Page 1 of 11
MI9.1-3 | Zoonotic & Opportunistic Infections — SDL Guide
Learning Objectives
- Define and classify zoonotic infections; explain the etiopathogenesis, vectors, transmission, risk factors, laboratory diagnosis and prevention of major zoonoses
- Describe the etiopathogenesis and laboratory diagnosis of opportunistic infections (OI) in immunocompromised hosts caused by bacterial, viral, fungal and parasitic agents
- Choose the most suitable microbiological investigation for a given clinical situation involving zoonoses or OIs, and interpret the results
INSTRUCTIONS
India is home to some of the world's deadliest zoonoses — rabies, leptospirosis, brucellosis, plague — and hosts the fastest-growing HIV epidemic in South-East Asia. Both zoonoses and OIs present as diagnostic puzzles that kill if missed. This SDL trains you to recognise the epidemiological clue (animal contact, vector, immune status) that unlocks the diagnosis.
References
- Ananthanarayan & Paniker's Textbook of Microbiology, Ch 37 (Brucella), Ch 38 (Leptospira), Ch 40 (Plague), Ch 72 (Rabies), Ch 62 (Opportunistic infections) (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 35-year-old farmer from Andhra Pradesh presents in September with 5 days of high fever, severe headache, myalgia and red eyes. He reports wading through flooded rice fields for the past week. Three other farmers from the same village were admitted last month with similar illness and jaundice. What is the most likely diagnosis, and which single investigation will you send first?
WHY THIS MATTERS
Zoonoses account for 75% of all emerging infectious diseases globally. In India, rabies kills ~18,000–20,000 people annually (highest in the world), leptospirosis outbreaks follow every monsoon in coastal states, and brucellosis affects millions of farming families. Opportunistic infections are the leading cause of mortality in HIV-positive patients — India has ~2.4 million people living with HIV (PLHIV). Recognising these conditions early is a life-saving skill.
RECALL
Before proceeding, recall: (1) Definition of zoonosis — an infection transmissible from vertebrate animals to humans under natural conditions. (2) Types of vectors: mechanical (non-replicating transport, e.g., housefly) vs biological (pathogen replicates/develops, e.g., Aedes, Ixodes). (3) Opportunistic infection — infection by organism of low intrinsic virulence that causes disease only when host immune defences are compromised. (4) CD4 count thresholds: <500 → early OIs; <200 → PCP, histoplasmosis; <100 → Cryptococcus, CMV retinitis; <50 → MAC.
Classification and Overview of Zoonoses
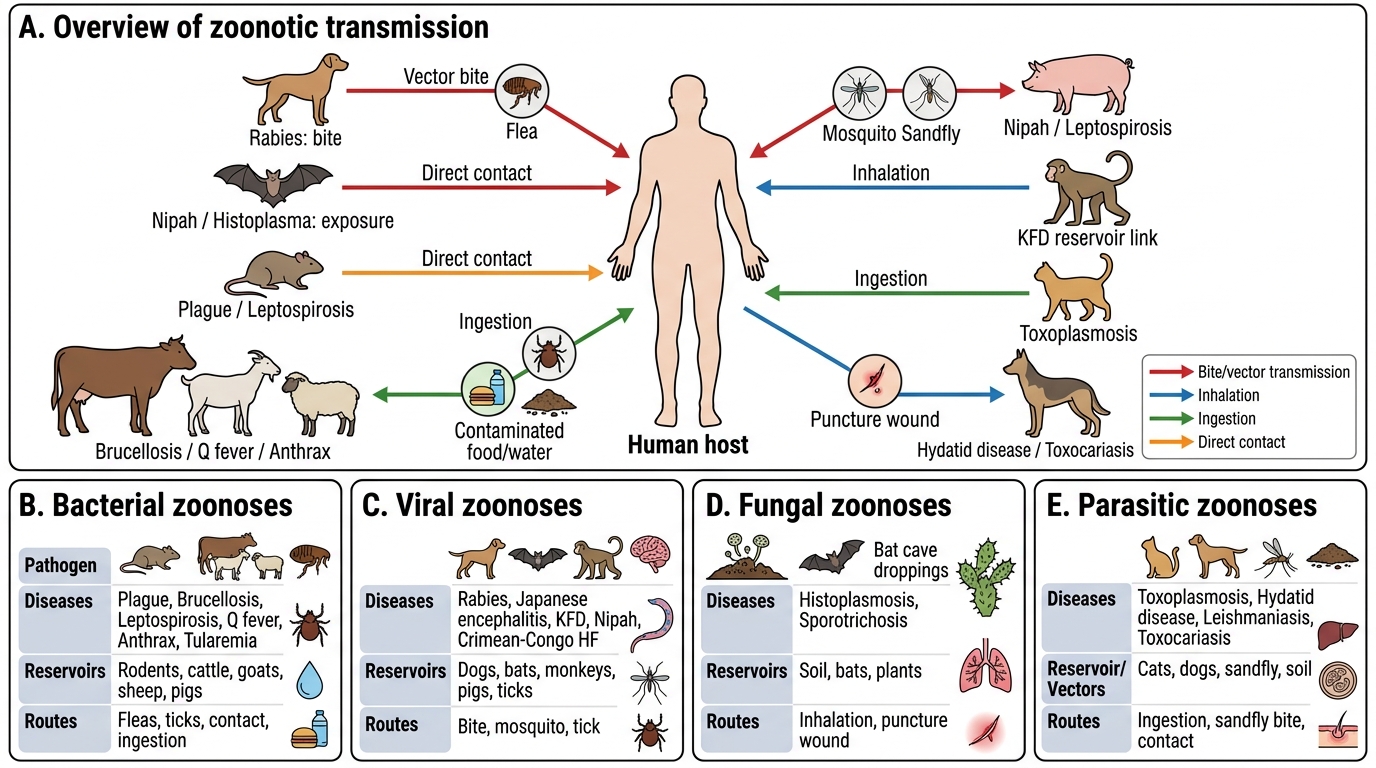
Classification and Overview of Zoonoses
Classification by pathogen type:
| Type | Major Zoonoses in India | Reservoir | Vector/Route |
|---|---|---|---|
| Bacterial | Plague, Brucellosis, Leptospirosis, Q fever, Anthrax, Tularemia | Rodents, cattle, goats, sheep, pigs | Fleas, ticks, contact, ingestion |
| Viral | Rabies, Japanese encephalitis, Kyasanur Forest Disease (KFD), Nipah, Crimean-Congo HF | Dogs, bats, monkeys, ticks, pigs | Bite, mosquito, tick |
| Fungal | Histoplasmosis, Sporotrichosis | Soil/bats (Histoplasma), soil/plants (Sporothrix) | Inhalation, puncture wound |
| Parasitic | Toxoplasmosis, Hydatid disease, Leishmaniasis, Toxocariasis | Cats, dogs, sandfly, soil | Ingestion, sandfly bite, contact |
Major Bacterial Zoonoses
Major Bacterial Zoonoses: Leptospirosis and Brucellosis
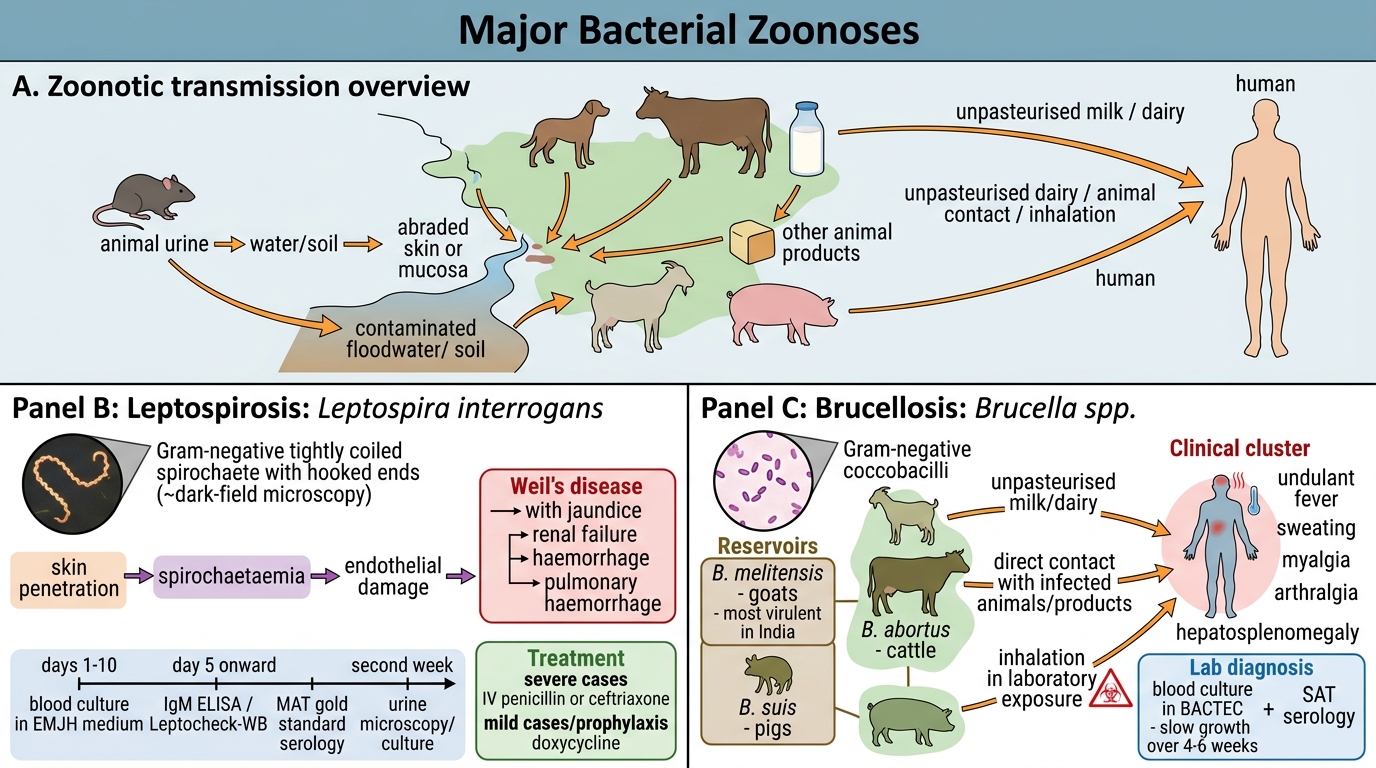
1. Leptospirosis (Leptospira interrogans)
- Gram-negative, tightly coiled spirochaete with hooked ends; motile (requires dark-field microscopy)
- Weil's disease — severe leptospirosis with jaundice, renal failure, haemorrhage
- Transmission: Contact of abraded skin or mucous membranes with water/soil contaminated by animal urine (rats, dogs, cattle); occupational — farmers, sewer workers, flood rescue
- Pathogenesis: Penetrates intact/abraded skin → spirochetaemia → endothelial damage → hepatorenal syndrome, pulmonary haemorrhage
- Lab diagnosis:
- Blood culture in EMJH medium (first 7–10 days)
- Dark-field microscopy of blood/urine (not sensitive in labs; artefacts common)
- MAT (Microscopic Agglutination Test) — gold standard serology; detects serovar-specific antibodies; reference lab test
- IgM ELISA (Leptocheck-WB) — rapid bedside test; positive from day 5
- Urine microscopy/culture (second week)
- Treatment: IV penicillin/ceftriaxone (severe); doxycycline (mild/prophylaxis)
2. Brucellosis (Brucella spp.)
- Gram-negative, small coccobacillus; B. melitensis (goats — most virulent in India), B. abortus (cattle), B. suis (pigs)
- 'Undulant fever' — undulating pyrexia with sweating, myalgia, arthralgia, hepatosplenomegaly
- Transmission: Ingestion of unpasteurised milk/dairy (main route in India), direct contact with infected animals/products, inhalation (lab biohazard — Biosafety Level 3)
- Lab: Blood culture in BACTEC (4–6 weeks; slow); SAT (Standard Agglutination Test) titre ≥1:80 significant; 2-mercaptoethanol (2-ME) test to distinguish IgM (acute) from IgG (past/chronic); Brucella-capt or ELISA
- Treatment: Doxycycline + rifampicin (6 weeks) or doxycycline + streptomycin (preferred by WHO)
3. Plague (Yersinia pestis)
- Gram-negative coccobacillus with bipolar staining (safety-pin appearance on Giemsa/Wayson stain); F1 capsule (anti-phagocytic)
- Reservoir: Rats; vector: rat flea (Xenopsylla cheopis) — transmitted when rat dies, fleas seek human host
- Forms: Bubonic (bubo — swollen, tender lymph node in inguinal/axillary/cervical region), Septicaemic, Pneumonic (most dangerous — human-to-human droplet; Biosafety Level 3)
- Lab: Aspirate from bubo; Gram stain + Wayson stain (safety-pin morphology); culture on MacConkey; F1 antigen rapid test; PCR
- India: Last major epidemic in Surat, 1994. Endemic foci in Himalayan foothills.
- Treatment: Streptomycin/gentamicin (drug of choice); doxycycline
4. Anthrax (Bacillus anthracis)
- Gram-positive, spore-forming, capsulate rod
- Forms: Cutaneous (malignant pustule → eschar — painless black necrotic ulcer, most common), Inhalation ('Woolsorter's disease'), Gastrointestinal
- Lab: Culture on blood agar (non-haemolytic, rough colonies); Gram stain; ELISA for anthrax toxin; ascoli precipitin test (for animal products)
- Treatment: Ciprofloxacin/doxycycline; anthrax antitoxin

Leptospira interrogans: Morphology, Exposure, and Weil Disease Clue
CLINICAL PEARL
Weil's disease diagnostic clue: High fever + jaundice + acute kidney injury + haemorrhagic manifestations + monsoon season + occupational/flood exposure = Leptospirosis until proven otherwise. Send IgM ELISA on day 5 and MAT for definitive serogrouping. Do NOT wait for LFT/RFT to normalise before treating — penicillin/ceftriaxone must start on clinical suspicion.
Major Viral Zoonoses
Major Viral Zoonoses: Rabies and Kyasanur Forest Disease
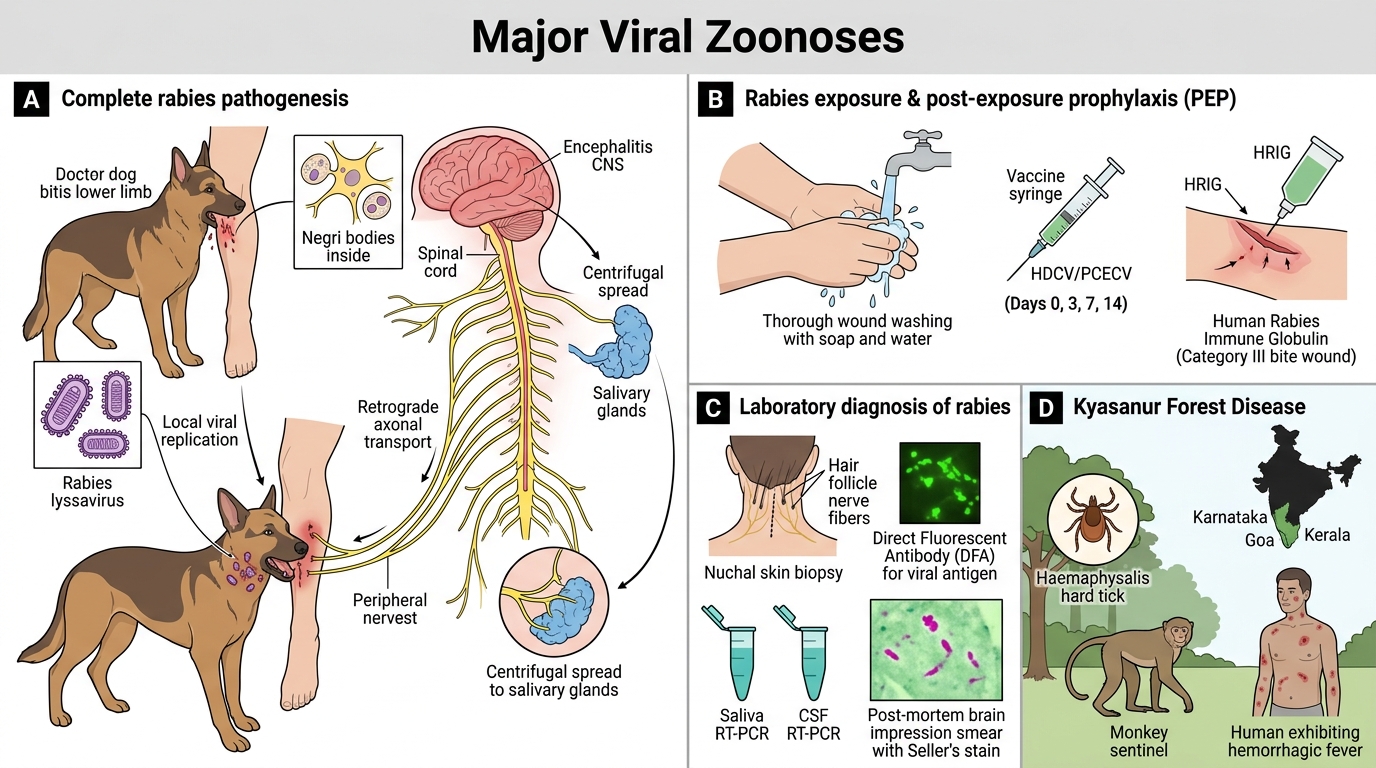
Rabies (Rabies lyssavirus):
- Negative-sense ssRNA; Rhabdoviridae; bullet-shaped
- Transmission: Bite/scratch/lick on broken skin from infected dog (95% in India), cat, bat, mongoose
- Pathogenesis: Virus replicates locally at site → ascends via peripheral nerve axons (retrograde axoplasmic transport) → reaches CNS → encephalitis → descends to salivary glands → hydrophobia (pharyngeal spasm on swallowing), aerophobia, autonomic dysfunction, Negri bodies (eosinophilic cytoplasmic inclusions in hippocampal Purkinje cells — pathognomonic)
- Incubation: 2 weeks–6 months (depends on bite site distance from CNS)
- Lab (ante-mortem): Nuchal skin biopsy (DFA for viral antigen in nerve fibres around hair follicles — most reliable); saliva RT-PCR; CSF RT-PCR; serum/CSF neutralising antibody titre
- Lab (post-mortem): Brain impression smear — Seller's stain → Negri bodies (magenta on green)
- Pre-exposure prophylaxis (PrEP): HDCV/PCECV vaccine on days 0, 7, 21/28 (for veterinarians, lab workers, travellers)
- Post-exposure prophylaxis (PEP): Wound washing 15 min with soap + HDCV on days 0,3,7,14 + HRIG (Human Rabies Immune Globulin) infiltrated into wound (for category III exposure) — THIS IS LIFE-SAVING
Kyasanur Forest Disease (KFD) — India-specific:
- Flavivirus; Haemaphysalis tick (hard tick); monkeys (sentinel) + humans
- Endemic: Karnataka, Goa, Kerala forests; monkey fever — haemorrhagic fever
- Vaccine: Formalin-inactivated KFD vaccine (available in India, forest area residents)
Nipah Virus:
- Paramyxovirus; fruit bats (Pteropus) are reservoir; transmission via contaminated fruit/date palm sap or direct contact
- Outbreaks in Kerala (2018, 2019, 2023): encephalitis, high CFR (~65–75%)
- BSL-4 pathogen; no approved vaccine or antiviral (ribavirin investigational)
Japanese Encephalitis (JE):
- Flavivirus; Culex mosquito → pig/bird amplifying hosts → humans (dead-end host)
- Acute encephalitis syndrome; MRI: bilateral thalamic lesions (characteristic)
- Prevention: JE vaccine (SA-14-14-2 live attenuated) in UIP in endemic districts