Page 1 of 8
MI11.1-3 | Antimicrobial Resistance & Antimicrobial Stewardship — SDL Guide
Learning Objectives
- Describe the genotypic and phenotypic mechanisms of antimicrobial drug resistance and the methods of antimicrobial susceptibility testing (AST), including interpretation of AST reports.
- Explain intrinsic and acquired drug resistance, the antimicrobial spectrum of important human pathogens, and the application of this knowledge in clinical therapy.
- Explain the concept and application of the Antimicrobial Stewardship Programme (AMSP), including rational antimicrobial prescription and your role in implementing stewardship.
INSTRUCTIONS
Antimicrobial resistance (AMR) is not a future threat — it is India's present clinical reality. Every day, patients in Indian hospitals die from infections caused by organisms resistant to every available antibiotic. Yet the same hospitals continue to over-prescribe, under-dose, and fail to de-escalate antibiotics. This module equips you with the science to understand resistance, the skill to read a susceptibility report, and the professional responsibility to be part of the solution through stewardship. This is the most consequential topic in clinical microbiology for your future prescribing practice.
References
- Ananthanarayan & Paniker's Textbook of Microbiology, 10th ed., Ch 51–52 (textbook)
- Mandell, Douglas & Bennett's Principles and Practice of Infectious Diseases, 9th ed., Ch 17–18 (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
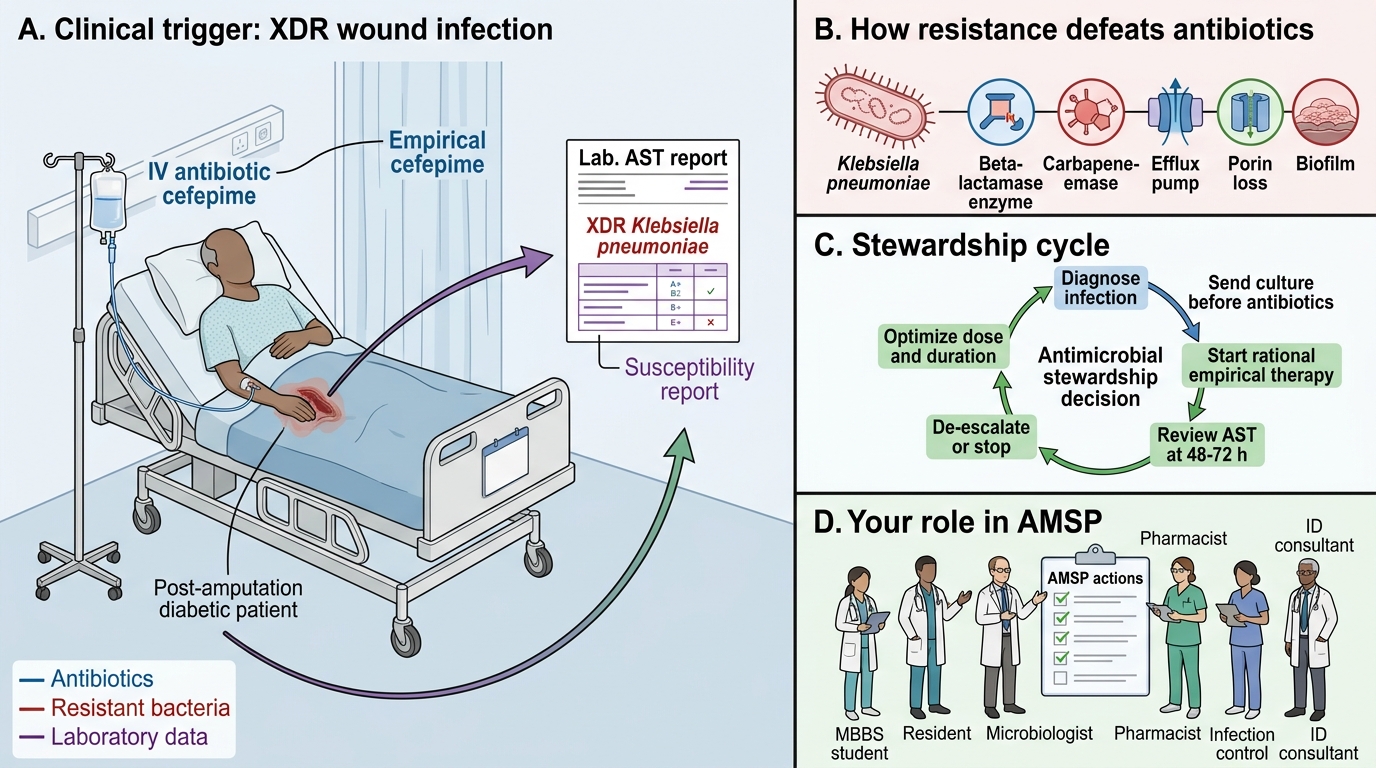
Ward 7, a tertiary government hospital in Chennai. A 55-year-old diabetic man post-amputation has a wound infection that is not responding to cefepime. The AST report arrives: XDR Klebsiella pneumoniae — resistant to all beta-lactams, carbapenems, fluoroquinolones, aminoglycosides, and colistin. The infectious disease consultant reads the report and says: 'We have nothing left.'
This is not a science fiction scenario. The Chennai hospital network reported the first fully pan-drug-resistant Klebsiella cluster in India in 2017. Understanding how we arrived here — and how to prevent repeating it — begins with understanding AMR mechanisms.
WHY THIS MATTERS
India is the world's largest consumer of antibiotics and faces one of the highest burdens of drug-resistant infections. An estimated 58,000 neonatal deaths per year in India are attributable to sepsis caused by drug-resistant organisms. As a prescribing clinician, every antibiotic order you write either contributes to this problem or helps control it. This module is foundational to your role as both a clinician and a public health actor.
RECALL
From General Microbiology I and Pharmacology:
- Mechanisms of action of major antibiotic classes (cell wall synthesis inhibitors, protein synthesis inhibitors, DNA gyrase inhibitors, membrane disruptors)
- Beta-lactam ring structure and penicillin-binding proteins (PBPs)
- Bacterial cell wall structure — gram-positive vs gram-negative
From Biochemistry:
- Enzyme inhibition: competitive and non-competitive
- Efflux pumps and membrane transport proteins
- Gene expression: transcription, translation, mutation
Mechanisms of Antimicrobial Resistance
Intrinsic Mechanisms of Antimicrobial Resistance
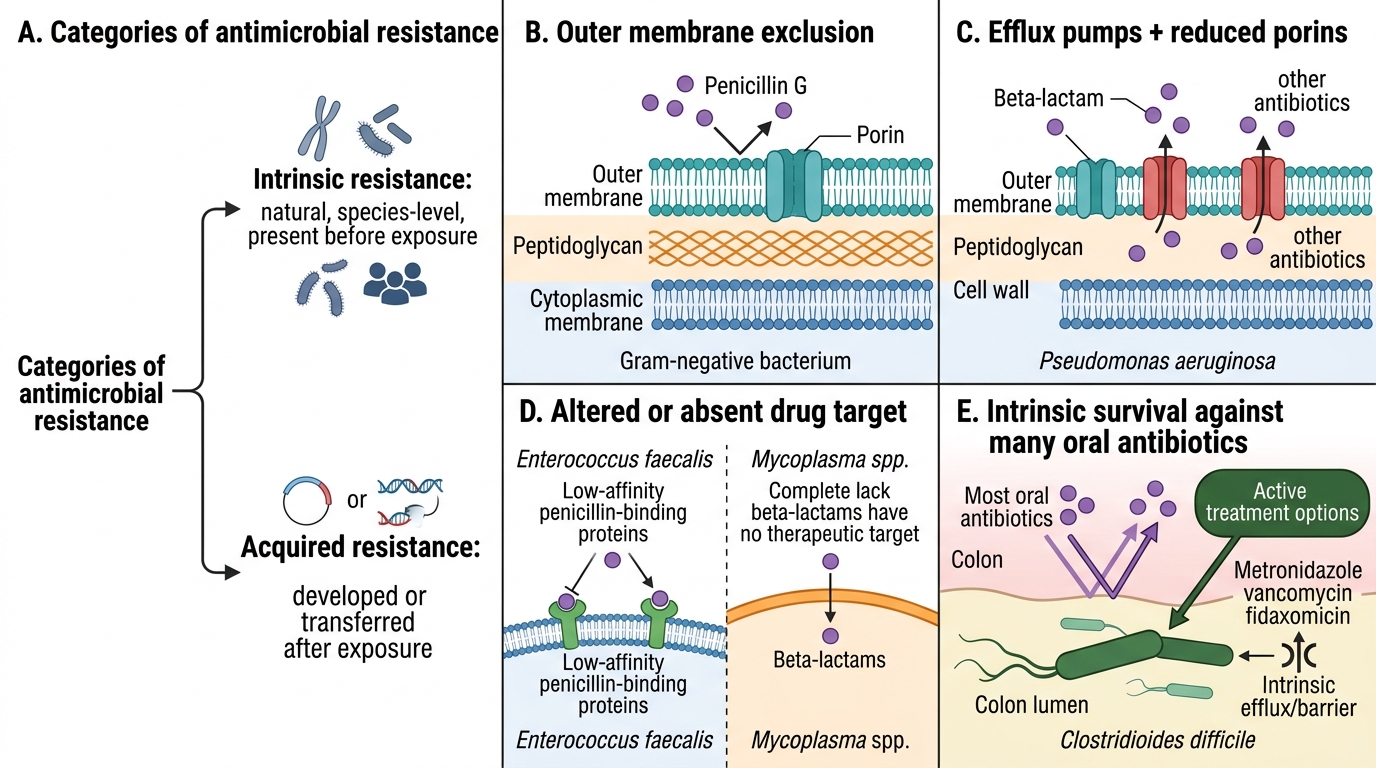
Resistance mechanisms fall into two broad categories: intrinsic (natural, species-level) and acquired (developed or transferred).
A. Intrinsic Resistance
Intrinsic resistance is an inherent property of the species — present before any antibiotic exposure.
| Organism | Intrinsic Resistance | Mechanism |
|---|---|---|
| Gram-negatives | Penicillin G | Outer membrane excludes hydrophobic penicillin G |
| Pseudomonas aeruginosa | Most beta-lactams, many antibiotics | Multiple efflux pumps + reduced porins |
| Enterococcus faecalis | Cephalosporins | Low affinity PBPs |
| Mycoplasma spp. | Beta-lactams | No cell wall |
| Clostridium difficile | Most oral antibiotics (except metronidazole, vancomycin, fidaxomicin) | Intrinsic efflux |
Intrinsic resistance is predictable — if you know the organism, you know certain antibiotics will not work without needing an AST.
B. Acquired Resistance: Genotypic Mechanisms
1. Mutation (vertical transmission)
Spontaneous point mutations in chromosomal genes alter drug targets or expression of transport proteins:
- rpoB mutation in M. tuberculosis → rifampicin resistance (detectable by GeneXpert)
- gyrA/parC mutations → fluoroquinolone resistance (quinolone-resistance determining region, QRDR)
- katG mutation → isoniazid resistance (loss of enzyme that activates isoniazid pro-drug)
Mutation-based resistance is clonal — it cannot jump to other species.
2. Horizontal Gene Transfer (HGT) (lateral spread — clinically critical)
Resistance genes transfer between organisms via three mechanisms:
- Conjugation: direct cell-to-cell plasmid transfer through a sex pilus — the most clinically important HGT mechanism. NDM-1 (New Delhi Metallo-beta-lactamase) and MCR (colistin resistance) are plasmid-borne and spread this way across unrelated species in ICUs.
- Transduction: bacteriophage carries resistance gene from donor to recipient — important in Staphylococci
- Transformation: uptake of free DNA from environment — important in Streptococcus pneumoniae (PBP gene mosaics causing penicillin resistance)
Mobile genetic elements that carry resistance genes:
- Plasmids: self-replicating circular DNA; carry multiple resistance genes simultaneously
- Transposons ('jumping genes'): move resistance genes within and between replicons
- Integrons: capture gene cassettes from the environment; may carry 5–10 resistance genes in one integron

Conjugative Transfer of NDM-1 Carbapenem Resistance
C. Acquired Resistance: Phenotypic Mechanisms
1. Enzymatic inactivation of the antibiotic
- Beta-lactamases: hydrolyse the beta-lactam ring, inactivating penicillins, cephalosporins, monobactams, carbapenems
- ESBLs (Extended-Spectrum Beta-Lactamases): produced by E. coli, Klebsiella — hydrolyse all penicillins and cephalosporins; inhibited by tazobactam/clavulanate; NOT carbapenems
- Carbapenemases (MBL, KPC, OXA): hydrolyse carbapenems — the last-resort antibiotics
- NDM-1 (Metallo-beta-lactamase): NOT inhibited by tazobactam; requires zinc co-factor
- KPC (Klebsiella pneumoniae Carbapenemase): inhibited by new beta-lactam/BLI combinations (ceftazidime-avibactam)
- OXA-48: requires ceftazidime-avibactam
- Aminoglycoside-modifying enzymes (AMEs): acetylation, phosphorylation, adenylation — inactivate gentamicin, amikacin
- Chloramphenicol acetyltransferase (CAT): inactivates chloramphenicol
2. Alteration of drug target
- MRSA (Methicillin-Resistant Staphylococcus aureus): mecA gene encodes PBP2a — a new penicillin-binding protein with very low affinity for all beta-lactams; entire class becomes ineffective
- VRE (Vancomycin-Resistant Enterococcus): vanA gene cluster alters peptidoglycan terminus from D-Ala-D-Ala to D-Ala-D-Lac — vancomycin cannot bind
- Rifampicin resistance: rpoB mutation alters RNA polymerase binding site
3. Efflux pumps
Membrane transporter proteins actively pump antibiotics out of the bacterial cell before they can reach their target.
- MexAB-OprM in Pseudomonas: broad-spectrum; expels beta-lactams, fluoroquinolones, macrolides
- AcrAB-TolC in Enterobacteriaceae: expels tetracyclines, fluoroquinolones, macrolides
- Efflux pump overexpression often contributes to low-level resistance, creating a stepping stone to higher-level resistance through additional mutations
4. Reduced permeability (porin loss)
Gram-negative bacteria regulate entry of hydrophilic antibiotics through outer membrane porin channels (OmpF, OmpC). Loss or mutation of porins reduces intracellular antibiotic concentration.
- Loss of OprD in Pseudomonas: reduced carbapenem uptake (imipenem resistance without carbapenemase)
- Combined porin loss + efflux upregulation = synergistic resistance amplification
5. Target bypass / overproduction
- DHFR overproduction (trimethoprim resistance): excess enzyme overwhelms inhibition
- Alternative pathway: MRSA expresses PBP2a (encoded by mecA) as a bypass to blocked PBPs
CLINICAL PEARL
The ESKAPE pathogens — Enterococcus faecium, Staphylococcus aureus, Klebsiella pneumoniae, Acinetobacter baumannii, Pseudomonas aeruginosa, Enterobacter spp. — 'escape' the effects of most antibiotics via multiple simultaneous mechanisms and account for the majority of hospital-acquired drug-resistant infections globally. Recognising their names and resistance profiles is a foundational clinical skill.
Antimicrobial Susceptibility Testing (AST)
Disk Diffusion AST and Breakpoint Interpretation
AST determines whether a specific pathogen is susceptible or resistant to a specific antibiotic, guiding targeted therapy.
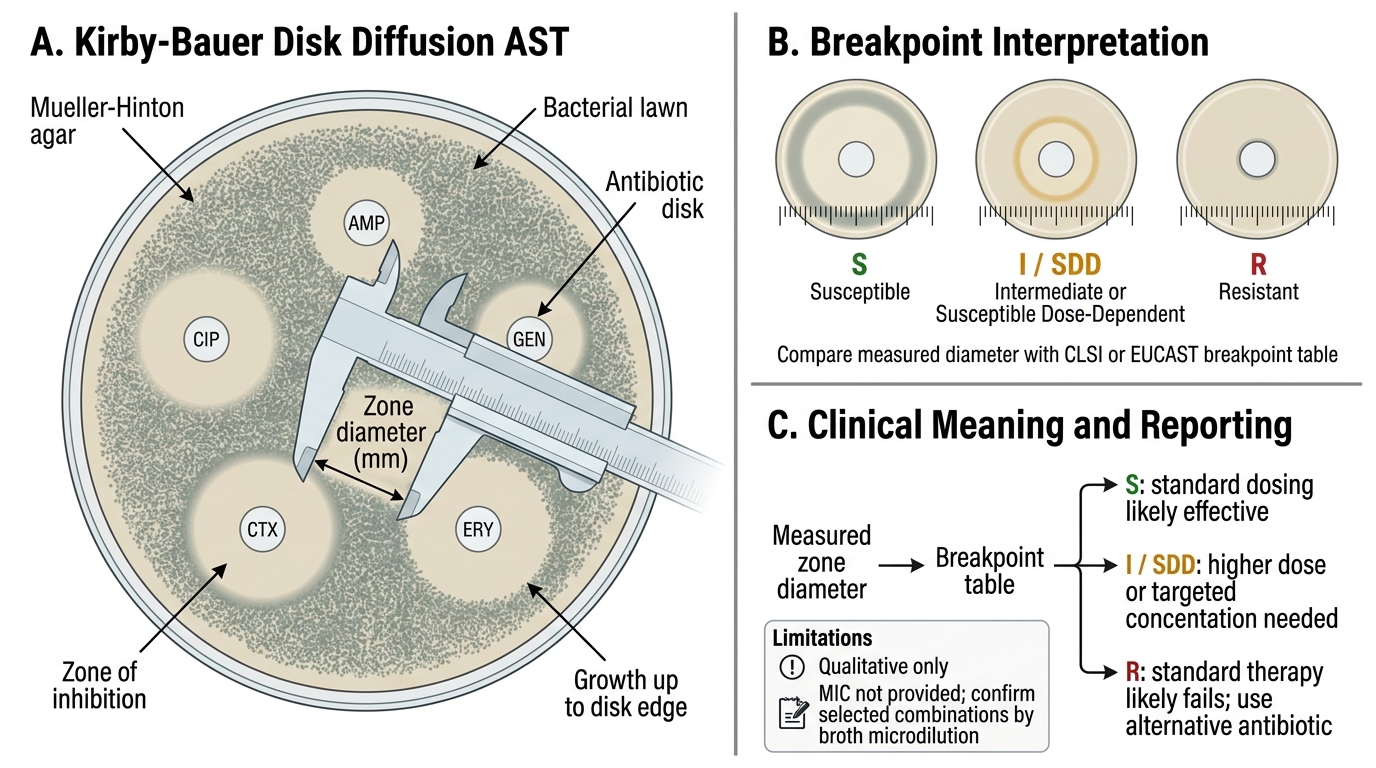
1. Disk Diffusion (Kirby-Bauer method)
Antibiotic-impregnated disks are placed on Mueller-Hinton agar inoculated with the test organism. Antibiotic diffuses outward; a clear zone of inhibition appears where growth is suppressed. Zone diameter is measured and compared to CLSI or EUCAST breakpoints.
Result interpretation:
- S (Susceptible): Standard dosing likely to achieve therapeutic levels at the site of infection
- I (Intermediate) or SDD (Susceptible Dose-Dependent): Higher dose or targeted drug concentration needed; indicates borderline
- R (Resistant): Standard therapy will fail; alternate antibiotic required
Advantages: Inexpensive, simple, widely available in Indian district hospitals
Limitations: Qualitative; does not give MIC; some organism-antibiotic combinations require broth microdilution confirmation

Disk Diffusion AST and CLSI Breakpoint Interpretation
2. Broth Microdilution (BMD) — Gold Standard for MIC
Serial doubling dilutions of antibiotic in broth, each inoculated with standardised bacterial suspension. The MIC is the lowest concentration showing no visible turbidity.
MIC interpretation (using CLSI 2024 breakpoints):
- MIC ≤ S breakpoint → Susceptible
- MIC ≥ R breakpoint → Resistant
Clinical relevance: MIC allows pharmacokinetic/pharmacodynamic (PK/PD) target attainment — e.g., for a pathogen with MIC 2 mg/L, can standard meropenem dose achieve free drug concentration >4× MIC at the infection site?
3. E-test (Epsilometer Test)
A plastic strip impregnated with an antibiotic gradient placed on agar. The intersection of the elliptical inhibition zone with the MIC scale reads a precise MIC. Useful for slow-growing organisms (pneumococcus, Haemophilus) and confirmation of borderline results.
4. Automated systems (VITEK 2, BD Phoenix, Microscan)
Fluorescence-based detection of bacterial growth in miniaturised broth microdilution panels. Provides complete AST with MIC values in 4–8 h; standardised and reproducible. Standard of care in accredited Indian hospital laboratories.
5. Molecular resistance detection
- PCR/real-time PCR: rapid detection of specific resistance genes (mecA for MRSA, blaNDM for NDM-1, vanA/B for VRE)
- Does not replace phenotypic AST for full susceptibility profile but provides faster actionable data for high-priority targets
- GeneXpert Ultra: rpoB for rifampicin resistance in MTB
Reading an AST Report — Practical Guide
| Column | What it means |
|---|---|
| Antibiotic name | Tested drug |
| MIC (µg/mL) | Measured inhibitory concentration |
| Interpretation (S/I/R) | Based on CLSI/EUCAST breakpoints for species-drug-infection site combination |
| Comments | e.g., 'ESBL detected — report all penicillins, cephalosporins, and aztreonam as Resistant' |
CLSI phenotypic rules (selective reporting / cascade reporting):
An ESBL-producing isolate may appear susceptible to cephalosporins by disk but will fail in vivo — CLSI mandates reporting all cephalosporins as R when ESBL is confirmed. Always read the comments column.
Critical values requiring immediate clinician notification:
- Blood/CSF culture isolate with carbapenem R
- Any isolate with colistin MIC ≥4 µg/mL (potential PDR)
- MRSA from a sterile site
- VRE from blood culture
SELF-CHECK
An AST report on a urine isolate of E. coli shows: Cefotaxime MIC 32 µg/mL (R), Meropenem MIC 0.25 µg/mL (S), ESBL detected. The clinician wants to use cefotaxime because 'the MIC is only 32 and the patient was responding.' What is the correct microbiological response?
A. Agree — MIC 32 µg/mL is achievable with high-dose cefotaxime in urine
B. Advise against cefotaxime — ESBL producers must have all cephalosporins reported as Resistant regardless of MIC by CLSI rules, and clinical failure is documented
C. Request repeat culture — the ESBL result may be a laboratory error
D. Suggest adding clavulanate to the cefotaxime to overcome ESBL
Reveal Answer
Answer: B. Advise against cefotaxime — ESBL producers must have all cephalosporins reported as Resistant regardless of MIC by CLSI rules, and clinical failure is documented
CLSI mandates that ESBL-producing isolates have all penicillins, cephalosporins, and aztreonam reported as Resistant regardless of in vitro MIC, because in vivo clinical failure with cephalosporins is documented even when in vitro MICs appear low (an inoculum effect and pharmacodynamic failure). Meropenem is the correct choice for systemic ESBL infections. Beta-lactam/BLI combinations (e.g., piperacillin-tazobactam) have variable reliability for ESBL infections — not standard recommendation. Adding clavulanate to cefotaxime is not a licensed or validated approach.
Intrinsic vs Acquired Resistance & Antibiotic Spectrum of Key Pathogens
Provided image
MI11.2 — Applied resistance and spectrum knowledge
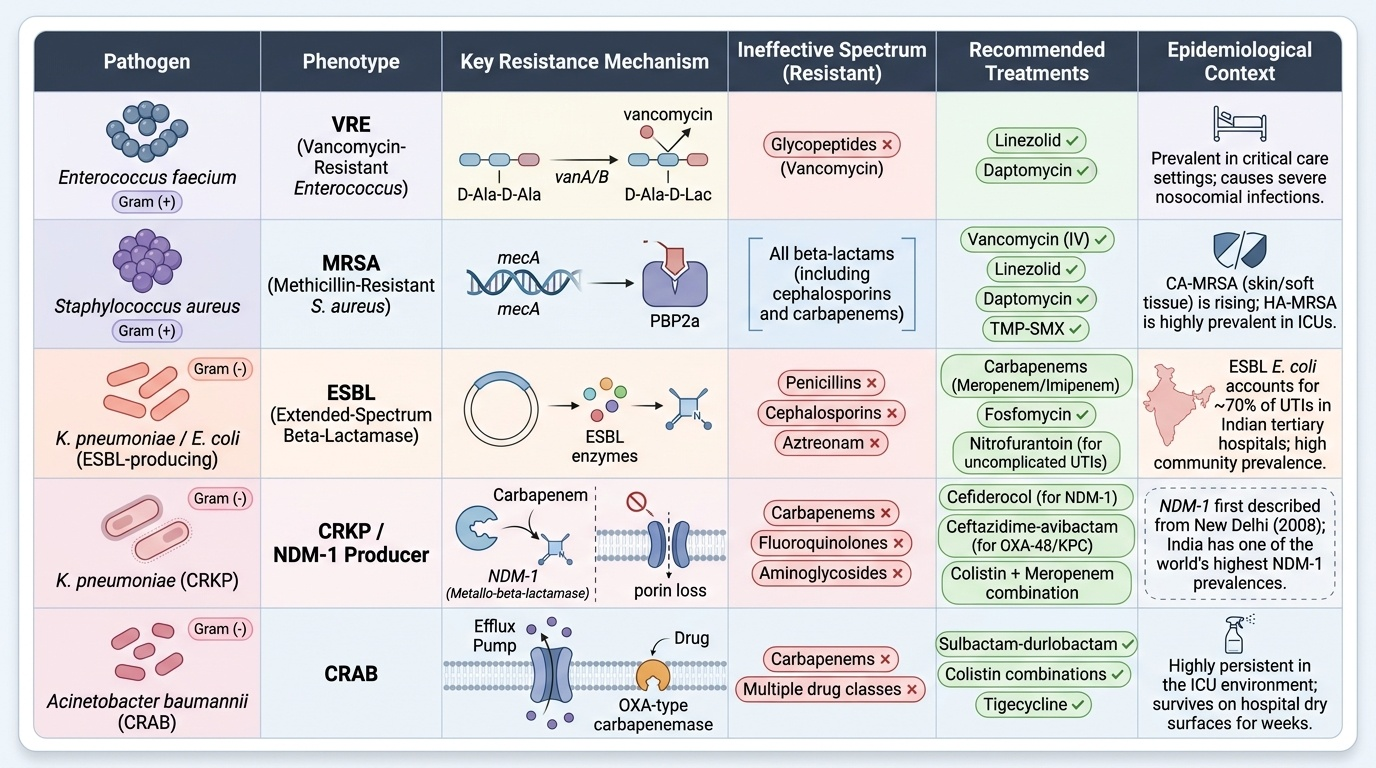
Clinically important resistance phenotypes and their implications:
MRSA (Methicillin-Resistant Staphylococcus aureus)
- Mechanism: mecA gene → PBP2a (low affinity for all beta-lactams)
- Spectrum: Resistant to ALL beta-lactams (including cephalosporins, carbapenems)
- Treatment: Vancomycin (IV, for serious infections); Linezolid (alternative); Daptomycin (non-pulmonary); Trimethoprim-sulfamethoxazole (skin/soft tissue only)
- Indian context: CA-MRSA (community-acquired) presenting as furuncles/skin infections is increasing; HA-MRSA (healthcare-associated) in ICUs is prevalent
ESBL-producing E. coli and Klebsiella pneumoniae
- Mechanism: Plasmid-encoded ESBLs hydrolyse extended-spectrum cephalosporins
- Spectrum: R to all penicillins + cephalosporins + aztreonam; S to carbapenems, aminoglycosides (often), fosfomycin (UTI)
- Treatment: Meropenem/Imipenem for systemic infection; Fosfomycin/Nitrofurantoin for uncomplicated ESBL UTI
- Indian context: ESBL E. coli accounts for ~70% of E. coli UTIs in tertiary Indian hospitals — this is now de facto community prevalence in urban India
Carbapenem-Resistant Klebsiella pneumoniae (CRKP) / NDM-1 producers
- Mechanism: NDM-1 (MBL) + porin loss
- Spectrum: R to carbapenems; often co-resistant to fluoroquinolones, aminoglycosides, colistin
- Treatment: Ceftazidime-avibactam (if OXA-48 or KPC; NOT NDM-1!); Cefiderocol (NDM-1); Colistin + meropenem combination; Fosfomycin combinations
- Indian context: NDM-1 was first described from a Swedish patient treated in New Delhi (2008); India has one of the world's highest NDM-1 prevalences
Carbapenem-Resistant Acinetobacter baumannii (CRAB)
- Mechanism: OXA-type carbapenemases + efflux + porin loss
- Treatment: Sulbactam-durlobactam (new); Colistin-based combinations; Tigecycline
- Indian context: Common in burns units and ICUs; environmental survival allows ward contamination for weeks
VRE (Vancomycin-Resistant Enterococcus)
- Mechanism: vanA/B gene cluster → D-Ala-D-Lac peptidoglycan
- Treatment: Linezolid; Daptomycin
MDR Mycobacterium tuberculosis (MDR-TB)
- MDR-TB: R to rifampicin + isoniazid (at minimum)
- XDR-TB (pre-2021 definition): MDR + fluoroquinolone + injectable
- Current WHO XDR-TB definition (2021): MDR + fluoroquinolone + any additional Group C drug
- Treatment: All-oral regimens (BPaL — Bedaquiline + Pretomanid + Linezolid); 6–9 months
- Indian context: India has second highest MDR-TB burden globally after China; NTEP provides free MDR-TB treatment
CLINICAL PEARL
'Pradofloxacin-resistant E. coli in a 25-year-old woman's UTI, no carbapenem!' For uncomplicated ESBL UTIs, many clinicians reflexively reach for carbapenems — this is carbapenem over-use and drives resistance. Current IDSA/ICMR guidance supports oral fosfomycin or nitrofurantoin for uncomplicated lower UTI caused by ESBL E. coli (when susceptible) — preserving carbapenems for complicated, systemic, or high-MIC infections. Know the difference between treating pyelonephritis (IV carbapenem) and simple cystitis (oral fosfomycin).
Antimicrobial Stewardship Programme (AMSP)
Antimicrobial Stewardship Programme: From AST Report to Responsible Action
MI11.3 — Concept, application, and your role in AMSP
Definition: An AMSP is a coordinated, systematic set of strategies to optimise antimicrobial use — ensuring patients receive the right drug, at the right dose, by the right route, for the right duration — while minimising selection pressure for resistance, adverse drug events, and Clostridioides difficile infection.
Why AMSP?
Antibiotic misuse patterns in India:
- Empirical broad-spectrum therapy continued beyond 48–72 h without culture results
- Failure to de-escalate when narrow-spectrum options are available
- Over-use of carbapenems for community-acquired infections where extended-spectrum cephalosporins are sufficient
- Inadequate duration knowledge (3 days for uncomplicated UTI; 5 days for community pneumonia; 2 weeks for bacteraemia, not indefinitely)
Core AMSP strategies:
1. Prospective audit and feedback (PAF)
ASP pharmacist or ID physician reviews antibiotic prescriptions prospectively and provides real-time feedback to the prescribing team. Most evidence-based and cost-effective strategy.
2. Formulary restriction and pre-authorisation
Designated 'restricted' antibiotics (carbapenems, colistin, linezolid, ceftazidime-avibactam) require approval from an ID physician or ASP team before dispensing. Reduces over-use of last-resort agents.
3. De-escalation
Switch from empirical broad-spectrum therapy to targeted narrow-spectrum therapy once culture and AST results are available (typically at 48–72 h). Requires culture data — which is why specimen collection is the foundation of stewardship.
4. IV-to-oral switch
Convert from intravenous to oral antibiotic when:
- Patient is clinically improving
- Able to absorb oral medications
- Oral formulation with good bioavailability exists (fluoroquinolones, metronidazole, co-trimoxazole achieve near-identical serum levels orally)
Reduces duration of hospitalisation, line-related infections, and costs.
5. Optimising duration (time-out)
A 48–72-hour mandatory 'time-out' review of every antibiotic prescription to:
- Confirm ongoing indication
- Review culture results and de-escalate
- Set a clear stop date
6. Rapid diagnostics integration
Faster results → faster de-escalation. MALDI-TOF provides species ID in hours; GeneXpert in 2 h. Blood culture positivity flagging with direct-from-bottle sensitivity testing reduces time to optimal therapy.
7. Biomarker-guided therapy
- Procalcitonin (PCT): elevated in bacterial sepsis, low in viral infections; serial PCT-guided antibiotic duration protocols reduce treatment duration in CAP and sepsis without worsening outcomes
- C-reactive protein (CRP): less specific but widely available in India
Indian AMSP context:
- National Action Plan on AMR (NAP-AMR) 2017–2021 (now 2022–2025): India's multi-sectoral national strategy, coordinated by MoHFW, ICMR, ICAR, and MoEFCC
- ICMR AMR surveillance network: tracks resistance trends at sentinel sites across India; publishes annual 'Treatment Guidelines for Antimicrobial Use'
- NABH accreditation: requires hospitals to have a functional Antibiotic Policy and AMSP
- Hospital Infection Control Committee (HICC): mandated by MoHFW; includes the AMSP within its remit
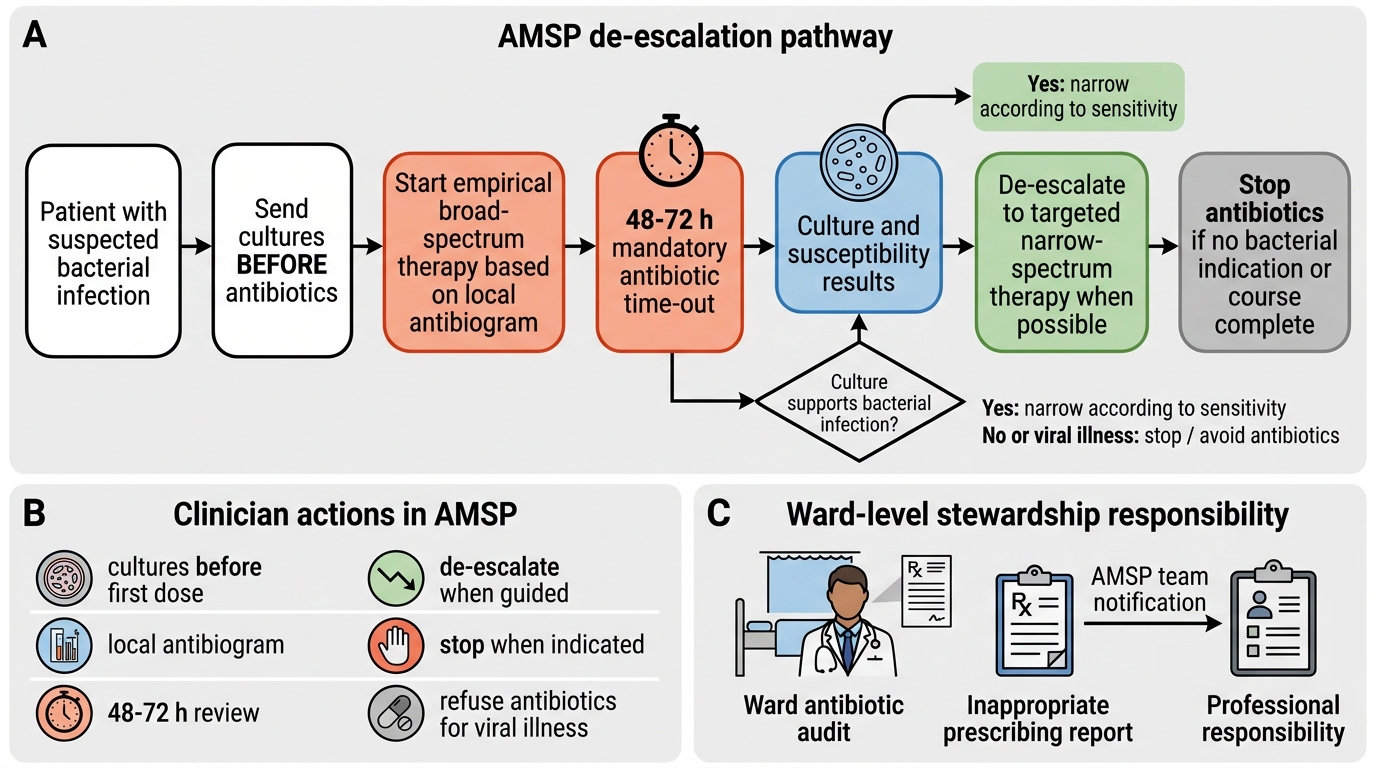
AMSP De-escalation Pathway After 48-72 Hour Culture Review
Your role as a clinician in AMSP:
| Action | When |
|---|---|
| Send cultures BEFORE antibiotics | Always — before every first dose |
| Select empirical therapy based on local antibiogram | Always — know your hospital's resistance data |
| Review culture results at 48–72 h | Mandatory 'time-out' |
| De-escalate if narrow-spectrum option is available | When culture guides narrow therapy |
| Stop antibiotics when indicated | Completion of course; afebrile, improving |
| Refuse patient demand for antibiotics for viral illness | Every cold, every throat pain |
| Participate in ward-level antibiotic audits | As a resident and consultant |
| Report to AMSP team when you observe inappropriate prescribing | Professional and ethical responsibility |
SELF-CHECK
A patient admitted with community-acquired pneumonia (CAP) is started on ceftriaxone. Blood and sputum cultures are negative at 72 hours. The patient has improved: afebrile for 48 h, CRP falling, tolerating oral intake. What is the most appropriate AMSP-consistent action?
A. Continue IV ceftriaxone for a total of 10 days as per traditional pneumonia treatment
B. Switch to oral amoxicillin-clavulanate and discharge with 5 days total antibiotic duration (IV + oral)
C. Escalate to piperacillin-tazobactam as culture was negative (suggesting resistant organism)
D. Continue IV antibiotics until fully asymptomatic to prevent relapse
Reveal Answer
Answer: B. Switch to oral amoxicillin-clavulanate and discharge with 5 days total antibiotic duration (IV + oral)
IDSA/ATS guidelines and AMSP principles support IV-to-oral switch when clinical stability criteria are met (afebrile ≥48 h, improving, oral toleration) and oral antibiotic therapy for a total course of 5 days in non-severe CAP. Negative cultures in CAP are common (50–70% of cases) and do not indicate resistance — empirical ceftriaxone coverage for typical bacteria is appropriate. Extended IV therapy prolongs hospitalisation, increases costs, and increases catheter-related complications. Escalation is contraindicated when the patient is improving.
REFLECT
You are a junior resident in a ward where carbapenems are prescribed 'just to be safe' for every febrile patient with a positive urine culture — regardless of organism sensitivity or clinical severity. When you suggest de-escalating a patient's meropenem to oral co-trimoxazole (the isolate is trimethoprim-susceptible, patient is afebrile and improving), your senior dismisses you: 'Don't take chances — this is a teaching hospital, not a PHC.'
- What are the clinical and public health consequences of this prescribing culture?
- How would you, as a junior team member, escalate this concern through legitimate channels?
- What role can the AMSP team play in supporting you?
- Draft a 3-sentence evidence-based case for de-escalation you would present at the bedside.
This scenario reflects a real challenge: stewardship requires courage, not just knowledge.
KEY TAKEAWAYS
Key takeaways:
- Resistance mechanisms are biochemically specific — beta-lactamases hydrolyse the ring; PBP2a in MRSA bypasses the target; efflux pumps expel the drug; porin loss reduces intracellular concentration. Knowing the mechanism predicts which alternatives will still work.
- Horizontal gene transfer (conjugation, transduction, transformation) drives the rapid spread of resistance across unrelated species — a single plasmid can carry NDM-1, ESBL, and aminoglycoside resistance simultaneously.
- AST report interpretation requires reading both MIC and interpretation columns AND the comments field — CLSI rules mandate reporting ESBL-producers' cephalosporins as Resistant regardless of measured MIC.
- Intrinsic resistance is predictable — if you know the organism (e.g., Pseudomonas), you know which drugs will not work without waiting for AST.
- AMSP = right drug, right dose, right route, right duration. Its core strategies — audit + feedback, de-escalation, IV-to-oral switch, time-out — save lives and preserve antibiotics for future generations.
- Your prescribing decisions have population-level consequences. Every unnecessary carbapenem prescription is a vote for the next NDR-TB or XDR-Klebsiella outbreak in your hospital. Culture before antibiotics, de-escalate at 72 h, stop at the evidence-based endpoint.