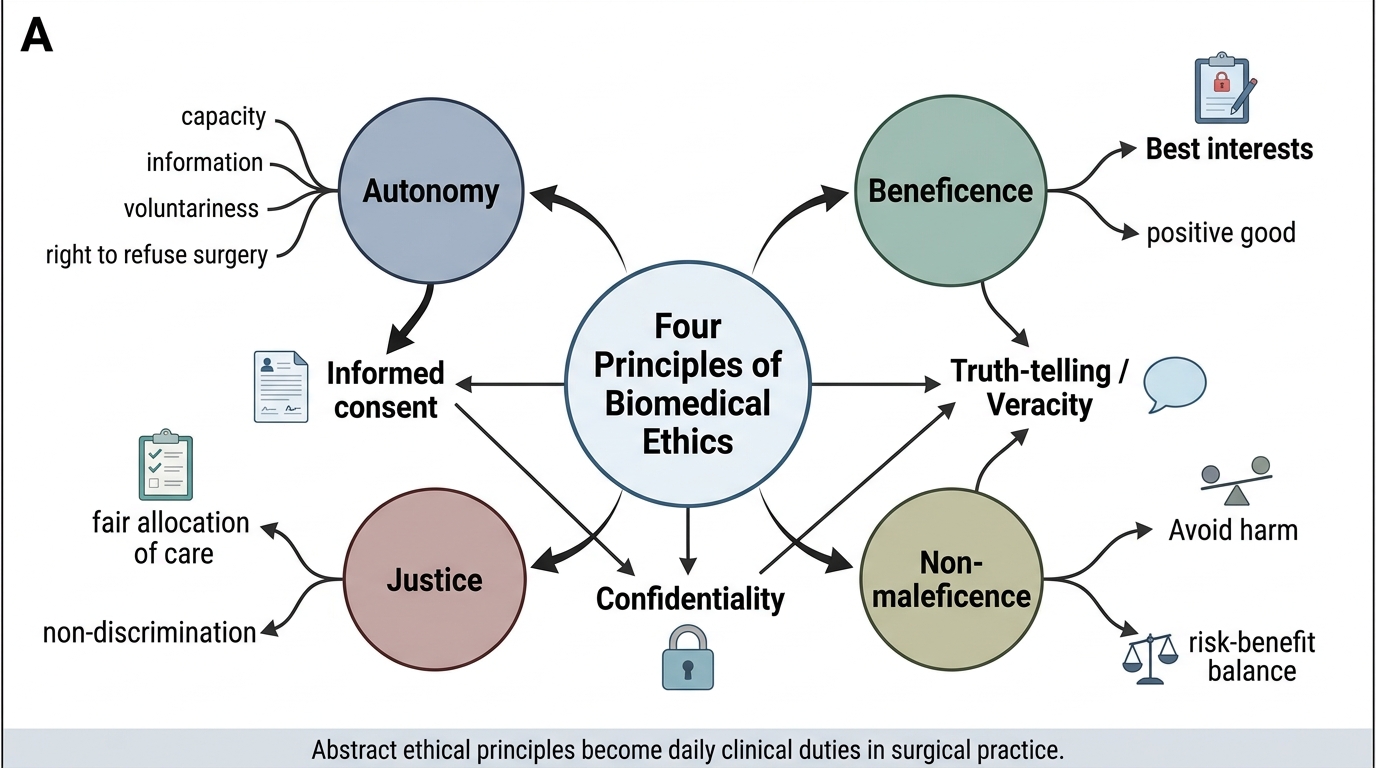
Modern biomedical ethics is most often taught through the four-principle framework popularised by Beauchamp and Childress, which gives a shared vocabulary for reasoning through any clinical dilemma. The first principle is autonomy — respect for the patient's right to make their own informed decisions about their body, including the right to refuse surgery even when refusal seems unwise. The second is beneficence — the duty to act in the patient's best interests, to do positive good. The third is non-maleficence — the duty to avoid causing harm, captured in the maxim primum non nocere; in surgery these two are in constant tension, since every operation does some harm (the wound) in pursuit of a greater good, which is why the risk-benefit balance must always favour the patient. The fourth is justice — fairness in the distribution of care and resources, treating like cases alike and not discriminating on irrelevant grounds. From these four flow the practical duties that dominate day-to-day surgery: informed consent is autonomy made operational; confidentiality protects the trust on which disclosure depends; and truth-telling (veracity) underpins both. These derivatives, not the abstract principles, are what a surgeon actually exercises at the bedside.
Provided image
- Autonomy: respect the patient's informed choices, including a competent refusal of surgery.
- Beneficence: act positively in the patient's best interests.
- Non-maleficence: avoid causing harm; weigh the risk-benefit balance of every operation.
- Justice: fair, non-discriminatory distribution of surgical care and resources.
- Operational derivatives: informed consent, confidentiality and truth-telling are how these principles are practised.
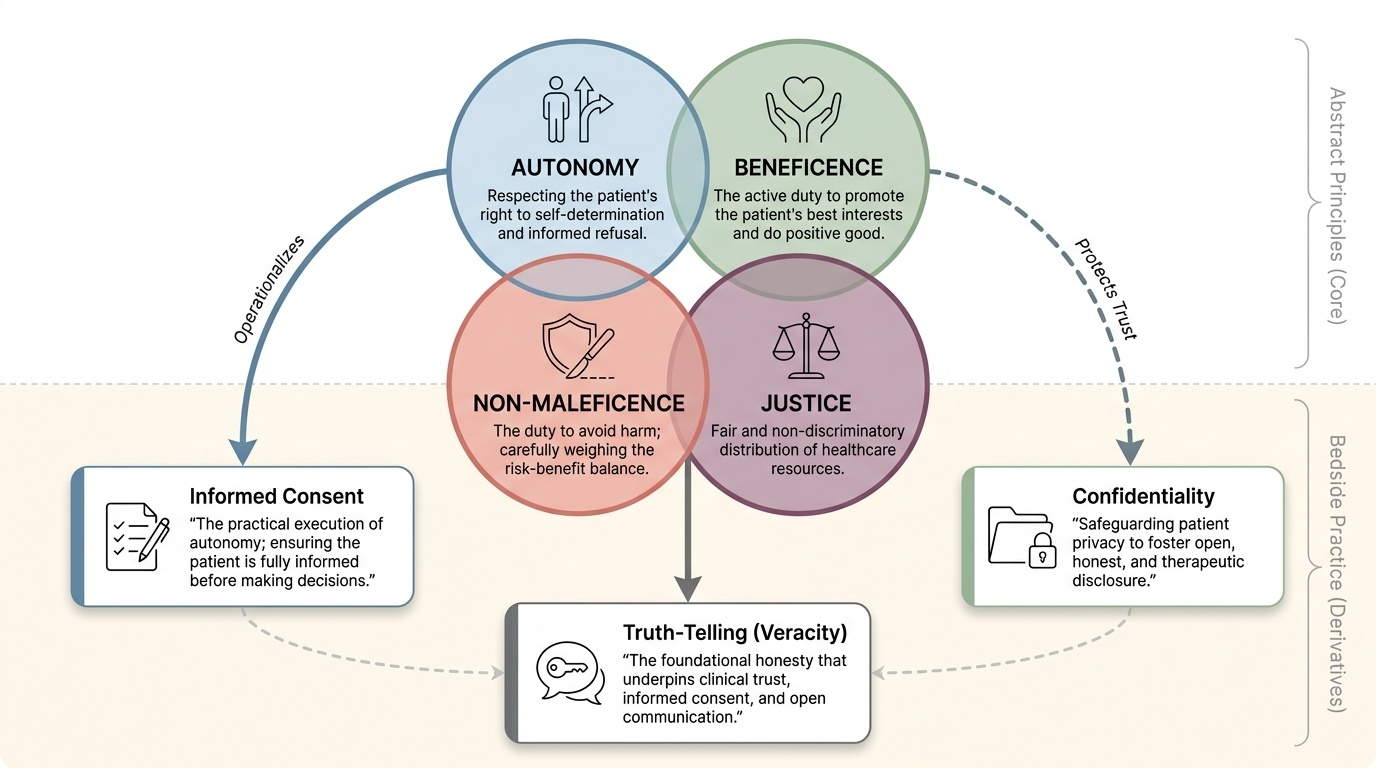
How the Principles Work in Practice: Consent, Confidentiality and Truth-telling
Principles only matter when they change what the surgeon does, so consider how each is operationalised. Informed consent is the practical expression of autonomy and is far more than a signature on a form: it is a process of shared decision-making. For consent to be valid the patient must have the capacity (competence) to decide, must be given adequate information — the nature and purpose of the operation, its material risks and benefits, and the reasonable alternatives including doing nothing — must actually understand that information, and must give the decision voluntarily, free from coercion, with the decision then documented. Consent obtained the moment before surgery, from a sedated patient, or for a different operation than the one performed, is not valid consent. Confidentiality is the duty to protect information disclosed within the clinical relationship; it sustains the trust that makes honest disclosure possible. It is strong but not absolute, and may be breached only for narrow, defensible reasons — with the patient's consent, where statute requires it (for example notification of certain diseases or of births and deaths), under a court order, or to protect an identifiable third party from serious harm. Truth-telling, including the empathic breaking of bad news and the honest disclosure of complications, completes the triad: a surgeon who hides a complication betrays both veracity and the patient's autonomy to make further decisions. Doing all of this with genuine empathy — unhurried explanation, attention to fear, and respect for the person — is what professionalism looks like in practice.
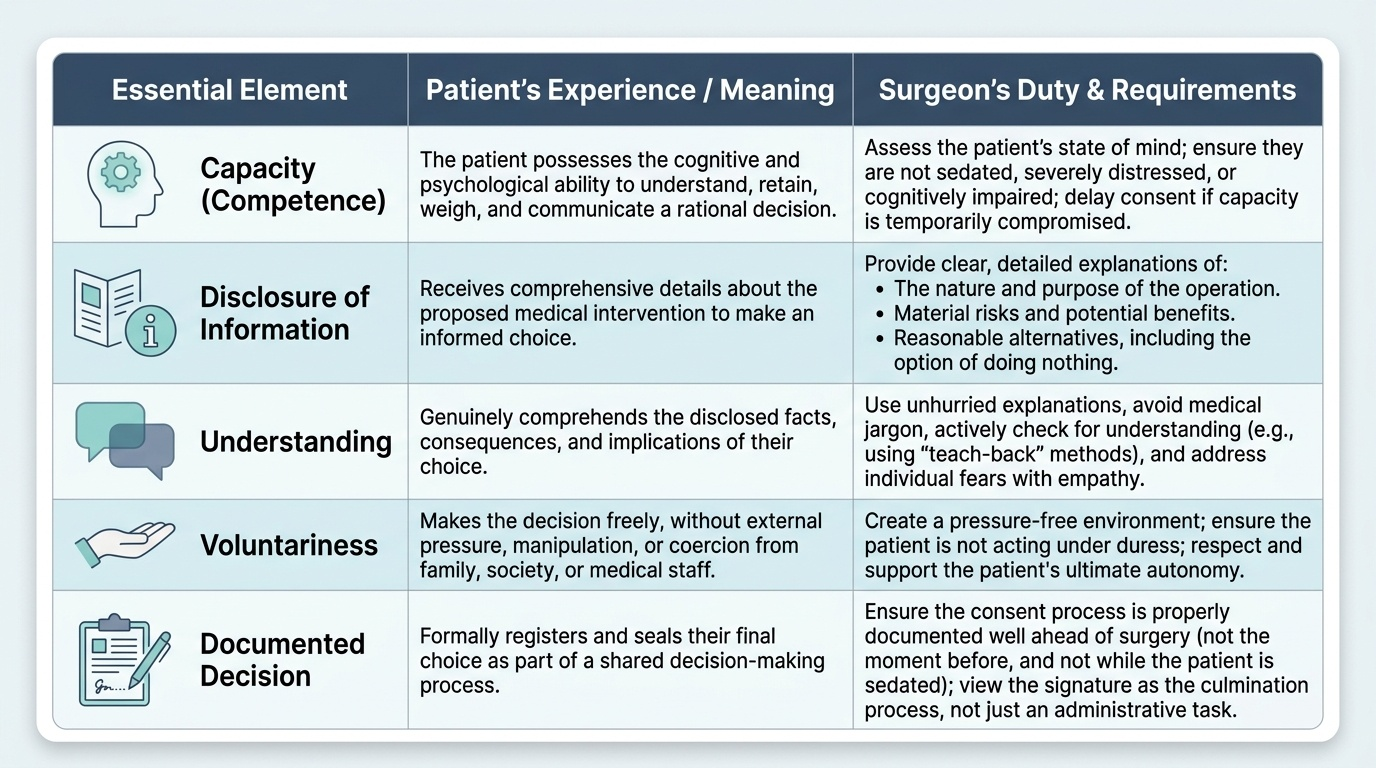
Provided image
| Element of valid consent | What the surgeon must ensure |
|---|---|
| Capacity (competence) | The patient can understand, retain, weigh and communicate a decision; assess it, do not assume it. |
| Disclosure of information | Nature and purpose of the operation, material risks and benefits, and the reasonable alternatives including no treatment. |
| Understanding | The patient has actually grasped the information — check, invite questions, use plain language. |
| Voluntariness | The decision is free of coercion or undue pressure from staff or family. |
| Documented decision | The consent (or refusal) is recorded; the form documents a process, it is not the process itself. |
SELF-CHECK
A competent, fully informed adult refuses a recommended life-saving emergency laparotomy, understanding that she may die without it. Which ethical principle most directly obliges the surgeon to respect this refusal?
A. Beneficence
B. Non-maleficence
C. Autonomy
D. Justice
Reveal Answer
Answer: C. Autonomy
Autonomy is the patient's right to make her own informed decisions about her body, including the right to refuse treatment a doctor judges to be in her interest. A competent, informed and voluntary refusal must be respected even when the surgeon believes beneficence points the other way; overriding it would be battery.