Page 5 of 28
OG20.2 | MTP Consent — SDL Guide
Learning Objectives
- Describe the legal and ethical framework governing informed consent for Medical Termination of Pregnancy
- Administer a structured consent consultation for MTP in a simulated environment, covering all five elements of informed consent
- Identify situations where consent may be compromised, coerced, or requires a guardian
- Document consent appropriately for MTP in a medical record
INSTRUCTIONS
Obtaining valid informed consent for MTP is a distinct clinical skill — not a routine signature on a form. The woman requesting MTP may be frightened, under external pressure, uncertain of her decision, or legally incapable of consenting alone. This module teaches you the legal framework, the structured technique for a consent consultation, the warning signs of compromised consent, and how to manage special situations such as minors and women of unsound mind. You will practice through worked role-play scenarios.
References
- DC Dutta's Textbook of Obstetrics, 9th ed., Chap 14 (MTP — consent provisions) (textbook)
- MTP Act 1971 (amended 2021) and MTP Rules 2021 — Section 3 and Section 5A (confidentiality) (guideline)
- NMC Code of Ethics for Registered Medical Practitioners, 2023 (guideline)
- FOGSI MTP Consent Guide, 2022 (guideline)
- WHO Consolidated Guideline on Self-Care Interventions for Health: Sexual and Reproductive Health and Rights, 2022 — Chapter on Consent (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 16-year-old girl presents to your gynaecology outpatient clinic accompanied by her 32-year-old boyfriend. She is 10 weeks pregnant and wants an MTP. The boyfriend insists on signing the consent form 'to save time.' The girl is quiet throughout and does not make eye contact. How do you proceed? Can the boyfriend sign? What if she refuses to speak in front of him? This scenario encapsulates the specific vulnerabilities that make MTP consent a skill, not a formality.
WHY THIS MATTERS
Competency OG20.2 requires you to administer informed consent for MTP in a simulated environment — this is a performative skill, not just declarative knowledge. In clinical practice, a poorly obtained consent exposes the patient to undisclosed risks, may indicate a coerced or unwanted procedure, and exposes the practitioner to legal liability. India's NMC Code of Ethics and the MTP Act both impose specific consent obligations, including who may consent, when a guardian is required, and how confidentiality must be maintained. Mastering this skill protects both the patient and the practitioner.
RECALL
Recall from your Professional Development and Medical Ethics modules: Informed consent requires (1) disclosure of information relevant to the decision, (2) the patient's comprehension of that information, (3) voluntariness — freedom from coercion, (4) decision-making capacity — the cognitive and legal ability to consent, and (5) explicit authorisation or refusal. A signature on a form without all five elements is not valid consent. Also recall: under Indian law, a minor is a person below 18 years; the Indian Contract Act sets 18 as the age of contractual capacity.
Why MTP Consent Is Different: Clinical and Ethical Stakes
Informed consent for MTP differs from consent for a routine surgical procedure in several important dimensions. First, the decision is inherently personal and value-laden — a woman's choice about continuing or terminating a pregnancy engages her deepest values about autonomy, bodily integrity, family, and future. A clinician who treats this as a checklist item rather than a genuine consultation risks both a suboptimal therapeutic relationship and an ethical violation. Second, the social context of MTP creates unique vulnerability to coercion — a partner, parent, or in-law may pressure the woman to terminate a wanted pregnancy or to continue an unwanted one; distinguishing her authentic choice from an imposed one requires skill and sensitivity that a signature alone cannot provide.
Third, the confidentiality provisions of the MTP Act are stronger than for most other procedures. Section 5A of the MTP Act (as amended) mandates that no registered medical practitioner shall reveal the name and other particulars of a woman seeking an MTP to any person except on the order of a competent court. This provision exists because disclosure of MTP status can expose women to stigma, violence, or family rupture — consequences that are not merely inconvenient but dangerous. Understanding this legal protection helps you frame the consent conversation in a way that reassures the woman of her privacy.
Fourth, MTP consent intersects with medicolegal obligations. If the woman is a survivor of sexual assault, the MTP may be part of a medicolegal investigation; if she is a minor, the law requires a guardian to consent. Knowing when to involve a social worker, a child-protection officer, or a legal authority — without violating the woman's trust — is part of this skill.
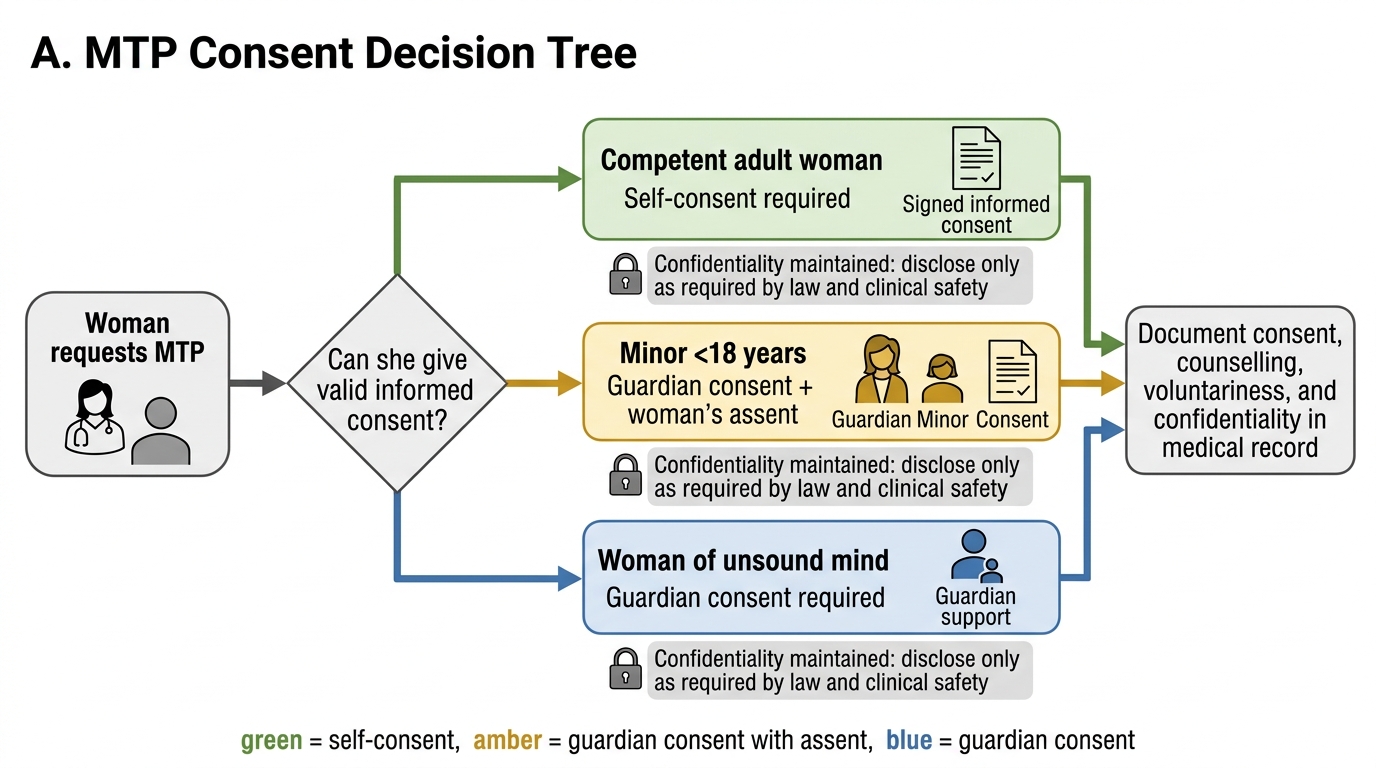
MTP Consent Decision Tree
Legal and Ethical Principles Governing MTP Consent
The MTP Act 1971 (as amended 2021) lays down the legal structure for consent in a way that is both explicit and protective of the woman's interests. The Act's consent provisions were revised substantially in 2021 to reflect modern principles of patient autonomy: the amendment removed the requirement that a husband's or partner's consent be sought for a first-trimester termination (a requirement that had persisted in some interpretations of the original Act), and it extended eligibility to unmarried women and to a broader range of specified categories at 20–24 weeks. Every practitioner performing or assisting with MTP must know three specific provisions precisely, because errors in who consents or how consent is documented carry both medicolegal liability and ethical gravity.
Who may consent:
- A competent adult woman (18 years or older, of sound mind) consents for herself. No one else — not her husband, partner, parent, or in-law — has any legal standing to give or withhold consent on her behalf for a first-trimester or second-trimester MTP within the permitted categories.
- A minor (below 18 years): the guardian's consent is required in writing. Importantly, the woman's own assent should also be obtained — her silence or refusal is a clinical and ethical concern even when the guardian has signed.
- A woman of unsound mind (intellectual disability, severe psychiatric illness affecting capacity): guardian consent is required.
Confidentiality (Section 5A, MTP Act): The woman's identity, particulars, and the fact that she had an MTP must not be disclosed except by court order. This is stronger protection than general medical confidentiality and must be explicitly explained to the woman during the consent process — it directly reduces her fear of social consequences and enables a more open conversation.
Voluntariness in the context of rape or sexual assault: When the pregnancy resulted from sexual assault, the woman's own consent (if she is an adult) is fully sufficient. She does not need a police report, an FIR, or anyone else's endorsement. The law does not require her to have reported the assault to access MTP services.
Documentation: Consent must be recorded, signed (or thumbprint if the woman cannot write), and dated. The form should be part of the medical record and kept confidential. A verbal consent without documentation does not constitute proof of consent in a legal dispute.
From an ethical standpoint, the four principles of biomedical ethics — autonomy, beneficence, non-maleficence, and justice — all converge in MTP consent. Autonomy is operationalised by ensuring the woman makes a free, informed, and uncoerced decision. Beneficence requires that you disclose the benefits and what to expect. Non-maleficence requires disclosure of risks. Justice requires that the same standard of care and respect is offered to all women regardless of age, marital status, or socioeconomic background.
SELF-CHECK
A 28-year-old married woman at 8 weeks requests MTP after contraceptive failure. Her husband is present and says he 'doesn't agree with it.' Which of the following is correct?
A. Proceed with her consent alone — the husband has no legal standing to block MTP
B. The husband's consent is required because she is married
C. Defer the MTP until the couple agrees; arrange marital counselling first
D. Refer to a two-RMP panel because of the marital dispute
Reveal Answer
Answer: A. Proceed with her consent alone — the husband has no legal standing to block MTP
Under the MTP Act 1971 (amended 2021), a competent adult woman consents for herself. The husband has no legal right to veto or authorise her MTP. Requiring a husband's consent was specifically removed from the 2021 amendment framework; it is not required and should not be sought. Her autonomous decision is both legally and ethically sufficient at this gestational age with a single RMP's opinion.
Conducting a Structured MTP Consent Consultation
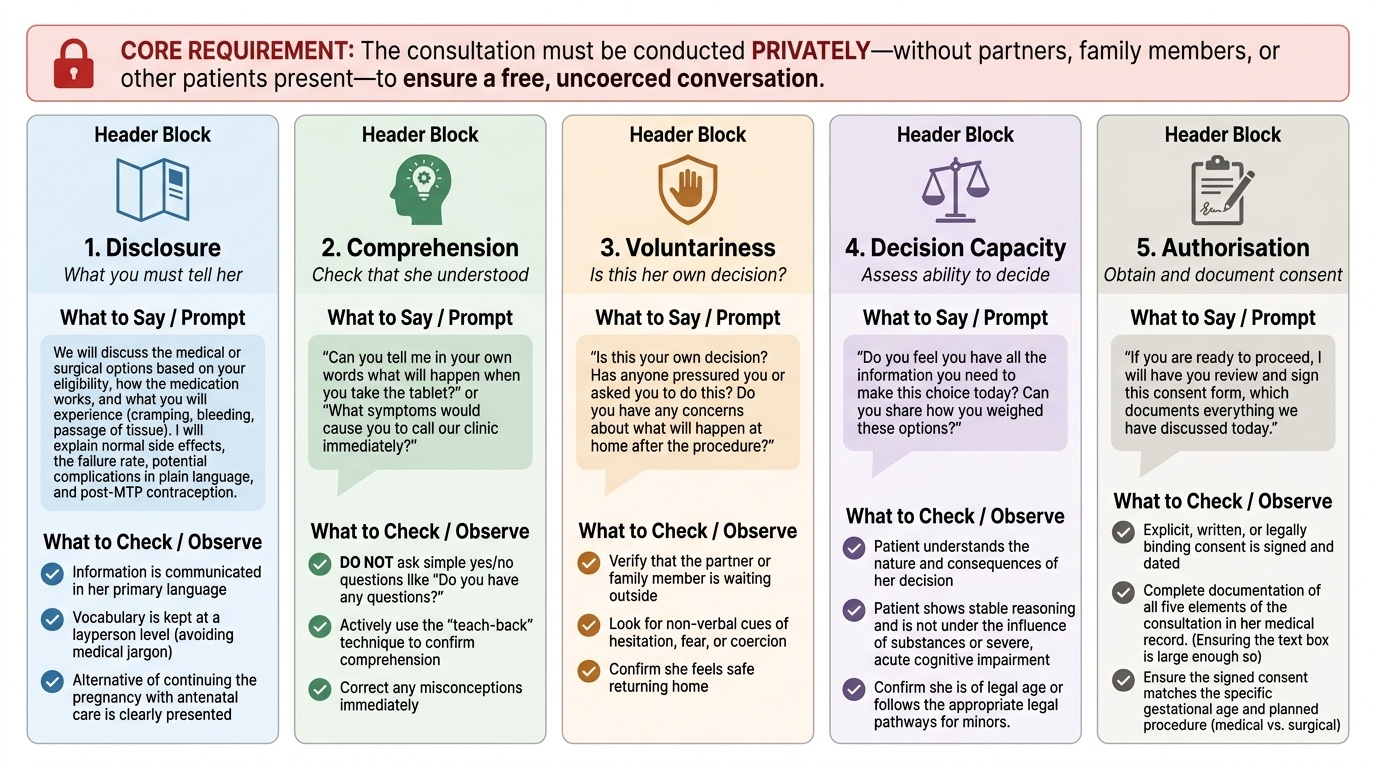
A structured consent consultation for MTP proceeds through five elements, each of which must be addressed explicitly and documented. The consultation should be conducted privately — without partners, family members, or other patients present — to create the conditions for a free, uncoerced conversation. Asking the accompanying person to wait outside is not just courteous; it is clinically necessary to assess voluntariness.
1. Disclosure — What you must tell her:
The nature of the procedure (medical or surgical, depending on gestational age and her eligibility); the expected process (how the medication works, what she will experience, or what the surgical procedure involves); expected side effects and what is normal (cramping, bleeding, passage of tissue); the failure rate and what happens if the procedure fails; possible complications (incomplete abortion, haemorrhage, infection, uterine perforation — risks stated in plain language, not medical jargon); the need for follow-up; post-MTP contraception options; and the alternative of continuing the pregnancy with antenatal care. All of this must be communicated in her primary language and at a vocabulary level she can understand.
2. Comprehension — Check that she understood:
Do not ask 'Do you have any questions?' and move on if she says no. Use a teach-back technique: 'Can you tell me in your own words what will happen when you take the tablet?' or 'What symptoms would you call us about?' This actively confirms understanding rather than assuming it.
3. Voluntariness — Is this her decision?
Ask directly: 'Is this your own decision?' 'Has anyone pressured you or asked you to do this?' 'Do you have any concerns about what will happen at home after the procedure?' Watch for hesitation, anxiety disproportionate to the procedure, or inconsistencies between what she says and her body language. If you suspect coercion, explore it — this is part of the clinical examination.
4. Decision-making capacity:
For most adult women this is assumed present unless there are signs of severe psychiatric illness, intellectual disability, or acute intoxication. If capacity is in doubt, a brief cognitive assessment and, if needed, a psychiatric review may be required before proceeding.
5. Authorisation — Documentation:
The consent form should record: the woman's name (kept confidential), the date, the procedure, the main risks discussed, the alternative options discussed, a statement that she understands and agrees, and her signature or thumbprint. The consulting doctor signs as witness. The form is kept in the medical record in a manner that maintains confidentiality.
Provided image