Page 6 of 32
OG17.2 | Breastfeeding Counselling — SDL Guide (Part 2)
Achieving and Correcting a Correct Latch
The latch is the single most critical determinant of breastfeeding comfort and effectiveness — a poor latch is the root cause of nipple trauma, inadequate milk transfer, engorgement, early lactation failure, and ultimately breastfeeding cessation in the first weeks. Teaching a correct latch is therefore the centrepiece of every breastfeeding counselling interaction, and the technical steps below should be practised until they are second nature. The anatomy reviewed in the previous section underpins every step: the infant must compress the lactiferous sinuses beneath the areola, not just the nipple tip; the tongue must lie flat and anterior to perform its peristaltic extraction action; the chin must be the first contact point, ensuring the lower jaw captures maximum areolar tissue; and the latch must be asymmetric, with more tissue taken from the lower areola than the upper. Mastering these principles transforms latch teaching from a mechanical checklist into an anatomically reasoned intervention.
Steps to achieve a correct latch:
- Position the mother comfortably (chair with back support; pillow under arm if needed; feet flat on the floor).
- Position the infant tummy-to-tummy, head at breast level, in the chosen hold.
- Hold the breast in a C-hold, thumb above, fingers below, well behind the areola.
- Stroke the infant's upper lip or philtrum with the nipple — wait for a wide gape (wide open mouth, tongue down, chin forward). Do NOT push the infant onto the breast; wait for the gape.
- When the gape is wide, bring the infant quickly to the breast with a scooping motion, leading with the chin (the chin touches the breast first, below the nipple).
- The infant's lower jaw should take the largest bite — more lower areola in the mouth than upper areola.
Signs of a correct latch:
- Baby's mouth is wide open (>100–120° gape)
- Chin touching breast, nose clear or just touching
- Lower lip flanged outward (not tucked in)
- Cheeks rounded and full (not sucked-in/dimpled)
- More areola visible above the upper lip than below the lower lip (asymmetric latch)
- Audible rhythmic swallowing after initial rapid suck bursts
- No pain beyond initial mild discomfort in the first 30–60 seconds
Signs of a poor latch:
- Nipple-only feeding (infant mouth on nipple tip only)
- Infant cheeks dimpled inward (air in, milk out — wrong)
- Clicking sounds (air leaking from a broken seal)
- Infant's chin not touching breast
- Maternal nipple pain throughout the feed and post-feed nipple distortion (stripe, wedge, or lipstick shape)
Correcting a poor latch: Break the latch by inserting a clean finger at the corner of the infant's mouth to release suction (to avoid nipple abrasion from pulling the baby off). Reposition and re-attempt. Repeat until comfortable for the mother.
| Feature | Good Latch | Poor Latch |
|---|---|---|
| Mouth opening | Wide (>100°) | Narrow, pursed |
| Areola coverage | Asymmetric — more below | Symmetric or nipple-only |
| Chin position | Touching breast | Not touching breast |
| Cheeks | Rounded, full | Dimpled, sucked-in |
| Sound | Rhythmic swallowing | Clicking, smacking |
Care of the Breast: Nipple Problems, Engorgement, and Expressed Milk
Breast care is an integral part of breastfeeding counselling that is often underemphasised. The most common problems encountered in the first two weeks of lactation — nipple soreness, breast engorgement, and difficulties with milk expression — are each preventable or manageable with correct technique, but only if the counsellor and mother recognise them early and respond appropriately. Failure to address these problems is one of the principal reasons breastfeeding is abandoned in the critical first weeks, even when the mother has strong motivation to continue. Systematic teaching of breast care skills on the postnatal ward, before problems arise, is far more effective than reactive management after the mother is already in pain or distress. This section covers the three most common breast care issues in the postnatal period.
Nipple soreness: Mild discomfort in the first few suckles is normal as the nipple is drawn deep into the infant's mouth. However, persistent pain throughout the feed, or pain that does not improve by day 3–4, indicates a latch problem. Management of latch-related nipple soreness:
- Correct the latch before persisting with the feed
- Express a few drops of hind-milk after each feed and apply to the nipple (contains fat and has skin-soothing and antimicrobial properties)
- Allow nipples to air-dry after feeds
- Purified lanolin (anhydrous) applied sparingly after feeds reduces friction and promotes moist wound healing
- Nipple shields (thin silicone) may provide temporary pain relief but reduce milk transfer and should not be used long-term without lactation consultant input
Breast engorgement occurs 2–5 days postpartum when the transition to copious milk production (lactogenesis II) is accompanied by vascular congestion. It presents as bilateral, firm, painful, warm breasts that may be so engorged that the nipple is flattened and the infant cannot latch. Management:
- Warm compress or warm shower immediately before feeds (promotes vasodilation and let-down)
- Gentle breast massage and hand expression to soften the areola before the feed (the reverse pressure softening technique — gentle pressure on the areola for 1–2 minutes to displace oedema fluid)
- Frequent, effective feeding is the treatment — emptying the breast reduces back-pressure
- Cold compress (ice pack wrapped in cloth) after feeds for pain relief and to reduce oedema
- Engorgement is NOT an indication for antibiotics (no infection present)
Hand expression is a critical skill the mother must learn: form a C-hold with thumb and forefinger 2–3 cm behind the nipple, compress toward the chest wall, then roll fingers forward toward the nipple. Collect expressed milk in a clean cup (cup-feeding preferred to bottles for supplementation to avoid nipple-teat preference). Expressed breast milk can be stored at room temperature for 4–6 hours, in a refrigerator for 3–5 days, or frozen for up to 6 months.
SELF-CHECK
A mother on day 2 postpartum is feeding her term neonate. On observation, you note the baby's cheeks are dimpled inward and the mother reports a clicking sound. The baby appears frustrated and is not gaining expected weight. What is the most likely problem and the most appropriate immediate action?
A. Insufficient milk supply — advise formula supplementation
B. Poor latch — break the seal, reposition and re-latch with a wider gape
C. Breast engorgement — apply warm compresses and offer expressed milk
D. Neonatal oral aversion — refer to neonatology
Reveal Answer
Answer: B. Poor latch — break the seal, reposition and re-latch with a wider gape
Dimpled cheeks and clicking sounds are classic signs of a poor latch — the infant is getting air in rather than milk out. The correct first action is to break the latch (insert a finger at the corner of the mouth to release suction) and re-latch with a wider gape and correct asymmetric deep latch. Formula supplementation is not indicated for a latch problem and would reduce breastfeeding demand, blunting prolactin and undermining galactopoiesis.
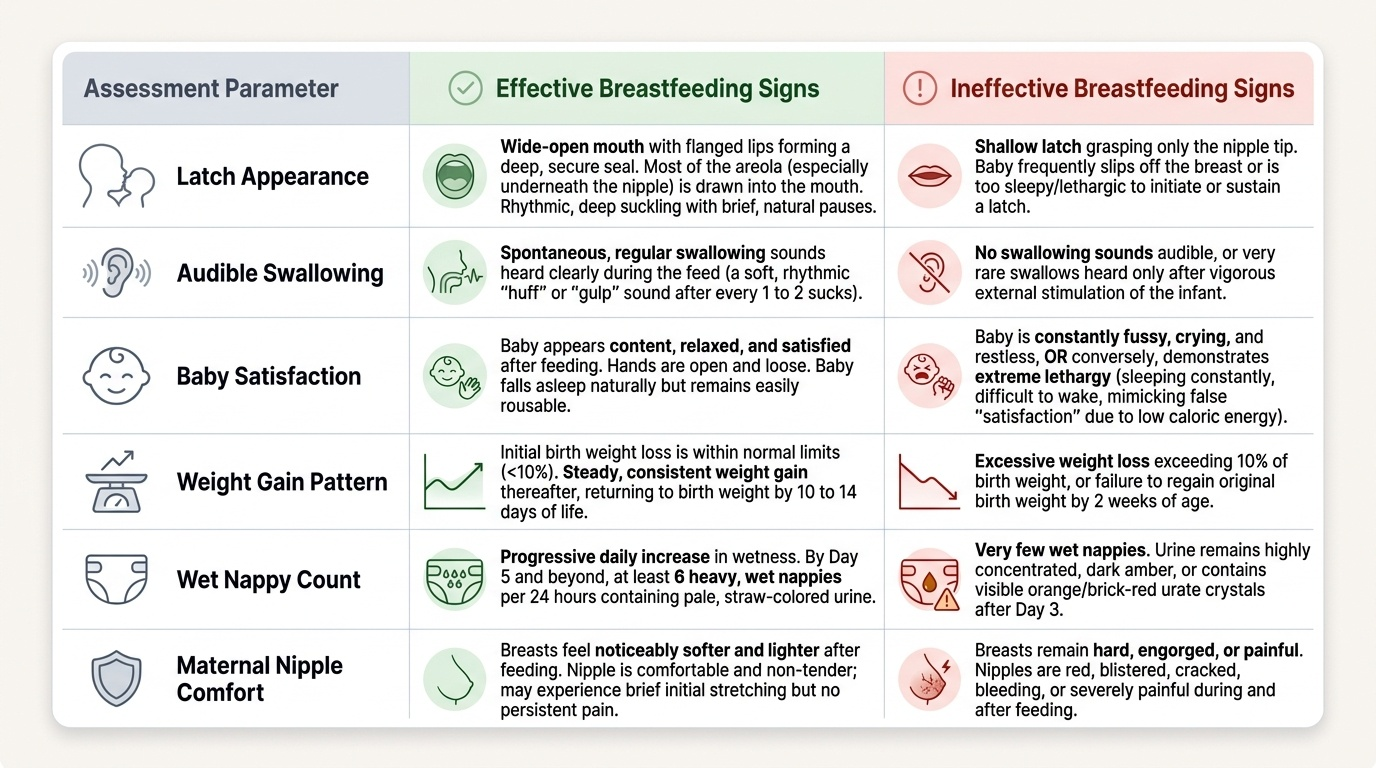
Interpreting Feeding Signs: Effective vs Ineffective Breastfeeding
Assessing whether a breastfeed is effective is a core postnatal ward skill that must be performed systematically and documented. Both direct observational signs — what you see and hear during the feed itself — and indirect markers — what the infant demonstrates over the subsequent 24 hours in terms of weight, urine output, and behaviour — contribute to this assessment. Relying on the mother's subjective report alone is insufficient; mothers who report 'the baby seems satisfied' may have an infant who is lethargic from poor caloric intake rather than genuinely satisfied. Conversely, a baby who cries frequently is not necessarily underfed. The LATCH score is a structured, five-item validated tool that formalises bedside breastfeeding assessment into a reproducible numeric score, enabling consistent communication across the nursing team and tracking of progress over successive feeds.
The LATCH assessment tool (0–2 per item, maximum 10):
- L — Latch: 0 = too sleepy or not latching; 1 = repeatedly falls off, sustained with help; 2 = grasps breast, rhythmic suckling, holds latch
- A — Audible swallowing: 0 = none; 1 = few, with stimulation; 2 = spontaneous and frequent
- T — Type of nipple: 0 = inverted; 1 = flat; 2 = everted after stimulation
- C — Comfort (nipple/breast): 0 = engorged or cracked, bleeding; 1 = filling/reddened/small blisters; 2 = soft, non-tender
- H — Hold (positioning): 0 = full assist needed; 1 = minimal assist needed; 2 = no assist needed
A score of ≥8 indicates effective breastfeeding. Scores below 8 identify specific areas for targeted support.
Signs of effective breastfeeding (global assessment beyond LATCH):
- Audible, rhythmic swallowing (typically after the initial rapid non-nutritive suck bursts trigger let-down)
- Baby appears satisfied, relaxed, and often sleepy after feeds; fists unclenched
- Adequate wet nappies: ≥1 per day of life (days 1–3), then ≥6 wet nappies per 24 h from day 4–5 onward
- Stools: meconium transitions to yellow seedy stools by day 3–5
- Birth weight regained by day 10–14 (maximum acceptable loss is 7–10% of birth weight in the first days)
Red flags for inadequate milk transfer:
- Persistent excessive crying between feeds
- Fewer than 6 wet nappies per day beyond day 4
- Weight loss >10% of birth weight, or failure to regain birth weight by day 14
- Persistent jaundice (may indicate inadequate caloric intake and stool output)
Differential for nipple pain (beyond poor latch):
- Thrush/candida (burning pain, itching, white patches on infant tongue) — treat both mother and infant simultaneously with nystatin or miconazole
- Bacterial infection (cracked nipple acting as portal) — presents later, may require antibiotics
- Raynaud's phenomenon of the nipple (triphasic colour change: white → blue → red after feed)
Provided image
SELF-CHECK
Using the LATCH scoring tool, a nurse records: L=1 (falls off repeatedly), A=1 (few swallows with stimulation), T=2 (normal nipple), C=1 (reddened), H=1 (minimal assist). What is the total LATCH score and what does it indicate?
A. Score 5 — breastfeeding is effective and no further support is needed
B. Score 6 — breastfeeding is suboptimal and requires targeted support
C. Score 7 — borderline but adequate; reassess in 24 hours
D. Score 8 — effective breastfeeding; no intervention indicated
Reveal Answer
Answer: B. Score 6 — breastfeeding is suboptimal and requires targeted support
L(1)+A(1)+T(2)+C(1)+H(1) = 6. A LATCH score below 8 indicates suboptimal breastfeeding that requires targeted support. The low scores in latch (L=1), swallowing (A=1), and comfort (C=1) specifically suggest a latch technique problem as the root cause, warranting a hands-on positioning and latch correction session.