Page 7 of 14
MI3.9 | Infective Causes of Anaemia — SDL Guide
Learning Objectives
- Enumerate the common infective causes of anaemia
- Describe the mechanisms by which infections cause anaemia in each case
INSTRUCTIONS
Anaemia is one of the most common clinical findings in India — and infection is a frequently overlooked contributor. This focused session maps the major infective pathogens to their mechanisms of causing anaemia, equipping you to investigate and manage anaemia in a patient with concurrent or recent infection.
References
- Ananthanarayan & Paniker's Textbook of Microbiology, Ch 54 (Plasmodium), Ch 56 (Leishmania) (textbook)
- Harrison's Principles of Internal Medicine — Anaemia in Infectious Disease (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 7-year-old boy from Odisha is brought in with pallor, jaundice, and high fever for 4 days. Haemoglobin is 6.2 g/dL — severe anaemia. The peripheral smear shows ring forms and banana-shaped gametocytes inside red cells. Liver and spleen are enlarged. His mother says: "He never had anaemia before this fever."
This child did not develop anaemia from poor diet alone — an organism has commandeered his red blood cells and destroyed them at a rate his bone marrow cannot replace. The diagnosis is malignant malaria with severe haemolytic anaemia.
Infection-driven anaemia is common in India and often the most acute, life-threatening form a clinician will encounter. By the end of this session, you will enumerate the infective causes and explain their distinct mechanisms.
WHY THIS MATTERS
India has among the world's highest burdens of both anaemia and tropical infections. In a busy OPD in an endemic area, the majority of severe acute anaemias are infective in origin — malaria and hookworm being the commonest. A clinician who cannot distinguish infective from nutritional anaemia will miss treatable causes, delay correct therapy, and potentially transfuse unnecessarily. This topic bridges Microbiology with Medicine, Paediatrics, and Haematology.
RECALL
Before proceeding, recall:
- Haemolytic anaemia = red cell destruction faster than production; features include jaundice, reticulocytosis, elevated LDH, low haptoglobin
- Anaemia of chronic disease (ACD) = normocytic normochromic anaemia due to impaired iron utilisation and suppressed erythropoiesis — seen in any prolonged infection
- Normal haemoglobin: Men >13 g/dL, Women >12 g/dL, Children (6–14 years) >11.5 g/dL
Classification of Infective Causes of Anaemia
Classification of Infective Causes of Anaemia
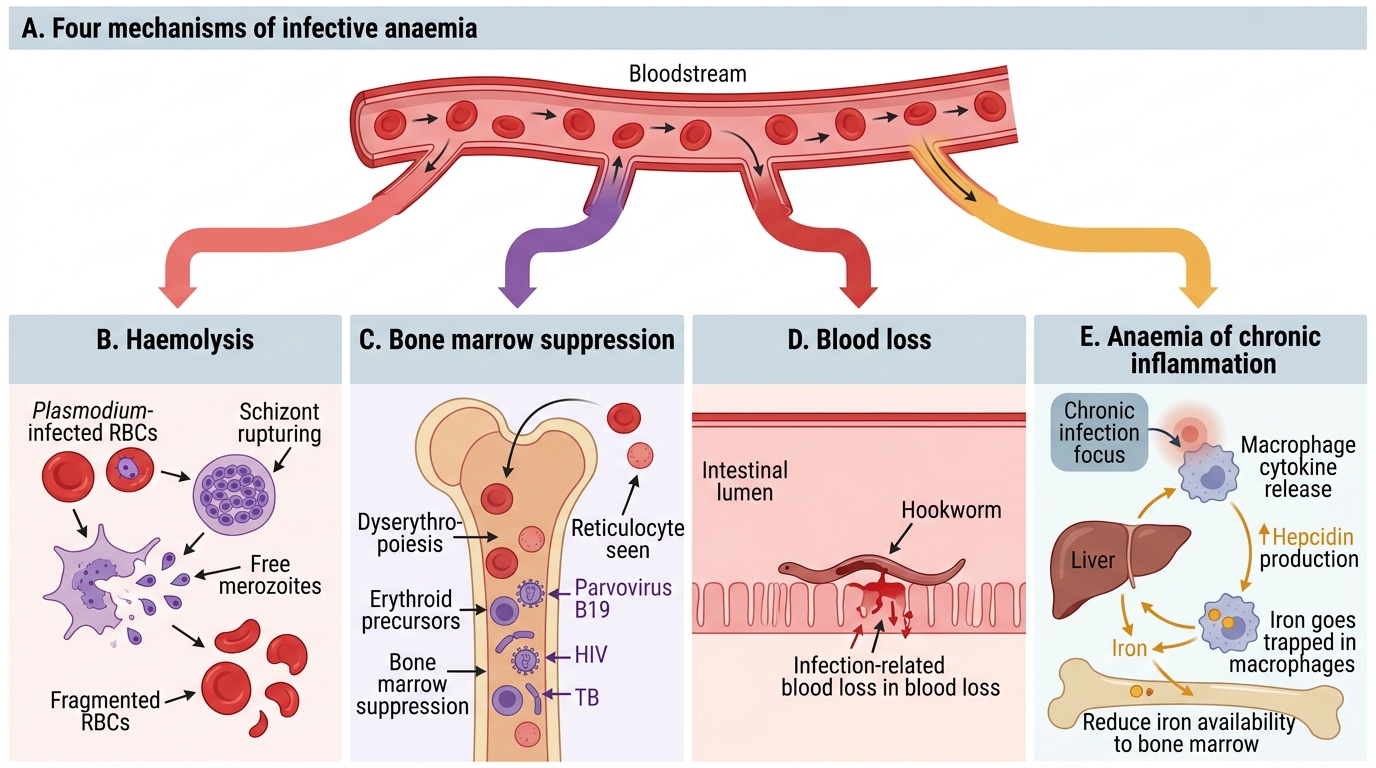
Infections cause anaemia through four main mechanisms. Many infections operate through more than one mechanism simultaneously.
| Mechanism | Examples |
|---|---|
| 1. Haemolysis (direct red cell destruction) | Malaria, babesiosis, Clostridium perfringens sepsis, Bartonella bacilliformis (Oroya fever) |
| 2. Dyserythropoiesis / Bone marrow suppression | Parvovirus B19, HIV, disseminated TB, typhoid, visceral leishmaniasis (kala-azar) |
| 3. Blood loss (from infection-driven inflammation) | Hookworm (Ancylostoma, Necator), trichuriasis (heavy load), schistosomiasis |
| 4. Anaemia of chronic disease (ACI/ACD) | TB, chronic brucellosis, osteomyelitis, chronic HIV, endocarditis, any prolonged infection |
1. Haemolytic Anaemia — Mechanism:
Malaria (Plasmodium falciparum, P. vivax, P. malariae, P. ovale)
- Merozoites invade RBCs → intracellular parasite multiplies → schizont rupture (every 48 or 72 hours) destroys the parasitised RBC
- Additional mechanisms: immune-mediated destruction of non-parasitised RBCs (bystander haemolysis), dyserythropoiesis in the bone marrow, hypersplenism (spleen traps and destroys abnormal RBCs)
- P. falciparum: infects ALL ages of RBCs → high parasitaemia, severe haemolysis; blackwater fever = massive intravascular haemolysis → haemoglobinuria (dark urine) → acute renal failure
- P. vivax/P. ovale: infect only reticulocytes; milder haemolysis
- P. malariae: infects only senescent RBCs; lowest parasitaemia
Clostridium perfringens sepsis:
- Alpha toxin (phospholipase C) cleaves phospholipids of RBC membrane → massive haemolysis → haemolytic jaundice
- Rare but fulminant when it occurs (post-abortion sepsis, gas gangrene with bacteraemia)
Bartonella bacilliformis (Oroya fever — South America; not endemic in India but may appear in examinations)
- Bacteria adhere to and invade RBCs → massive haemolysis in the acute Oroya phase
2. Bone Marrow Suppression — Mechanism:
Parvovirus B19:
- Infects and lyses erythroid progenitors (pro-erythroblasts) in bone marrow via P antigen receptor (globoside)
- In healthy individuals → fifth disease (mild anaemia); in haemolytic anaemia patients (sickle cell, thalassaemia) → aplastic crisis (sudden, severe drop in Hb)
- Mechanism: temporary arrest of erythropoiesis → reticulocytopenia
HIV:
- Direct suppression of erythropoiesis (HIV infects erythroid progenitors)
- Anaemia of chronic disease (cytokine-mediated)
- Opportunistic infections (TB, CMV, MAI) further suppress marrow
- Drug-related (zidovudine causes macrocytic anaemia by inhibiting mitochondrial DNA synthesis)
Visceral Leishmaniasis (Kala-azar) — Leishmania donovani:
- Massively enlarged spleen → hypersplenism → trapping and destruction of RBCs, WBCs, platelets (pancytopenia)
- Bone marrow infiltration by amastigotes → suppressed haemopoiesis
- Anaemia of chronic disease
Typhoid fever (Salmonella Typhi):
- Bone marrow suppression during bacteraemic phase
- Haemolysis in patients with G6PD deficiency
3. Blood Loss — Mechanism:
Hookworm (Ancylostoma duodenale and Necator americanus) — commonest infective cause of iron deficiency anaemia in India:
- Adult worms attach to jejunal mucosa, suck blood (0.03–0.15 mL blood/worm/day)
- Chronic blood loss → iron deficiency anaemia (microcytic hypochromic)
- A. duodenale more voracious (0.15 mL/worm/day) vs N. americanus (0.03 mL/worm/day)
- Heavy infection: >100 worms → 5–15 mL blood loss/day → severe iron deficiency
Trichuris trichiura (whipworm) — with heavy worm load, rectal prolapse + bloody diarrhoea → blood loss anaemia
Schistosomiasis (S. mansoni, S. japonicum) — chronic intestinal bleeding; S. haematobium → haematuria → chronic blood loss
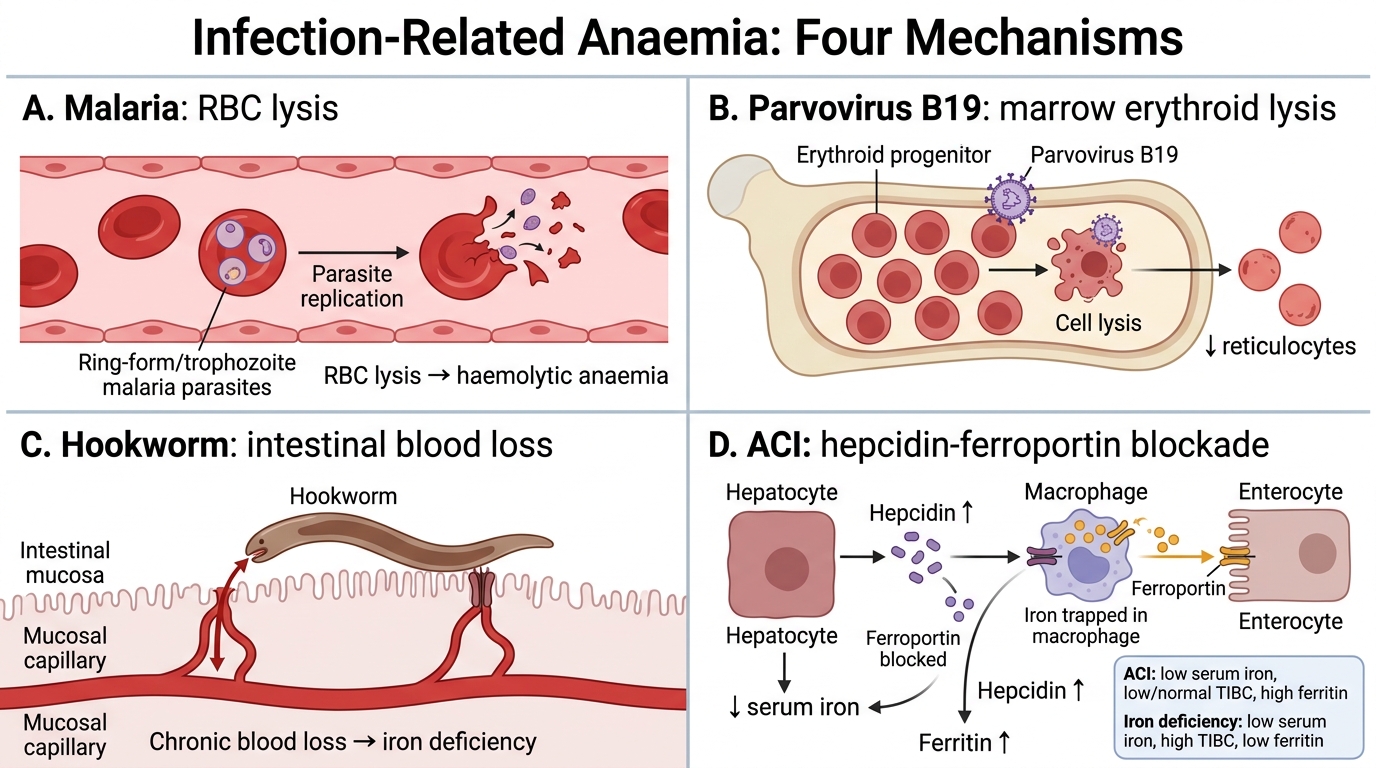
4. Anaemia of Chronic Infection (ACI) — Mechanism:
- Elevated IL-6, IL-1, TNF-α → stimulate hepcidin synthesis in the liver
- Hepcidin inhibits ferroportin on enterocytes and macrophages → iron sequestration in macrophages → iron unavailable for erythropoiesis despite normal/high stores
- Additionally: inhibition of EPO production; shortened RBC survival
- Result: normocytic normochromic anaemia with low serum iron, low TIBC, elevated ferritin (unlike iron deficiency: low ferritin)
- Common in: TB, chronic brucellosis, infective endocarditis, HIV, osteomyelitis, chronic osteomyelitis
Mechanisms of Infection-Related Anaemia
CLINICAL PEARL
Differentiating anaemia of chronic infection from iron deficiency:
| Feature | Iron Deficiency | ACI |
|---|---|---|
| Serum iron | Low | Low |
| TIBC (transferrin) | High | Low or normal |
| Ferritin | Low (<12 μg/L) | High (>100 μg/L) |
| Bone marrow iron | Absent | Present (in macrophages) |
Ferritin is the single most discriminating test — elevated ferritin in anaemia = ACI/inflammation, not iron deficiency. However, ferritin is an acute-phase reactant, so it can be elevated even when iron stores are marginally depleted if there is concurrent infection.
SELF-CHECK
A 30-year-old woman from a tea plantation in Assam presents with severe pallor and fatigue. Haemoglobin is 7.2 g/dL, MCV 64 fL (microcytic), serum ferritin 5 μg/L. Stool examination shows eggs with prominent mucus plugs at both poles. What is the MOST likely infective cause of her anaemia?
A. Plasmodium vivax malaria — haemolysis
B. Parvovirus B19 — aplastic crisis
C. Hookworm (Ancylostoma duodenale) — chronic blood loss causing iron deficiency
D. Visceral leishmaniasis — hypersplenism
Reveal Answer
Answer: C. Hookworm (Ancylostoma duodenale) — chronic blood loss causing iron deficiency
The microcytic hypochromic anaemia with very low ferritin indicates iron deficiency from chronic blood loss. Hookworm eggs have a characteristic barrel shape with mucus plugs at both poles. A. duodenale is more common in India, particularly in plantations and agricultural workers walking barefoot on contaminated soil. The clinical picture is entirely consistent with hookworm-induced iron deficiency anaemia. Malaria causes haemolytic (normocytic) anaemia; parvovirus causes normocytic with reticulocytopenia; kala-azar causes pancytopenia.
SELF-CHECK
A 10-year-old child with known sickle cell disease presents with sudden severe anaemia (Hb 4 g/dL), no fever, no jaundice, reticulocyte count near zero, and a 'slapped cheek' rash. Which organism is MOST likely responsible?
A. Plasmodium falciparum
B. Leishmania donovani
C. Parvovirus B19
D. Salmonella Typhi
Reveal Answer
Answer: C. Parvovirus B19
Parvovirus B19 infects erythroid progenitors via the P antigen (globoside) receptor and transiently halts red cell production. In a child with sickle cell disease (underlying haemolytic anaemia with shortened RBC lifespan), even a brief cessation of erythropoiesis causes a catastrophic aplastic crisis. The 'slapped cheek' rash (fifth disease) and reticulocytopenia are hallmarks. This is a medical emergency requiring red cell transfusion.
REFLECT
Construct a one-page table for your own reference:
- Column 1: Infective agent (organism)
- Column 2: Primary mechanism of anaemia
- Column 3: Type of anaemia on peripheral smear (microcytic, normocytic haemolytic, normocytic normochromic)
- Column 4: Key diagnostic test (peripheral smear, stool microscopy, marrow biopsy, etc.)
Fill in at least 8 organisms from today's session. This table will serve you in Medicine and Paediatrics clinical postings.
KEY TAKEAWAYS
Four mechanisms of infective anaemia:
1. Haemolysis — Malaria (commonest; P. falciparum most severe — blackwater fever); Cl. perfringens alpha toxin
2. Bone marrow suppression — Parvovirus B19 (aplastic crisis in haemolytic anaemia patients); HIV; Leishmania donovani (kala-azar — hypersplenism + marrow infiltration)
3. Blood loss — Hookworm (A. duodenale > N. americanus; iron deficiency anaemia; commonest infective IDA in India); Trichuriasis; Schistosomiasis
4. Anaemia of Chronic Infection (ACI) — Any prolonged infection via hepcidin-ferroportin axis → iron sequestration → normocytic normochromic anaemia
Key discriminators:
- Ferritin low → iron deficiency (usually blood loss or dietary)
- Ferritin high + normocytic → ACI or haemolysis — check peripheral smear
- Reticulocytopenia in anaemia → marrow failure (parvovirus B19, HIV, kala-azar)
- Reticulocytosis in anaemia → haemolysis (malaria)