Page 1 of 14
MI3.1-4 | Infective Endocarditis & Rheumatic Fever — SDL Guide
Learning Objectives
- Describe the etiopathogenesis, clinical features, complications, and sequelae of rheumatic fever
- Classify infective endocarditis (IE) and describe its etiopathogenesis and clinical features
- Discuss the diagnostic modalities of IE, including blood culture collection and processing, and explain the concept of sepsis
- Interpret microscopic, serological, and culture findings in a suspected case of rheumatic fever or IE to reach a clinical diagnosis
INSTRUCTIONS
Rheumatic fever and infective endocarditis are two leading infectious causes of acquired heart disease in India. Mastering their microbiology transforms you from a passive observer of 'the heart patient' to the clinician who catches the missed strep throat that seeds a valve, or reads the blood culture that changes management. Read through the blocks below, pause at micro-quizzes, and map each pathogen to its mechanism.
References
- Ananthanarayan & Paniker's Textbook of Microbiology, Ch 19 (Streptococci) (textbook)
- Harrison's Principles of Internal Medicine — Infective Endocarditis, Rheumatic Fever (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 14-year-old boy from a government school in Chennai presents with fever, migratory joint pains, and a new cardiac murmur three weeks after an episode of sore throat that was treated with paracetamol alone. His ESR is 90 mm/hr, CRP is elevated, and an echocardiogram shows mitral regurgitation.
A well-meaning junior doctor writes 'viral fever with arthralgia' and discharges him. The cardiologist reviewing him a month later says: "This child has rheumatic carditis. One missed streptococcal sore throat — one damaged heart valve for life."
By the end of this session you will understand precisely why Group A Streptococcus is the only organism that causes rheumatic fever, how molecular mimicry drives cardiac valve destruction, and how to diagnose and prevent it — and how infective endocarditis, its deadly sequel, is diagnosed through blood cultures.
WHY THIS MATTERS
India accounts for over 500,000 new cases of rheumatic heart disease annually — the highest burden in the world. Infective endocarditis is the commonest infectious cause of valvular heart disease requiring surgery. Both conditions are entirely preventable through correct microbiological diagnosis and penicillin therapy. The concepts in this module — molecular mimicry, Duke's criteria, blood culture technique, and Jones criteria — appear in MBBS professional examinations and in every real patient with a 'fever plus heart murmur' presentation.
RECALL
Before proceeding, recall:
- What is Group A beta-haemolytic Streptococcus (Streptococcus pyogenes) — where does it normally cause infection?
- What do the terms viridans streptococci and Staphylococcus aureus mean in the context of normal flora and virulence?
- What is bacteraemia versus sepsis?
- What is the function of the mitral valve and aortic valve?
If any of these are unclear, quickly revise Streptococcal chapter basics before continuing.
Rheumatic Fever: Etiopathogenesis
Rheumatic Fever: Etiopathogenesis
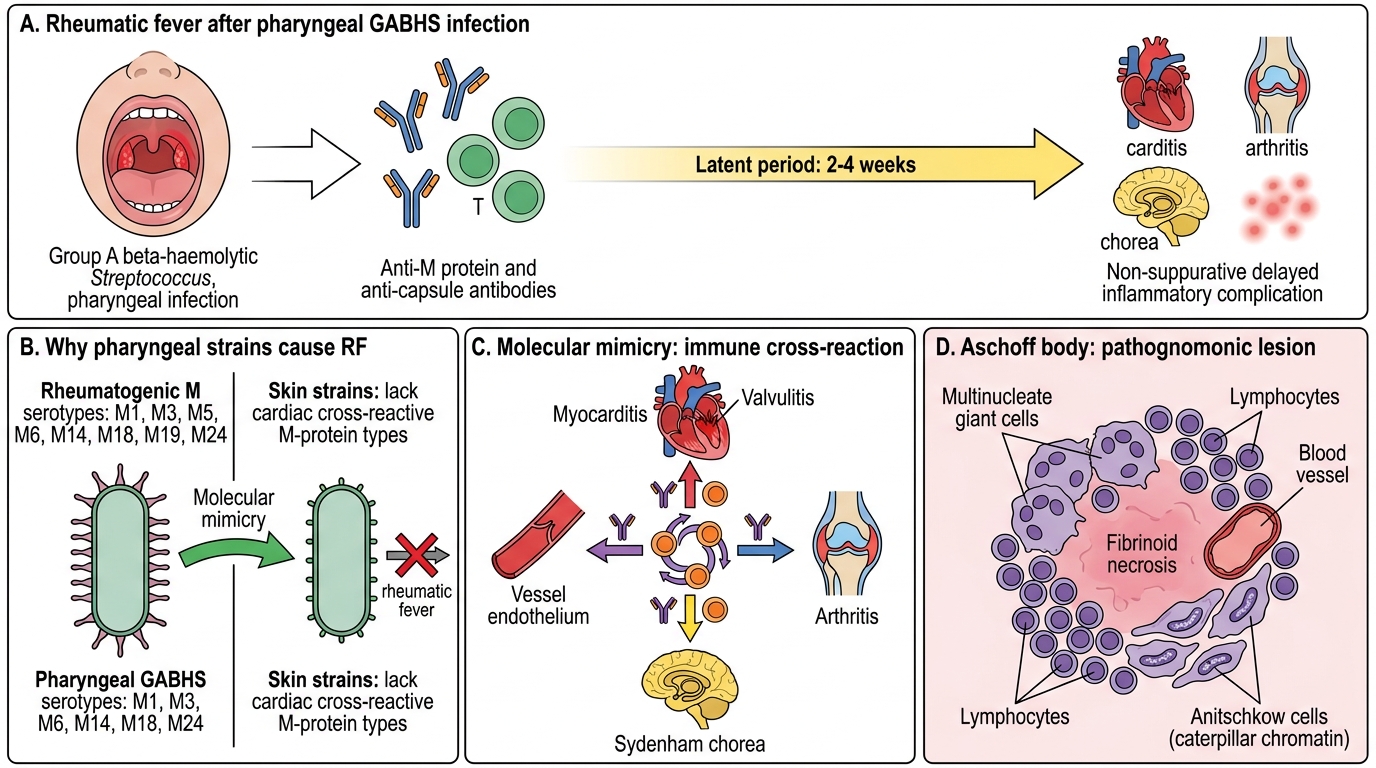
Rheumatic fever (RF) is a non-suppurative, delayed inflammatory complication of pharyngeal infection (never skin infection) with Group A beta-haemolytic Streptococcus (GABHS) — Streptococcus pyogenes.
Why only pharyngeal GABHS?
Skin strains of GABHS lack the M-protein types that cross-react with cardiac tissue. Pharyngeal strains express specific M-protein serotypes (e.g., M1, M3, M5, M6, M14, M18, M19, M24) that share antigenic similarity with host cardiac proteins — this is molecular mimicry.
Molecular mimicry — the core mechanism:
1. GABHS infects the pharynx → antibodies form against GABHS M-protein and hyaluronic acid capsule
2. These antibodies cross-react with:
- Cardiac myosin → myocarditis
- Valve leaflet endothelium → valvulitis
- Joint synovium → arthritis
- Neuronal antigens in caudate nucleus → Sydenham's chorea
3. T-lymphocytes primed against GABHS peptides also infiltrate cardiac tissue
Latent period: 2–4 weeks after pharyngitis before RF manifests.
Aschoff body — the pathognomonic histological lesion of RF: a perivascular granuloma with central fibrinoid necrosis, surrounded by Anitschkow cells (modified macrophages with caterpillar chromatin) and multinucleate giant cells.

Molecular Mimicry in Rheumatic Fever
Complications and sequelae:
- Pancarditis (pericarditis + myocarditis + endocarditis) in acute phase
- Rheumatic heart disease (RHD) — chronic valvular scarring; mitral stenosis is the commonest sequela in India
- Increased susceptibility to IE on scarred valves
- Recurrence risk — each subsequent strep throat re-triggers the immune cascade, worsening valvular damage → secondary prophylaxis with monthly benzathine penicillin is essential
Rheumatic Fever: Clinical Features & Jones Criteria
Rheumatic Fever: Pathogenesis and Jones Criteria
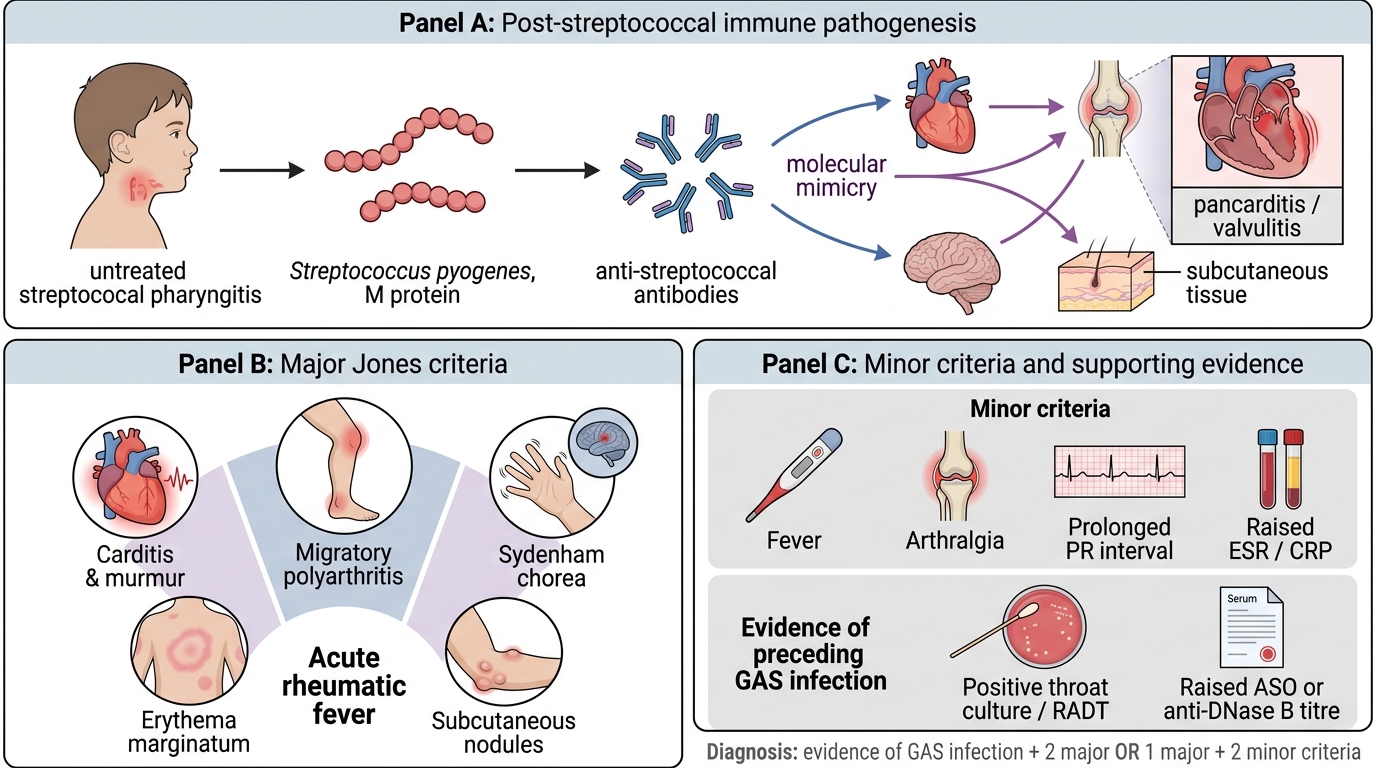
The Jones Criteria (revised 2015) are used to diagnose the first episode of RF. Two major, or one major + two minor criteria are required, PLUS evidence of preceding GABHS infection.
Major criteria (CANES):
| Criterion | Details |
|---|---|
| Carditis | Pancarditis; new murmur most significant; echocardiographic evidence now included |
| Arthritis | Migratory polyarthritis — large joints (knee, ankle, wrist); exquisitely tender |
| Nodules (subcutaneous) | Painless, over bony prominences; rare |
| Erythema marginatum | Serpentine rash over trunk; evanescent |
| Sydenham's chorea | Involuntary movements; female predominance; weeks to months after strep |
Minor criteria: Fever, elevated ESR/CRP, prolonged PR interval on ECG, arthralgia (only if arthritis is not a major criterion), previous RF.
Evidence of preceding GABHS:
- Elevated or rising ASO (Antistreptolysin O) titre — the most commonly used serological marker
- Elevated anti-DNase B — more sensitive for skin strains; complements ASO
- Positive throat culture or rapid strep antigen test (often negative by the time RF manifests)
ASO titre interpretation: ASO > 200 Todd units (adults) or > 333 Todd units (children under 5) = significant. Serial rising titres more meaningful than a single reading.
CLINICAL PEARL
The ASO trap: ASO titres peak 3–5 weeks after GABHS pharyngitis then decline — by the time RF is clinically apparent (2–4 weeks post-pharyngitis), ASO may already be falling. Always request both ASO and anti-DNase B to maximise sensitivity. A single normal ASO does NOT rule out recent GABHS infection.
SELF-CHECK
A 12-year-old girl presents with fever, migratory arthritis, and a new apical systolic murmur 3 weeks after a throat infection. Which of the following is the MOST important serological test to confirm recent GABHS infection?
A. Anti-nuclear antibody (ANA)
B. Antistreptolysin O (ASO) titre
C. Rheumatoid factor (RF)
D. C-reactive protein (CRP)
Reveal Answer
Answer: B. Antistreptolysin O (ASO) titre
ASO titre is the standard serological test for confirming preceding Group A Streptococcal pharyngitis in suspected rheumatic fever. ANA is for autoimmune disease, RF is for rheumatoid arthritis, and CRP is a non-specific acute-phase reactant (minor criterion for RF, not evidence of GABHS).
Infective Endocarditis: Classification & Etiopathogenesis
Infective Endocarditis: Classification and Etiopathogenesis
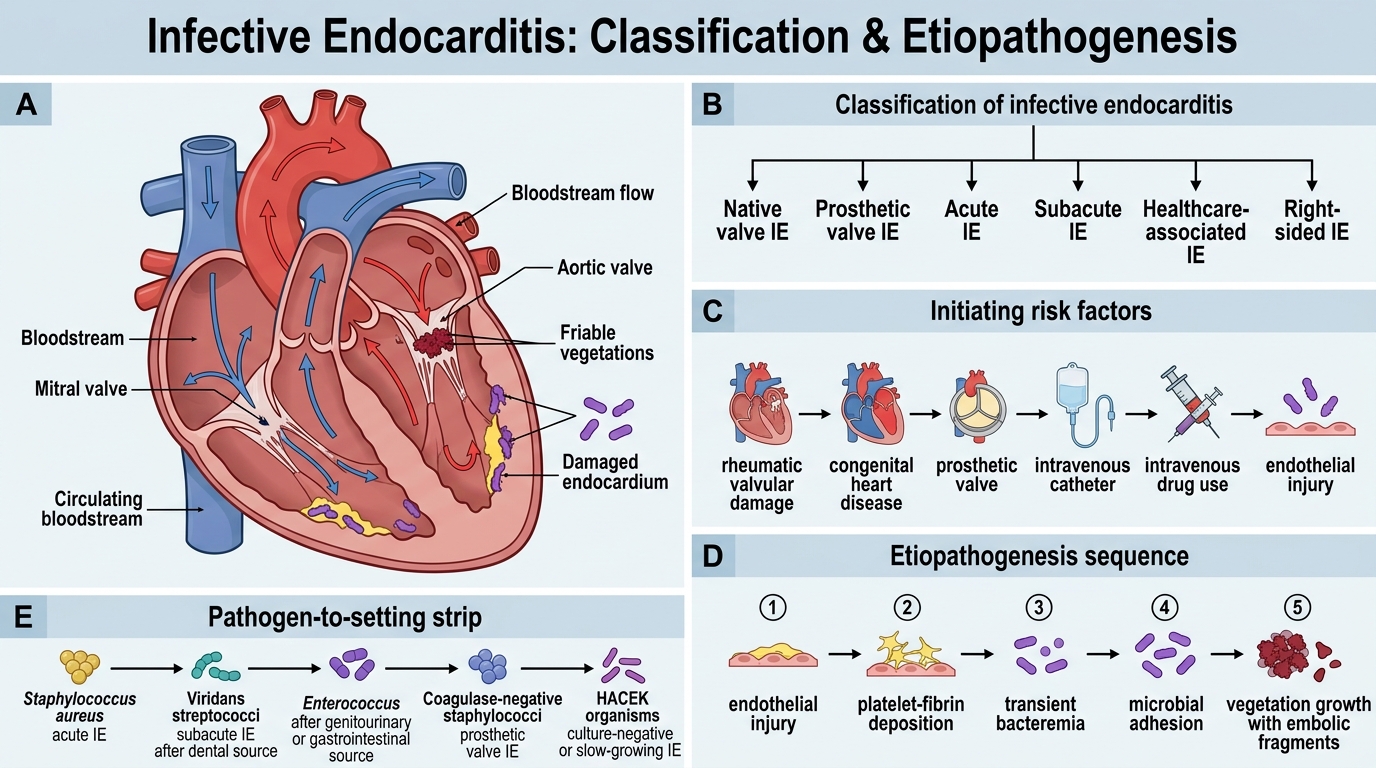
Infective endocarditis (IE) is microbial infection of the cardiac endothelium, most commonly the valves, producing vegetations — friable masses of fibrin, platelets, red cells, and organisms.
Classification:
By clinical course:
- Acute IE (AIE): Rapid onset (days to weeks); aggressive organisms (S. aureus); destroys normal valves; high mortality if untreated
- Subacute IE (SIE): Insidious onset (weeks to months); less virulent organisms (viridans streptococci); usually on abnormal valves
By valve type:
- Native valve IE (NVIE): Most common
- Prosthetic valve IE (PVIE): Early (<60 days post-surgery) vs late
- Right-sided IE: IV drug users — tricuspid valve; Staphylococcus aureus predominates
Common causative organisms:
| Organism | Setting | % of cases |
|---|---|---|
| Staphylococcus aureus | IVDU, skin/IV catheter | 30–40% (most common worldwide) |
| Viridans streptococci (S. sanguinis, S. mutans, S. salivarius) | Dental procedures, native valves | 20–30% |
| Enterococcus faecalis | GI/GU procedures, elderly | 10–15% |
| HACEK group | Slow-growing Gram-negative rods | 5–10% |
| Staphylococcus epidermidis | Prosthetic valves | 5% |
| Fungi (Candida, Aspergillus) | IV drug users, immunocompromised | Rare |
Pathogenesis:
1. Endothelial damage — congenital lesions, RHD, prosthetic valves, turbulent flow create a roughened surface
2. Non-bacterial thrombotic endocarditis (NBTE) — sterile platelet-fibrin thrombus forms on damaged endothelium
3. Transient bacteraemia — dental procedures (viridans strep), IV drug use (S. aureus), GI/GU manipulation (enterococci)
4. Colonisation — organisms adhere to NBTE via surface adhesins (e.g., fibronectin-binding proteins in S. aureus, dextran in viridans strep)
5. Vegetation — organisms buried in fibrin matrix, protected from antibiotics and phagocytes → relentless multiplication

Heart Valve Vegetation in Infective Endocarditis