Page 21 of 32
OG19.1 | Normal and Abnormal Puerperium — SDL Guide (Part 2)
Puerperal Sepsis: Pathophysiology and Diagnosis
Puerperal sepsis is defined by the WHO as infection of the genital tract occurring at any time between the onset of rupture of membranes or labour and the 42nd day postpartum, with two or more of the following: pelvic pain, fever (oral temperature ≥38.5°C), abnormal vaginal discharge (colour, smell), sub-involution of the uterus. It is the most dangerous infectious complication of the puerperium and accounts for approximately 10–15% of maternal deaths worldwide. The pathophysiology begins with a breach of the normal anatomical barriers — raw placental site, trauma to the vagina, cervix, or perineum from delivery — that allows colonising bacteria to ascend or directly infect pelvic structures. Understanding this mechanism is clinically useful: risk factors that enlarge the breach (prolonged labour, multiple vaginal examinations, instrumental delivery, manual removal of placenta, retained products) directly increase the probability of sepsis, and recognising these risk factors in the antenatal and intrapartum records helps the clinician maintain a lower threshold for investigation in the puerperium.
The principal causative organisms differ between community-acquired and healthcare-associated infection:
• Gram-positive: Streptococcus pyogenes (Group A beta-haemolytic streptococcus — historically the most lethal puerperal pathogen, capable of causing fulminant septic shock within hours; notifiable disease), Staphylococcus aureus (wound infections, mastitis, MRSA concerns), Streptococcus agalactiae (Group B strep).
• Gram-negative: Escherichia coli (most common overall; ascending from the rectovaginal flora), Klebsiella, Pseudomonas.
• Anaerobes: Bacteroides fragilis, Peptostreptococcus (polymicrobial infection from retained products).
The pathophysiological cascade: local endometritis → parametritis (spread to broad ligament/parametrium) → peritonitis → bacteraemia/septicaemia → septic shock (distributive: vasodilation, capillary leak, hypotension unresponsive to fluids) → multi-organ failure (renal, hepatic, DIC). The speed of progression depends on the organism: Group A streptococcus (GAS) can progress from fever to septic shock within 12–24 hours, making rapid recognition imperative.
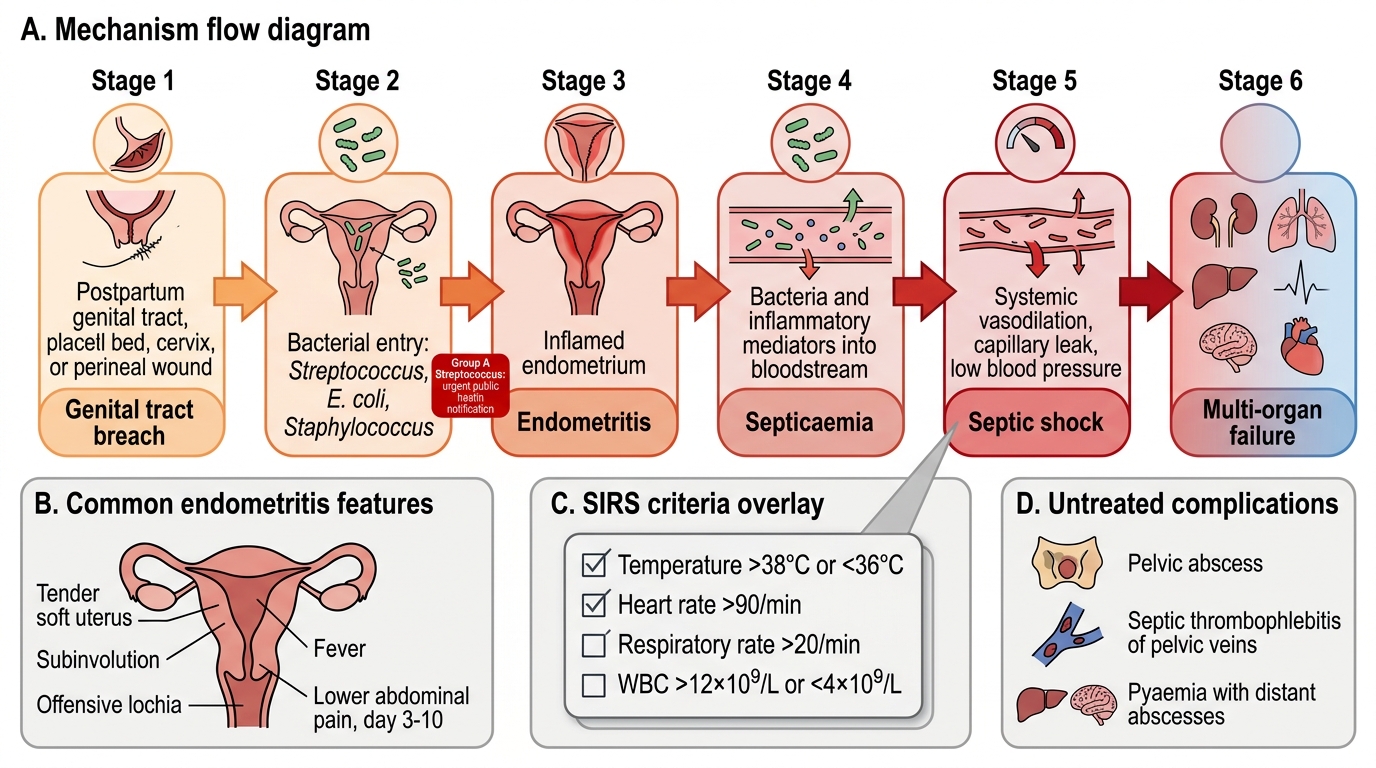
Puerperal Sepsis Pathophysiology and SIRS Criteria
Diagnostic criteria for sepsis in the puerperium use the same SIRS (Systemic Inflammatory Response Syndrome) framework as general medicine: temperature >38°C or <36°C, heart rate >90/min, respiratory rate >20/min, white cell count >12×10⁹/L or <4×10⁹/L. The clinical picture of endometritis — the most common manifestation — includes tender, soft, subinvoluted uterus, offensive lochia, fever, and lower abdominal pain, typically arising day 3–10. Complications of untreated sepsis include pelvic abscess, septic thrombophlebitis of pelvic veins, and pyaemia with distant abscesses.
SELF-CHECK
A primipara on day 4 post-vaginal delivery develops a temperature of 39°C, offensive lochia, and uterine tenderness. Blood cultures are sent. Which organism, if isolated, should prompt IMMEDIATE notification to public health authorities due to its potential for fulminant maternal collapse?
A. Escherichia coli
B. Staphylococcus aureus
C. Group A beta-haemolytic Streptococcus (Streptococcus pyogenes)
D. Bacteroides fragilis
Reveal Answer
Answer: C. Group A beta-haemolytic Streptococcus (Streptococcus pyogenes)
Group A beta-haemolytic streptococcus (Streptococcus pyogenes) is the historically most lethal puerperal pathogen and can cause fulminant septic shock within hours. It is a notifiable disease. While E. coli is the most common overall cause of puerperal sepsis, GAS requires the most urgent response. Staphylococcus and Bacteroides are important but less likely to cause rapid deterioration.
Management of Puerperal Complications: Sepsis, Secondary PPH and Subinvolution
Management of puerperal complications follows the principle of identifying the underlying cause first, then treating specifically while providing supportive care. In puerperal sepsis, the Sepsis Six bundle (from general medicine) applies: high-flow oxygen, IV access and blood cultures before antibiotics, broad-spectrum IV antibiotics within ONE hour, IV fluid resuscitation (crystalloid 30 mL/kg if hypotensive), serial lactate measurement, and hourly urine output monitoring. Antibiotic choice must cover the full polymicrobial spectrum: broad-spectrum penicillin (amoxicillin-clavulanate) PLUS metronidazole covers most community-acquired puerperal sepsis; if Group A streptococcus is suspected, high-dose IV benzylpenicillin is the drug of choice. Severely ill patients may require a carbapenem. If the uterus contains retained products, surgical evacuation (evacuation of retained products of conception, ERPC) is essential — antibiotics alone are insufficient. Transfer to the intensive care unit is indicated for septic shock.
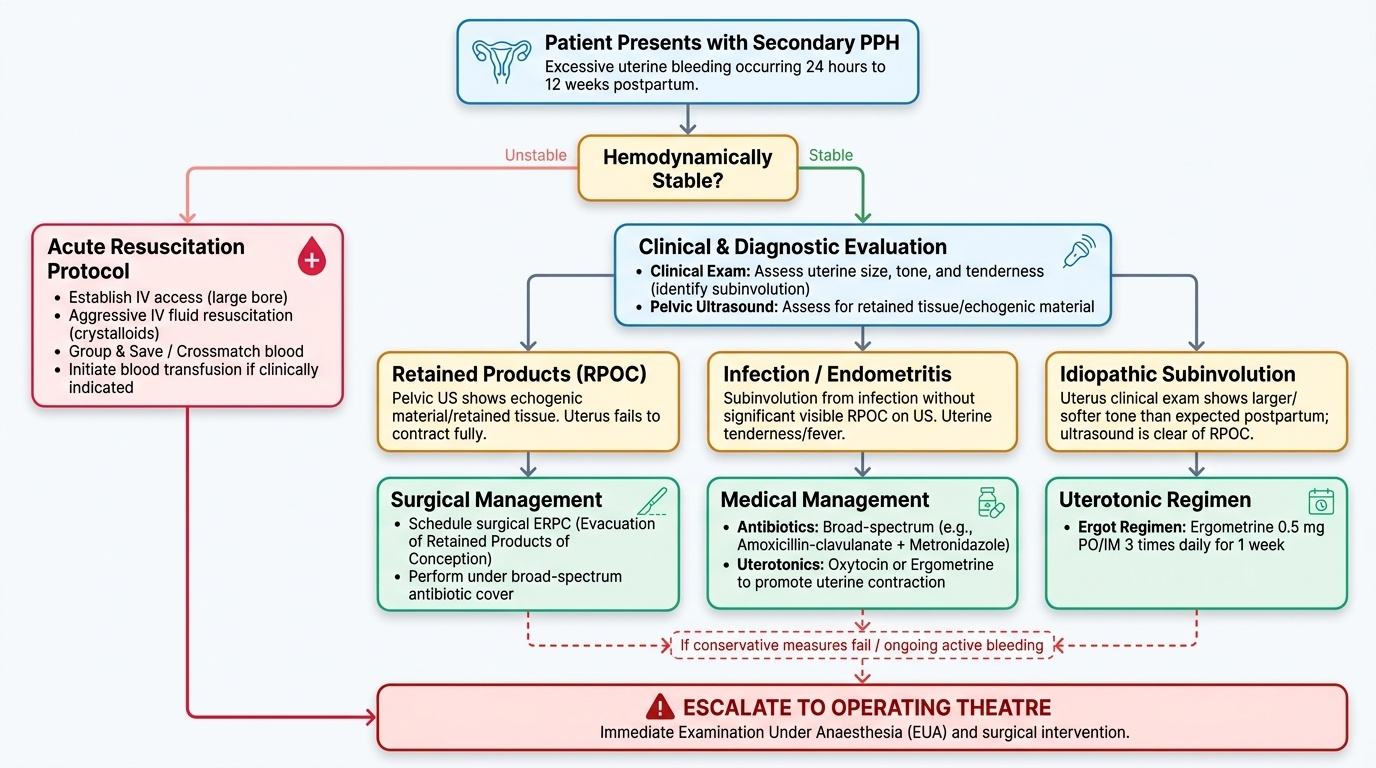
Secondary PPH is defined as excessive uterine bleeding occurring from 24 hours to 12 weeks after delivery. The two principal causes are: (1) retained products of conception (RPOC) — the retained tissue prevents full myometrial contraction and acts as a nidus for infection, diagnosed by pelvic ultrasound showing echogenic material in the uterine cavity; treated by surgical ERPC under antibiotic cover. (2) Infection/endometritis — subinvolution from infection even without visible RPOC; treated with antibiotics and uterotonics (oxytocin, ergometrine). In the acute episode, resuscitate with IV fluids and blood transfusion if haemodynamically unstable; examine under anaesthesia if conservative measures fail.
Subinvolution (failure of the uterus to involute at the expected rate) is diagnosed clinically: uterus larger and softer than expected for the day postpartum. The causes are the same as secondary PPH — RPOC and infection are the most common. Assess with pelvic ultrasound. Treat the underlying cause: ERPC for RPOC, antibiotics for endometritis, uterotonics (ergometrine 0.5 mg 3 times daily for 1 week — the 'ergot regimen') for idiopathic subinvolution.
Provided image
Puerperal Psychological Disorders: Blues, Depression and Psychosis
The postpartum period carries the highest risk of new-onset psychiatric illness across a woman's reproductive lifespan. Three distinct clinical entities exist along a spectrum of severity, and their differentiation is clinically important because management differs fundamentally. All three are underdiagnosed in resource-limited settings where follow-up is infrequent after the postnatal discharge check.
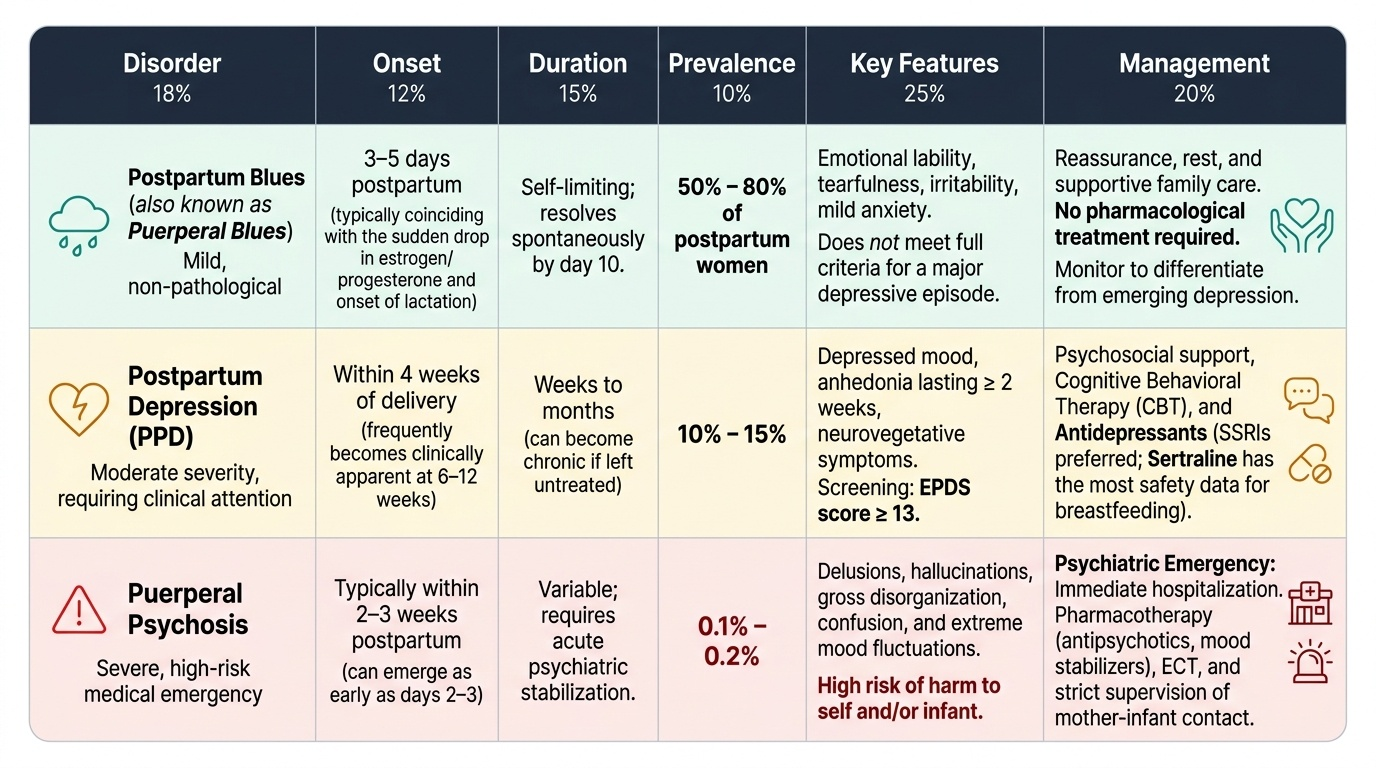
Postpartum (puerperal) blues is an extremely common, normal-variant mood disturbance affecting 50–80% of postpartum women. It typically peaks on days 3–5 after delivery, coinciding with hormonal changes (particularly the precipitous fall in oestrogen and progesterone) and the onset of milk let-down. The woman experiences emotional lability, tearfulness, irritability, and anxiety without meeting criteria for a depressive episode. It is self-limiting by day 10 and requires only reassurance, rest, and supportive care. No pharmacological treatment is needed. The primary clinical action is to distinguish it from the emerging symptoms of postpartum depression.
Postpartum depression (PPD) affects approximately 10–15% of women and is defined by a depressive episode (per DSM-5 criteria: depressed mood or anhedonia ≥2 weeks, with neurovegetative symptoms) with onset within 4 weeks of delivery. However, many cases become clinically apparent at 6–12 weeks. Screening uses the Edinburgh Postnatal Depression Scale (EPDS); a score of ≥13 is the standard screening threshold. Management includes psychosocial support, cognitive behavioural therapy, and antidepressants (SSRIs are preferred if pharmacotherapy is needed; sertraline has the most safety data in breastfeeding women — excreted minimally in breast milk). It is critical NOT to dismiss PPD as 'just blues' — untreated PPD has profound consequences for maternal bonding, infant development, and family function.
Puerperal psychosis is the most severe and urgent of the three conditions, with an incidence of approximately 1–2 per 1,000 deliveries. It typically presents within 2 weeks of delivery (often as early as days 2–4) with acute onset of psychotic symptoms: hallucinations (often visual and auditory), delusions (often centred on the baby — believing the baby is defective, possessed, or must be harmed), disorganised behaviour, and confusion. There is a real risk of infanticide and maternal suicide. Puerperal psychosis is a psychiatric emergency requiring immediate hospital admission, ideally to a mother-and-baby unit, with urgent psychiatric assessment. Management is with antipsychotic medication (haloperidol, olanzapine) and, where available, ECT for refractory cases. Women with a prior history of bipolar disorder or previous puerperal psychosis have a recurrence risk of approximately 50% and require prophylactic management.
Provided image
SELF-CHECK
A woman at day 12 postpartum is brought in by her husband who is concerned that she has not slept for 3 days, is speaking incoherently, believes the baby is 'possessed,' and attempted to throw the baby out of a window. The most appropriate immediate management is:
A. Reassurance — this is postpartum blues, which is self-limiting
B. Start an SSRI and review in 2 weeks
C. Immediate psychiatric admission as a medical emergency, with risk assessment for infant safety
D. Ergometrine 0.5 mg three times daily for 1 week
Reveal Answer
Answer: C. Immediate psychiatric admission as a medical emergency, with risk assessment for infant safety
This is puerperal psychosis: acute psychotic symptoms, delusions centred on the baby, dangerous behaviour, onset within 2 weeks. It is a psychiatric emergency with risk of infanticide and maternal suicide. Immediate admission is mandatory. Postpartum blues is self-limiting and does not produce psychosis or dangerous behaviour. SSRIs are for postpartum depression. Ergometrine is a uterotonic, not a psychiatric drug.
CLINICAL PEARL
The single most underappreciated clinical sign in the puerperium is the offensive-smelling lochia. Textbooks describe it, but students on the ward sometimes fail to examine and describe lochia systematically. Any foul odour — regardless of the quantity of discharge or the degree of fever — should be treated as endometritis until proven otherwise, because Group A streptococcus can cause a catastrophically rapid deterioration. The second underappreciated danger is puerperal psychosis: the window from unusual behaviour to infanticide can be very short. Any new-onset psychotic symptoms postpartum must be treated as an emergency, not a social or cultural issue. Involve the psychiatric team immediately.