Page 6 of 14
OG1.4-5 | Caesarean Audit and National OG Programs — SDL Guide
Learning Objectives
- Describe the Robson Ten-Group Classification System and define all 10 groups by their obstetric characteristics
- Explain how to conduct a caesarean section audit using the Robson TGCS and identify which groups drive high CS rates
- Describe the key features, beneficiaries, and services of JSY and JSSK
- Explain the objectives and key interventions of Anaemia Mukt Bharat and SUMAN
- Describe the purpose and legal basis of the birth and death registration system (RBD Act 1969)
- Apply programme knowledge to identify eligible patients and fulfil documentation responsibilities in clinical practice
INSTRUCTIONS
India's caesarean section rate has risen sharply over the past two decades, reaching over 21% nationally (NFHS-5, 2019–21) — with private sector rates exceeding 47%. Understanding whether this rise is clinically justified requires a systematic audit tool. The Robson Ten-Group Classification System provides precisely this framework. Simultaneously, India operates several national programmes specifically designed to improve obstetric and neonatal outcomes: JSY, JSSK, Anaemia Mukt Bharat, SUMAN, and the civil birth/death registration system. As a final-year student about to enter clinical practice, you need both the audit tools to monitor your institution's care quality and the programme knowledge to enrol eligible patients and fulfil your documentation obligations.
References
- DC Dutta's Textbook of Obstetrics, 9th Ed, Ch 1 — National Programmes (textbook)
- WHO: Robson Classification — Implementation Manual, WHO/RHR/15.23, Geneva 2017 (guideline)
- National Family Health Survey-5 (NFHS-5), 2019-21 — Ministry of Health and Family Welfare, India (report)
- Ministry of Health and Family Welfare: JSSK Implementation Framework, 2011 (guideline)
- Anaemia Mukt Bharat — Intensified National Iron Plus Initiative (I-NIPI), MoHFW 2018 (guideline)
- SUMAN — Surakshit Matritva Aashwasan, MoHFW 2019 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
You are the medical officer in charge of the obstetrics ward at a 200-bed district hospital. Your facility's caesarean section rate for the last year is 32% — well above the national average and the WHO's 10–15% population-level benchmark. The medical superintendent asks you to present a departmental audit at next month's quality meeting. Where do you begin? How do you determine which subset of patients is driving the high rate — is it the women with previous caesareans, the nulliparous women being induced, or the preterm cases? And when you find the answer, what clinical interventions and national programme supports can you mobilise to address it? This module gives you the framework to answer all of these questions.
WHY THIS MATTERS
Caesarean section rates in India are among the fastest-rising in the world. A CS rate above the clinically necessary level confers maternal risks (haemorrhage, infection, anaesthetic complications, future uterine rupture, placenta accreta spectrum) without proportional neonatal benefit. The Robson classification is the WHO-recommended tool for every facility globally to audit, benchmark, and communicate about CS rates in a standardised, reproducible way. On the programme side, JSY increased institutional delivery rates from under 40% to over 80% — one of the most impactful maternal health interventions in Indian public health history. Knowing these programmes enables you to connect vulnerable women to entitlements they may not know about, and to complete the documentation that unlocks cash transfers, free diagnostics, and transport — often on the same night a woman presents in labour.
RECALL
From OG1.1–1.3 (this cluster), recall: maternal mortality ratio (MMR), maternal death classification, perinatal mortality rate. Recall the three-delays model — Delay I (decision to seek care), Delay II (reaching facility), Delay III (receiving care). From Community Medicine, recall: the civil registration system as the source of vital statistics; anaemia in pregnancy (haemoglobin <11 g/dL). From basic obstetrics, recall: terms for labour onset — spontaneous versus induced; parity — nulliparous (no previous birth ≥20 weeks) versus multiparous; and modes of delivery — vaginal versus caesarean.
Orientation: Why Audit Caesarean Sections and Track National Programs
Caesarean section audit and national programme monitoring are two complementary pillars of obstetric quality governance. Audit is the internal mechanism by which a facility examines its own practice and identifies scope for improvement — in this case, whether its CS rate reflects clinical necessity or system-level factors such as patient preference, fear of litigation, lack of skilled staff for safe vaginal delivery, or perverse financial incentives. National programme monitoring ensures that government-funded interventions designed to address the determinants of maternal and perinatal mortality actually reach the intended beneficiaries.
For the final-year student entering clinical practice, these are not abstract governance concepts. Every week in a busy obstetric unit, you will make or observe decisions about mode of delivery. Every patient who delivers in a public facility is entitled to specific services under JSSK; every woman below the poverty line who delivers institutionally is eligible for a cash transfer under JSY. Every birth must be notified and registered. If a pregnant woman with severe anaemia is admitted to your ward, Anaemia Mukt Bharat protocols govern her management. If a labouring woman is denied free drugs or diagnostic tests, SUMAN's minimum service guarantees have been violated. Operationalising this knowledge — recognising eligibility, initiating correct documentation, and participating in audits — is a measurable clinical responsibility.
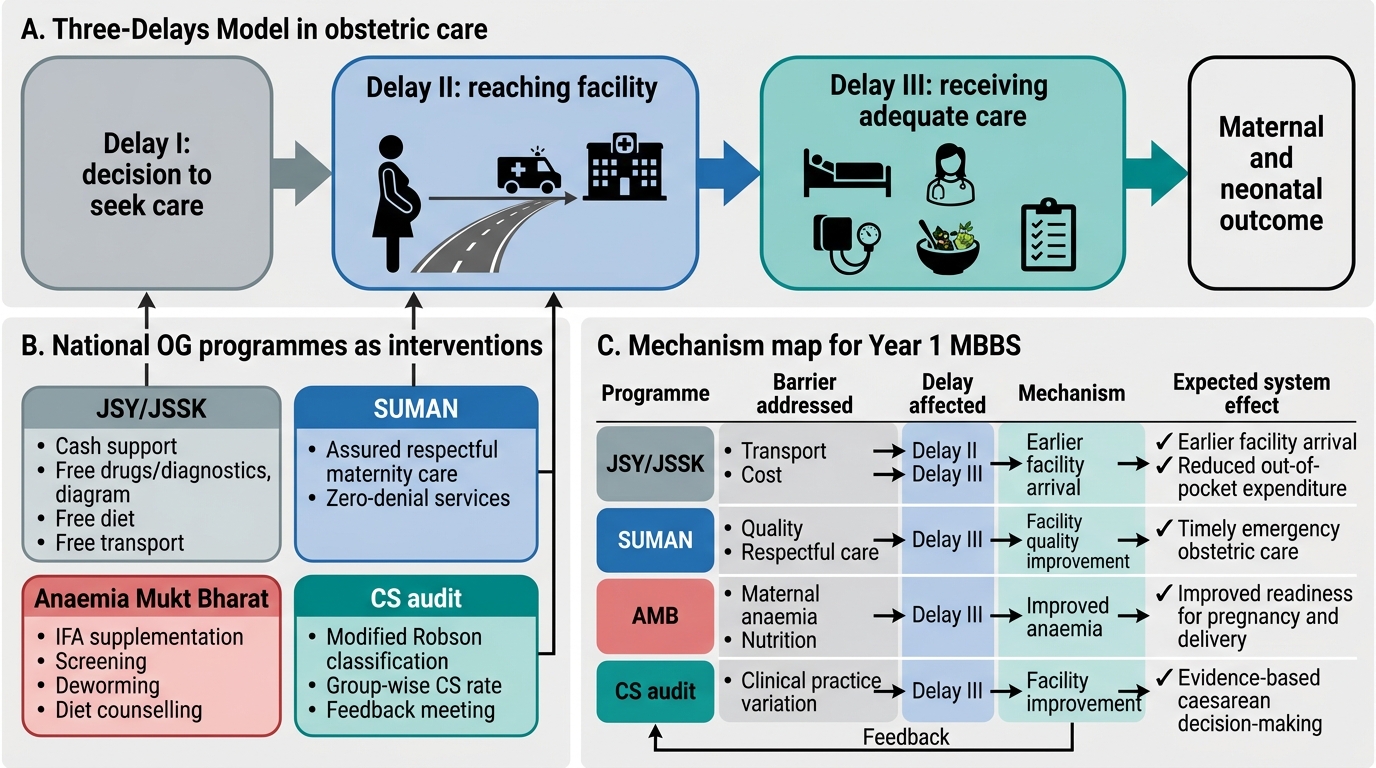
National OG Programmes and the Three-Delays Model
The two competencies this module addresses — OG1.4 (caesarean audit using modified Robson classification) and OG1.5 (national OG programmes: JSY, JSSK, birth and death registration, Anaemia Mukt Bharat, SUMAN) — are classified at the 'KH' (Knowledge and Understand and Higher' level, meaning you are expected not only to recall facts but to apply them to clinical decision-making and audit contexts.
The Robson Ten-Group Classification System: Groups and Definitions
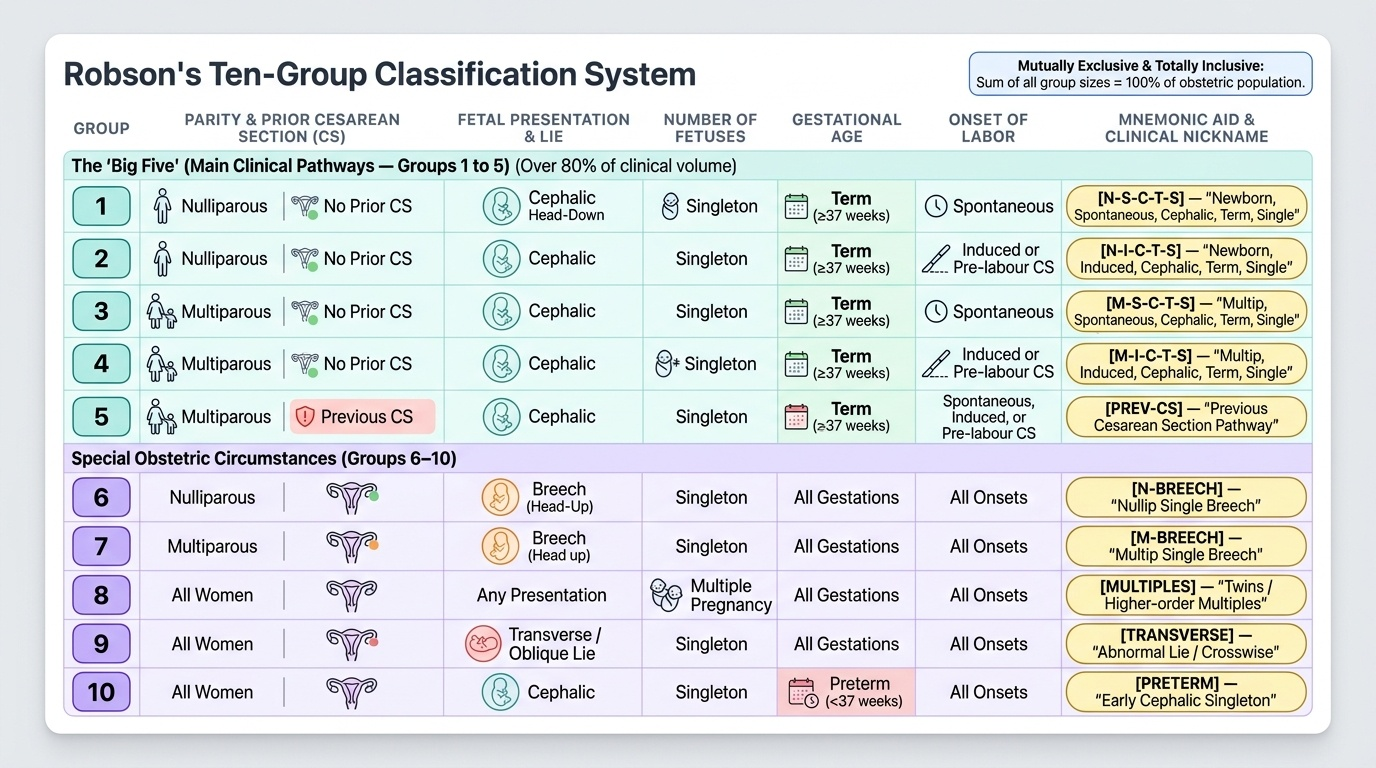
The Robson Ten-Group Classification System (TGCS), first published by Michael Robson in 2001 and adopted by the WHO as the global standard for CS audit in 2015, classifies every obstetric patient into one of exactly 10 mutually exclusive and totally inclusive groups. 'Mutually exclusive' means a patient belongs to only one group; 'totally inclusive' means every patient in the obstetric population can be classified. This property makes the system ideal for audit: the sum of all group sizes equals the total obstetric population, and the CS rates within each group sum to give the overall facility CS rate.
Each group is defined by four obstetric characteristics: (1) parity — nulliparous (no previous delivery ≥20 weeks) or multiparous; (2) previous caesarean section — yes or no; (3) fetal presentation — cephalic, breech, or transverse/oblique; (4) onset of labour — spontaneous, induced, or pre-labour CS; combined with (5) gestational age — term (≥37 weeks) or preterm (<37 weeks); and (6) number of fetuses — singleton or multiple.
The ten groups are:
• Group 1: Nulliparous, singleton, cephalic, ≥37 weeks, spontaneous labour.
• Group 2: Nulliparous, singleton, cephalic, ≥37 weeks, induced or pre-labour caesarean.
• Group 3: Multiparous (excluding previous CS), singleton, cephalic, ≥37 weeks, spontaneous labour.
• Group 4: Multiparous (excluding previous CS), singleton, cephalic, ≥37 weeks, induced or pre-labour caesarean.
• Group 5: Previous caesarean section, singleton, cephalic, ≥37 weeks.
• Group 6: All nulliparous women with a single breech.
• Group 7: All multiparous women with a single breech (including previous CS).
• Group 8: All women with multiple pregnancies (including previous CS).
• Group 9: All women with a singleton, transverse or oblique lie (including previous CS).
• Group 10: All women with a singleton, cephalic, preterm pregnancy (including previous CS).
Groups 1–5 represent the five main clinical pathways (the 'big five') accounting for the vast majority of all deliveries in any obstetric population. Groups 6–10 cover special obstetric circumstances. The 'modified Robson classification' referenced in NMC OG1.4 is this WHO-standardised version (identical to the original Robson groups — 'modified' in some Indian texts refers to minor adaptations for local record formats, not to any change in the group definitions).
Provided image
SELF-CHECK
A woman delivers her second baby (no previous CS) at 39 weeks. She was induced for gestational hypertension. She had a cephalic singleton. Which Robson group does she belong to?
A. Group 1 (nulliparous, spontaneous)
B. Group 3 (multiparous, no previous CS, spontaneous)
C. Group 4 (multiparous, no previous CS, induced or pre-labour CS)
D. Group 5 (previous CS)
Reveal Answer
Answer: C. Group 4 (multiparous, no previous CS, induced or pre-labour CS)
This woman is multiparous (second delivery), has no previous CS, has a singleton cephalic fetus at term (≥37 weeks), and her labour was induced — placing her in Group 4. Group 3 requires spontaneous labour onset. Group 1 is for nulliparous women. Group 5 is for women with a previous CS.
Conducting a Caesarean Section Audit Using Robson TGCS
A Robson TGCS audit is a prospective or retrospective analysis of all deliveries in a defined period at a given facility, designed to answer the question: where is our overall caesarean section rate coming from, and is any of it modifiable? To conduct the audit, you need three pieces of data for every delivery: the mode of delivery (vaginal or caesarean), the Robson group (derived from the four defining characteristics documented at the time of delivery), and the total denominator — the total number of deliveries in the audit period. The audit then computes, for each of the ten Robson groups, three layered metrics that together tell the full story of the facility's CS rate. Understanding all three metrics is essential: a facility that looks only at within-group CS rates misses the size effect; one that looks only at group sizes misses the clinical practice signal. The combination of group size and within-group CS rate is what determines the group's actual impact on the facility's overall rate.
From these, for each group, three metrics are calculated:
- Group CS rate = (CS deliveries in that group ÷ total deliveries in that group) × 100. This is the within-group rate — it tells you how often women in this clinical category end up with a caesarean at your facility.
- Relative group size = (Total deliveries in that group ÷ total obstetric population) × 100. This tells you what proportion of your population falls into this group.
- Absolute contribution to the overall CS rate = (CS deliveries in that group ÷ total obstetric population) × 100. This is the most policy-relevant metric: it identifies which groups have the largest impact on your overall CS rate, taking into account both the group-specific CS rate and the group's size.
To identify where to focus audit interventions, rank groups by their absolute contribution. A group with a high within-group CS rate but a very small relative size (e.g., Group 9 — transverse lie — which has a near-100% CS rate but is rare) contributes little to the overall rate. Conversely, a group with a moderate CS rate but a large relative size can be the dominant driver.
In India, as in many high-income and upper-middle-income countries, Group 5 (previous caesarean, term, cephalic singleton) and Group 2 (nulliparous, term, induced or pre-labour CS) are typically the largest contributors to the overall CS rate. Group 5's high CS rate reflects the common 'once a CS, always a CS' practice pattern — VBAC (vaginal birth after caesarean) is underutilised in many facilities. Group 2's contribution reflects high induction rates and a tendency to convert inductions to CS when progress is slow. Targeting these two groups — by promoting appropriate VBAC counselling and improving induction management — is the evidence-based audit response in the Indian context.
The Robson system also enables inter-facility and inter-country benchmarking: because every facility classifies patients identically, a facility in a rural district can compare its Group 1 CS rate against a tertiary teaching hospital, making case-mix-adjusted comparisons meaningful.
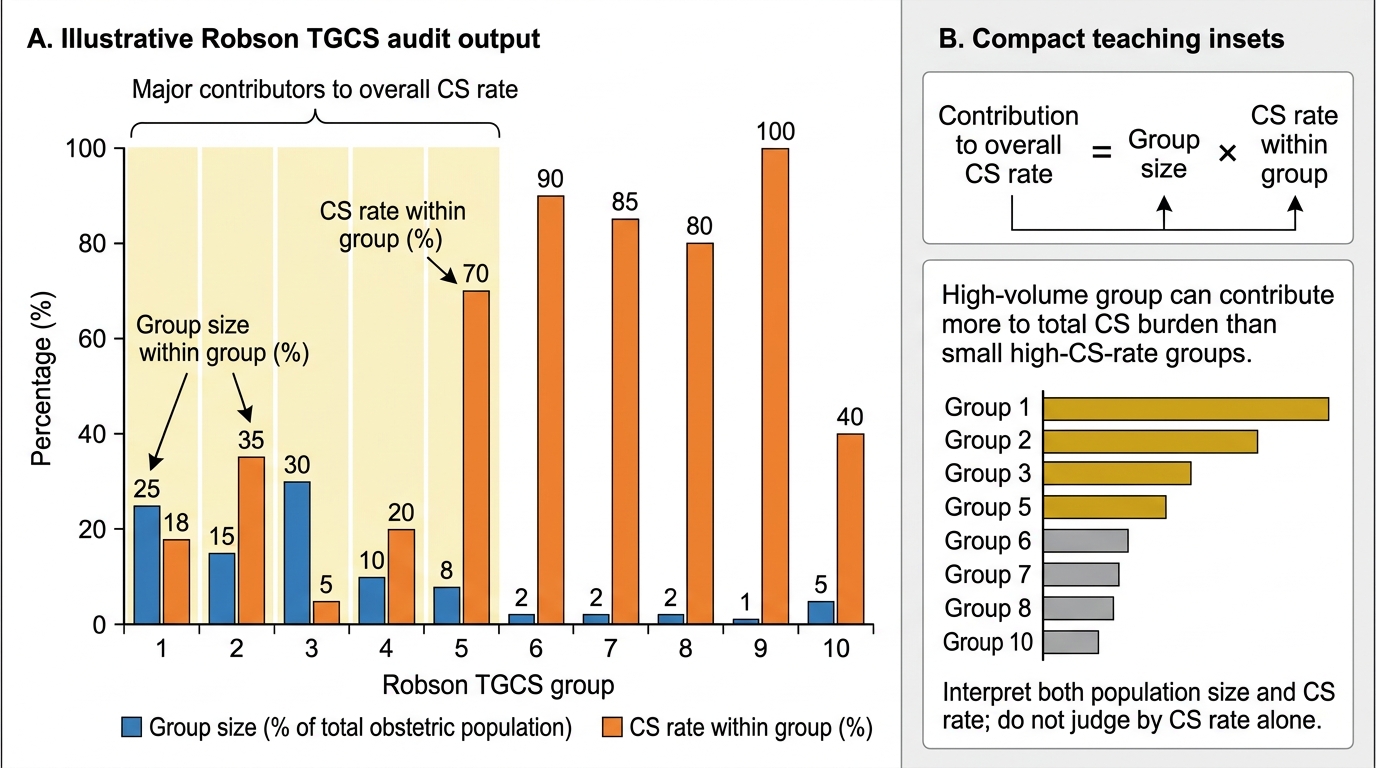
Illustrative Robson TGCS Audit Output