Page 1 of 10
MI8.{1-2,4} | Urinary Tract & Sexually Transmitted Infections — SDL Guide
Learning Objectives
- Describe the etiopathogenesis and laboratory diagnosis of common bacterial, viral, fungal, and parasitic infections of the genitourinary system.
- List common sexually transmitted infections (STIs) and explain the pathogenesis, laboratory diagnosis, and prevention of common bacterial and viral STIs.
- Explain the etiopathogenesis, clinical course, and appropriate specimen collection and laboratory diagnosis of the different clinical and epidemiological types of urinary tract infections.
INSTRUCTIONS
Genitourinary infections are among the most common reasons for outpatient consultations in India. This module integrates bacteriology, virology, parasitology, and clinical microbiology into one high-yield SDL. Emphasis is placed on specimen collection principles and laboratory interpretation, both of which are directly tested in theory and practical examinations.
References
- Ananthanarayan & Paniker's Textbook of Microbiology, Ch 26 (UTI), Ch 27 (STI) (textbook)
- Mandell, Douglas and Bennett's Principles and Practice of Infectious Diseases — Urinary Tract Infections (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 24-year-old woman from Bengaluru presents to your clinic with dysuria, frequency, and suprapubic pain for 2 days. She is otherwise healthy, non-pregnant. A 27-year-old male sex worker from the same city presents the same afternoon with urethral discharge and painful sores on the glans. In the evening, a diabetic woman with an indwelling urinary catheter in your surgical ward develops fever, chills, and cloudy urine. Three patients, three entirely different genitourinary infection scenarios — each requiring a different specimen, a different culture protocol, and a different treatment approach. Getting the microbiology right is what separates effective treatment from empirical guesswork.
WHY THIS MATTERS
Genitourinary infections are clinically pervasive and microbiologically diverse:
- UTI is the most common nosocomial bacterial infection in India's hospital wards and one of the top 5 reasons for antibiotic prescription in outpatient settings
- STIs carry high burden: India has an estimated 6 million new STI cases annually; syphilis, gonorrhoea, chlamydia, herpes, and HPV are all endemic
- Correct specimen collection determines whether the laboratory can give you a useful answer — urine collected by mid-stream clean catch vs catheter vs suprapubic aspiration gives entirely different contamination profiles
- Antimicrobial resistance in uropathogens (ESBL-producing E. coli, fluoroquinolone-resistant N. gonorrhoeae) is a growing crisis in India — culture and sensitivity guidance matters enormously
RECALL
Before starting, recall:
- What is the normal flora of the perineum and distal urethra, and how might it contaminate a urine specimen?
- What are the main virulence mechanisms bacteria use to adhere to host epithelial cells?
- Can you name two common Gram-negative enteric organisms that can cause both UTI and systemic infection?
Urinary Tract Infections: Etiopathogenesis
Etiopathogenesis of Urinary Tract Infection
Urinary tract infection (UTI) is defined as microbial invasion and multiplication within the urinary tract, confirmed by significant bacteriuria on culture.
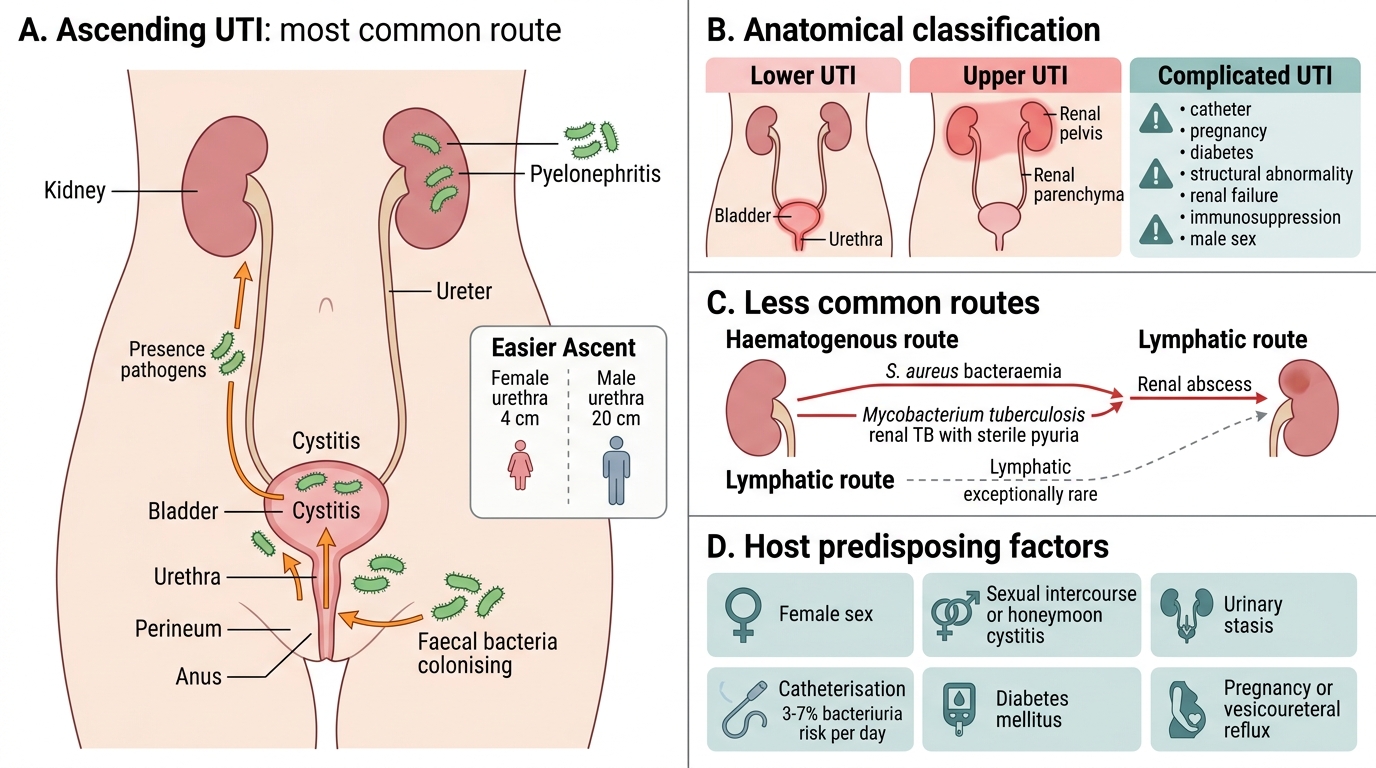
Anatomical classification:
- Lower UTI: Cystitis (bladder), urethritis
- Upper UTI: Pyelonephritis (renal pelvis + parenchyma), perinephric abscess
- Complicated UTI: UTI in the presence of structural/functional abnormality, catheter, pregnancy, diabetes, immunosuppression, renal failure, or male sex
Routes of infection:
- Ascending route (most common — >95% of UTIs): Faecal bacteria colonise the perineum → ascend urethra → bladder → ureter → kidney
- Haematogenous (descending) route: Rare; Staphylococcus aureus bacteraemia → renal abscess; Mycobacterium tuberculosis → renal TB (haematogenous always; presents with sterile pyuria)
- Lymphatic route: Exceptionally rare
Host factors predisposing to UTI:
- Female sex: Short urethra (4 cm vs 20 cm) → easier ascent; proximity of urethral meatus to anus
- Sexual intercourse: "Honeymoon cystitis" — mechanical introduction of periurethral bacteria into bladder
- Urinary stasis: Incomplete bladder emptying (BPH, neurogenic bladder, vesicoureteral reflux, pregnancy uterus)
- Catheterisation: Each day of catheterisation carries 3–7% risk of bacteriuria; CAUTI (catheter-associated UTI) is the most common hospital-acquired infection
- Diabetes mellitus: Glucosuria is a growth medium; impaired neutrophil function; autonomic neuropathy causes bladder hypotonia
- Pregnancy: Progesterone-induced ureteral dilatation + mechanical ureteral obstruction → asymptomatic bacteriuria can progress to pyelonephritis in 20–40% if untreated
Virulence mechanisms of uropathogens:
- Adhesins (fimbriae/pili): Type 1 fimbriae (bind mannose receptors on uroepithelium) and P fimbriae (bind blood group P antigen on renal tubular cells) of E. coli — P fimbriae are the key virulence factor for pyelonephritis
- Haemolysin (HlyA): Exotoxin of uropathogenic E. coli (UPEC) — lyses uroepithelial cells, promotes inflammation
- Uroease: Proteus mirabilis hydrolyses urea → ammonia → alkaline urine → struvite (triple phosphate) staghorn calculi + persistent renal infection
- Capsule (K antigen): Protects against complement and phagocytosis
- Siderophores: Iron-scavenging molecules for growth in iron-limited urine
CLINICAL PEARL
Sterile pyuria — always think TB: In a patient with pyuria (>10 WBC/hpf in urine) but a negative routine urine culture, the differential diagnosis includes: genitourinary tuberculosis (the classic), chlamydial urethritis, analgesic nephropathy, partially treated UTI, and renal calculi. In India's high-TB-burden context, sterile pyuria in a young adult with haematuria and constitutional symptoms should trigger early morning urine for acid-fast bacilli (AFB smear + culture on LJ medium) for three consecutive days.
Causative Organisms and Specimen Collection for UTI
Common Uropathogens and Urine Specimen Collection
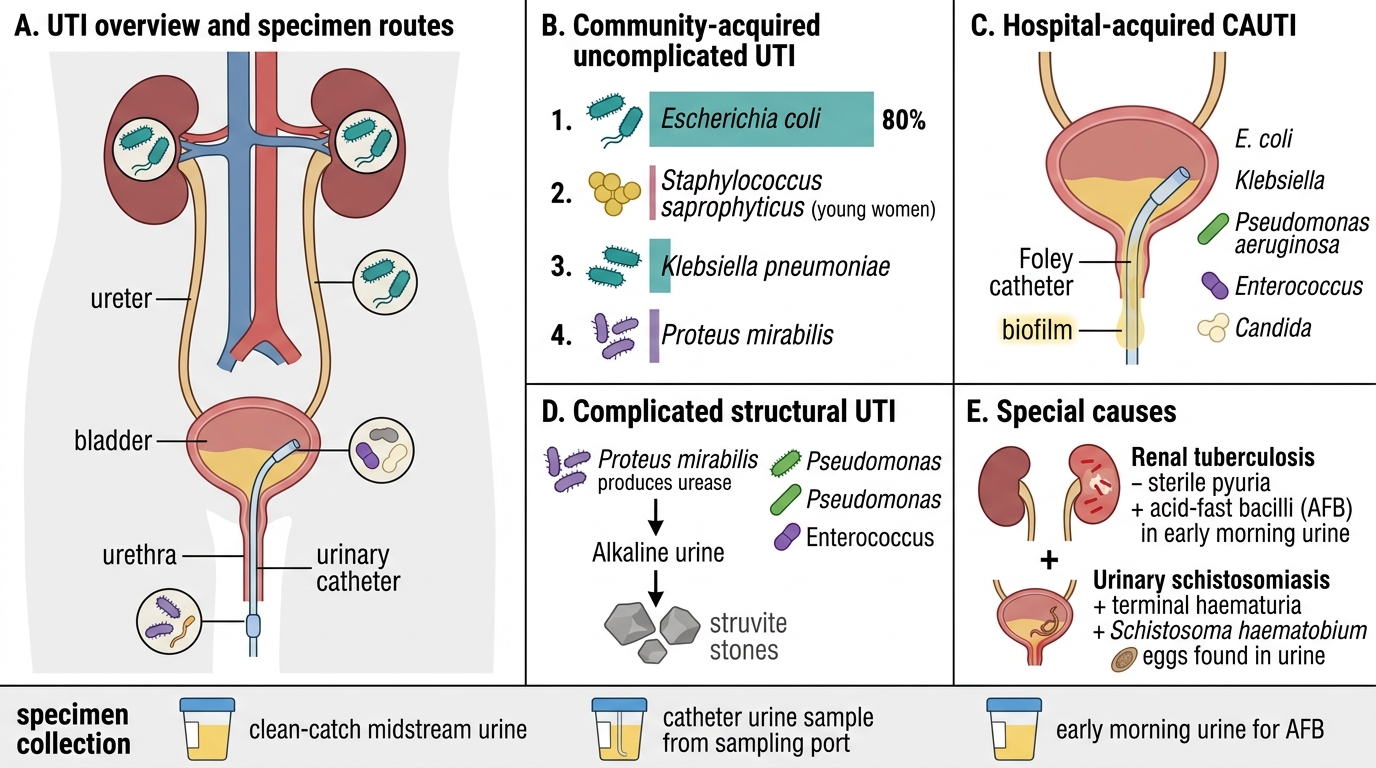
Common uropathogens by clinical setting:
| Setting | Primary pathogens | Notes |
|---|---|---|
| Community-acquired uncomplicated UTI | Escherichia coli (80%), Staphylococcus saprophyticus (young women), Klebsiella pneumoniae, Proteus mirabilis | ESBL-producing E. coli increasingly common in India |
| Hospital-acquired (CAUTI) | E. coli, Klebsiella, Pseudomonas aeruginosa, Enterococcus, Candida | Biofilm formation on catheters is key mechanism |
| Complicated UTI (structural) | Proteus mirabilis, Pseudomonas, Enterococcus | Proteus → urease → alkaline pH → struvite stones |
| Renal TB | Mycobacterium tuberculosis | Haematogenous; sterile pyuria; AFB in early morning urine |
| Schistosomiasis (India: rare, but endemic in some areas; important global) | Schistosoma haematobium | Haematuria; eggs in urine (terminal haematuria) |
Specimen collection — critical for diagnosis:
| Specimen type | Indications | Acceptable colony count (significant bacteriuria) |
|---|---|---|
| Mid-stream clean-catch (MSU) | Outpatient; ambulatory adults; standard | ≥10⁵ CFU/mL of a single organism |
| Catheter specimen (CSU) | Hospitalised patients; catheterised patients | ≥10³ CFU/mL (lower threshold due to reduced contamination) |
| Suprapubic aspiration (SPA) | Infants; equivocal MSU; gold standard for contamination concerns | ANY growth is significant (sterile procedure) |
| Early morning urine (×3) | Suspected renal TB | AFB culture on LJ medium; CBNAAT (Xpert MTB/RIF) |
Transport and processing:
- Transport within 2 hours at room temperature, or refrigerate at 4°C for up to 24 hours (prevents false colony count rise from contaminant growth)
- Dipstick urinalysis: Nitrite (reduced by Gram-negative bacteria) and leucocyte esterase (from WBCs) are rapid screening tests; negative predictive value is high but not diagnostic
- Microscopy: Mid-stream urine in a counting chamber — pyuria (>10 WBC/mm³); bacteriuria visible on Gram stain
- Culture: Calibrated loop (0.001 mL) inoculated onto CLED agar (Cystine Lactose Electrolyte Deficient — suppresses Proteus swarming) and blood agar

Urine Specimen Collection and CLED Agar Interpretation
SELF-CHECK
A 60-year-old man with BPH and an indwelling urinary catheter develops fever and rigors. Urine culture from the catheter bag grows Candida albicans ≥10⁴ CFU/mL. What is the most appropriate next step in clinical interpretation?
A. Start systemic antifungal therapy immediately — ≥10⁴ CFU/mL confirms invasive candidiasis
B. Obtain a fresh specimen from the catheter port (not the bag) and re-culture; the catheter bag is not a valid specimen
C. Repeat urine culture from the patient's voided stream only
D. Treat with bladder irrigation with amphotericin B before re-culturing
Reveal Answer
Answer: B. Obtain a fresh specimen from the catheter port (not the bag) and re-culture; the catheter bag is not a valid specimen
Urine from a catheter collection bag is NOT a valid specimen for culture because the bag is colonised and pooled urine grows abundant organisms. Specimens for catheterised patients must be aspirated from the sampling port of the catheter using a syringe after cleansing the port — this provides fresh urine directly from the bladder. Bag cultures routinely overdiagnose candiduria (and bacteriuria). Additionally, Candida in catheterised patients often represents colonisation, not infection; clinical context (fever, systemic signs, blood culture results) guides treatment decisions.
Sexually Transmitted Infections: Overview and Bacterial STIs
Overview and Bacterial Causes of Sexually Transmitted Infections
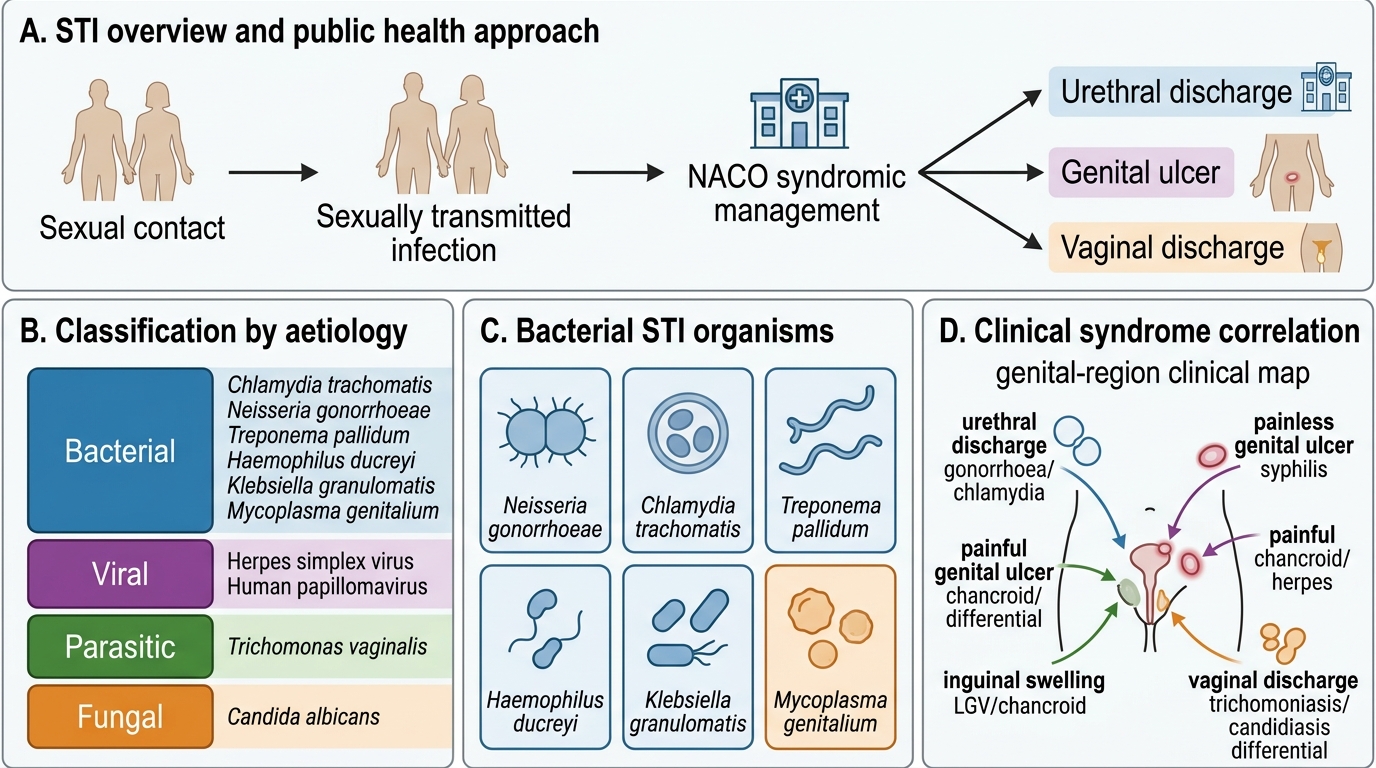
Sexually transmitted infections (STIs) are transmitted predominantly through sexual contact. India's National AIDS Control Organisation (NACO) categorises STIs for syndromic management — a public health approach where treatment is initiated based on clinical syndrome (urethral discharge, genital ulcer, vaginal discharge) without waiting for microbiological results.
Classification of STIs by aetiology:
| Category | Organisms |
|---|---|
| Bacterial | Neisseria gonorrhoeae (gonorrhoea), Chlamydia trachomatis (chlamydia, LGV), Treponema pallidum (syphilis), Haemophilus ducreyi (chancroid), Klebsiella granulomatis (donovanosis/granuloma inguinale), Mycoplasma genitalium |
| Viral | HSV-1/2 (herpes genitalis), HPV (warts, cervical cancer), HIV, HBV, HCV, CMV |
| Parasitic | Trichomonas vaginalis (trichomoniasis) |
| Fungal | Candida albicans (vulvovaginal candidiasis — not strictly STI) |
Gonorrhoea (Neisseria gonorrhoeae)
- Pathogen: Gram-negative diplococci (kidney-bean shaped, in pairs); fastidious, oxidase-positive
- Pathogenesis: Pili (fimbriae) attach to urethral columnar epithelium → invasion → IgA protease (cleaves secretory IgA) → local infection; spreads to epididymis (males), fallopian tubes (females → PID)
- Clinical features: Males: urethral discharge (purulent, yellow-green), dysuria. Females: often asymptomatic (80%) or cervicitis, vaginal discharge. Complications: PID, Fitz-Hugh-Curtis syndrome (perihepatitis), disseminated gonococcal infection (DGI — skin pustules, migratory polyarthritis, tenosynovitis)
- Diagnosis:
- Urethral/cervical swab → Gram stain: intracellular Gram-negative diplococci within PMNs (highly diagnostic in symptomatic males)
- Culture: Thayer-Martin (TM) medium (chocolate agar + antibiotics: vancomycin, colistin, nystatin) at 37°C in 5% CO₂
- NAAT (Nucleic Acid Amplification Tests): Most sensitive; used on urine or swab; can detect Chlamydia simultaneously
- Ophthalmia neonatorum: Neonatal conjunctivitis from vertical transmission during delivery → blindness risk; prevented by 1% silver nitrate or erythromycin eye drops at birth
Chlamydial infections (Chlamydia trachomatis)
- Pathogen: Obligate intracellular bacterium; lacks peptidoglycan wall; exists as elementary body (EB) (infectious, metabolically inert) and reticulate body (RB) (intracellular, metabolically active, replicating)
- Serovars and disease:
- D–K: Urethritis, cervicitis (most common STI in UK, increasingly in India), neonatal conjunctivitis, neonatal pneumonia
- L1–L3: Lymphogranuloma venereum (LGV) — painful inguinal lymphadenopathy (buboes), rectal disease; more common in MSM in India
- A–C: Trachoma (ocular — leading infectious cause of blindness; endemic in rural India)
- Clinical features of genital chlamydia: Often asymptomatic in both sexes (key reason for sustained transmission); urethritis in males (non-gonococcal urethritis, NGU); cervicitis, PID, ectopic pregnancy, infertility in females
- Diagnosis: Cannot culture on standard media (obligate intracellular)
- NAAT (PCR): Gold standard — high sensitivity, can use first-void urine
- Direct immunofluorescence (DIF): Fluorescent antibody on swab specimen detects elementary bodies
- Enzyme immunoassay (EIA): Less sensitive than NAAT
- Serology (MIF): Microimmunofluorescence for LGV diagnosis (IgA titres)
Syphilis (Treponema pallidum)
- Pathogen: Spirochaete; cannot be cultured in vitro; visualised by dark-field microscopy of primary lesion exudate
- Stages and clinical features:
- Primary: Painless indurated ulcer (chancre) + regional lymphadenopathy; 3–4 weeks after exposure; highly infectious
- Secondary: 6–8 weeks after chancre heals; generalised copper-coloured maculopapular rash including palms and soles (pathognomonic); condylomata lata (flat, warty, highly infectious); mucous patches; systemic — fever, lymphadenopathy
- Latent: Asymptomatic; early (<2 years) vs late (>2 years)
- Tertiary: Years later; gumma (granulomatous), cardiovascular syphilis (aortitis, aortic regurgitation), neurosyphilis (tabes dorsalis, general paresis of the insane)
- Congenital syphilis: Saddle nose, Hutchinson's teeth, interstitial keratitis, periostitis (Wimberger sign), snuffles
- Diagnosis:
- Dark-field microscopy: Primary chancre exudate — treponemes visible as corkscrew motility
- Non-treponemal tests (screening): VDRL, RPR — detect anti-cardiolipin (reagin) antibody; become positive in secondary syphilis; titres correlate with disease activity and treatment response; biological false-positives occur in SLE, TB, malaria, pregnancy
- Treponemal tests (confirmatory): TPHA (Treponema Pallidum Haemagglutination Assay), FTA-ABS (Fluorescent Treponemal Antibody Absorption), ELISA — detect anti-treponemal antibodies; remain positive for life (cannot use for treatment monitoring)

Genital Ulcer Diseases: Key Distinguishing Features
SELF-CHECK
A 25-year-old man presents with a single painless ulcer on his glans with indurated margins and bilateral painless inguinal lymphadenopathy for 1 week. VDRL is reactive. TPHA confirms positivity. He received antibiotic treatment 1 year ago for a similar presentation. His current VDRL titre is 1:4. Which of the following correctly interprets his serological results?
A. The VDRL titre of 1:4 confirms active secondary syphilis requiring benzathine penicillin 2.4 MU
B. VDRL and TPHA both positive indicates primary syphilis with serological conversion
C. TPHA positivity always indicates active disease regardless of VDRL titre
D. If VDRL titres have fallen from a prior higher level after treatment, this pattern is consistent with successfully treated past syphilis; rising titres would indicate active infection or reinfection
Reveal Answer
Answer: D. If VDRL titres have fallen from a prior higher level after treatment, this pattern is consistent with successfully treated past syphilis; rising titres would indicate active infection or reinfection
Non-treponemal tests (VDRL, RPR) titres rise with active untreated infection and fall with successful treatment — they are used to monitor treatment response (a four-fold fall in titre indicates adequate treatment). Treponemal tests (TPHA, FTA-ABS) become positive with infection and remain positive for life even after cure — they cannot distinguish past from active infection. A VDRL titre of 1:4 in a patient previously treated needs to be compared to prior titres. Rising titres suggest active infection or reinfection. A falling/low stable titre after prior treatment may represent serological scar (serofast reaction). Clinical presentation (painless indurated chancre = primary syphilis staging) plus rising/falling titre trend guides management.