Page 19 of 28
OG22.1 | Physiological Vaginal Discharge — SDL Guide (Part 2)
Vaginal Microbiome and the Lactobacillus-pH Axis
The healthy vaginal environment is actively maintained by a dynamic interplay between the vaginal epithelium, the hormonal milieu, and the resident microbial community. This is not simply a passive absence of pathogens — it is an actively defended acidic ecosystem in which Lactobacillus species play a central protective role, and whose disruption predisposes directly to the common vaginal infection syndromes covered in the next SDL.
Normal vaginal flora in reproductive-age women is dominated by Lactobacillus species, most commonly Lactobacillus crispatus, L. iners, L. jensenii, and L. gasseri. These are gram-positive rods that ferment the glycogen shed by desquamating vaginal epithelial cells into lactic acid and hydrogen peroxide (H₂O₂). Lactic acid maintains the vaginal pH at 3.8–4.5 — a strongly acidic environment that inhibits the growth of the vast majority of enteric, skin, and sexually transmitted pathogens. H₂O₂ provides additional direct antimicrobial activity. This is the lactobacillus–glycogen–lactic acid axis: oestrogen drives glycogen deposition in epithelial cells → glycogen is metabolised by lactobacilli → lactic acid lowers pH → acid pH inhibits pathogens → lactobacilli thrive.
The quantity of glycogen available to lactobacilli is directly proportional to the level of circulating oestrogen. This explains why the vaginal pH and the protective lactobacillus colonisation vary across physiological states: pre-pubertal girls (low oestrogen) have a near-neutral vaginal pH of 6–7 and no significant lactobacillus colonisation, rendering them more susceptible to vulvovaginitis from skin commensals; postmenopausal women (low oestrogen) similarly lose the glycogen substrate, pH rises, and lactobacilli diminish — the basis of atrophic vaginitis.
Factors that disrupt the lactobacillus–pH axis include: (1) Broad-spectrum antibiotics — kill lactobacilli along with the target pathogen, transiently raising pH and creating an ecological opening for Candida overgrowth (post-antibiotic candidiasis); (2) Alkaline semen (pH 7.2–8.0) — transiently neutralises vaginal acidity after unprotected intercourse; (3) Menstrual blood (pH ~7.4) — temporarily raises vaginal pH during menstruation, a window when bacterial vaginosis and candidiasis are more likely to be triggered; (4) Excessive vaginal douching — physically removes the protective secretions and flora; (5) Hormonal changes — as described, any oestrogen-deficient state (postmenopause, extended breastfeeding, postpartum) reduces glycogen and weakens the protective axis.
Clinical teaching point: a normal vaginal pH of ≤4.5 is one of the most useful chair-side tests in vaginal discharge assessment. A pH >4.5 in a woman with symptomatic discharge strongly suggests bacterial vaginosis or trichomoniasis (both raise pH by consuming acid and producing amines); candidiasis, by contrast, does NOT raise vaginal pH — pH remains ≤4.5 in candidal infection, which is an important diagnostic discriminator.
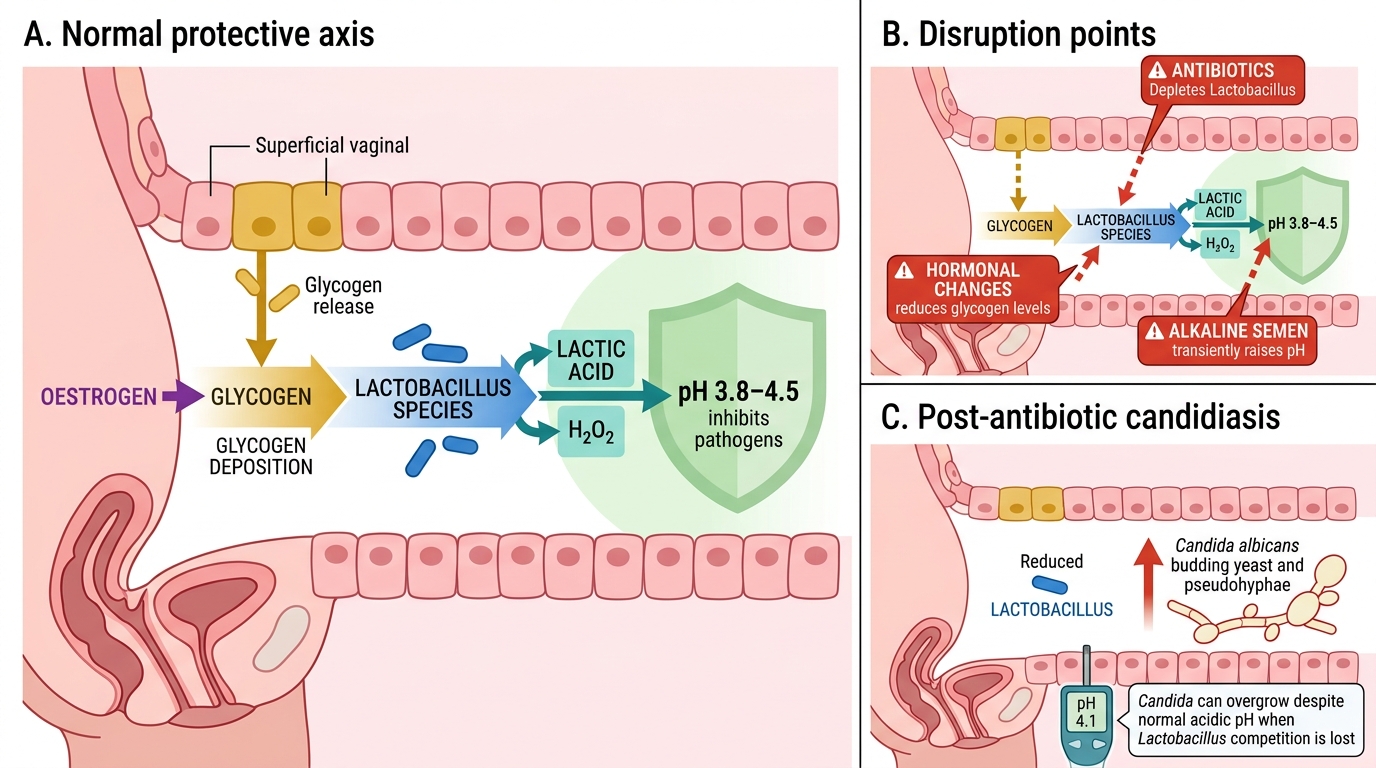
Lactobacillus-Glycogen-Lactic Acid Protective Axis
SELF-CHECK
A 32-year-old woman completed a 7-day course of amoxicillin for a urinary tract infection. Four days after finishing the antibiotics she presents with vulval pruritus and a thick, white, curdy vaginal discharge. Vaginal pH is 4.1. What is the most likely explanation for this sequence of events?
A. The amoxicillin was ineffective and the UTI has spread to cause vaginitis
B. Amoxicillin eradicated Lactobacillus species, raising vaginal pH and enabling Candida overgrowth
C. Amoxicillin eradicated Lactobacillus species; Candida proliferated despite normal (acidic) pH because lactobacilli had been removed
D. The UTI itself caused a secondary candidal vaginitis through urinary contamination of the vagina
Reveal Answer
Answer: C. Amoxicillin eradicated Lactobacillus species; Candida proliferated despite normal (acidic) pH because lactobacilli had been removed
Post-antibiotic candidiasis occurs because broad-spectrum antibiotics (including amoxicillin) deplete Lactobacillus species — the dominant protective flora. With lactobacillus removed, the competitive ecological check on Candida albicans is lost, allowing its overgrowth. Crucially, candidal vaginitis does NOT raise vaginal pH — pH remains ≤4.5 (as seen here at 4.1), because Candida does not produce the amines that alkalinise BV/trichomonas. The curdy white discharge and pruritus are the clinical hallmarks. Option B is incorrect: amoxicillin reduces the H₂O₂-producing protective flora, but pH in candidiasis remains acidic — the mechanism is loss of competitive suppression, not pH change.
Clinical Features of Normal Discharge and Distinguishing from Pathological
The ability to characterise a woman's discharge accurately on history and examination — and to tell her confidently whether it is normal or requires investigation — is a core clinical competency. The preceding sections have established the physiological basis of normal discharge: its four sources, cyclical hormonal variation, and the protective lactobacillus-pH axis. The present section translates that knowledge into a practical bedside assessment framework. The key insight is that normal discharge has a consistent clinical signature — specific colour, consistency, odour, and pH ranges — and that departures from this signature are the diagnostic anchors for each pathological syndrome. Crucially, the framework distinguishes patterns that require no treatment (physiological) from patterns that require specific antimicrobials (bacterial vaginosis, candidiasis, trichomoniasis, or cervicitis). Applying this framework systematically at every discharge consultation prevents both over-treatment of normal secretions and under-treatment of true infections.
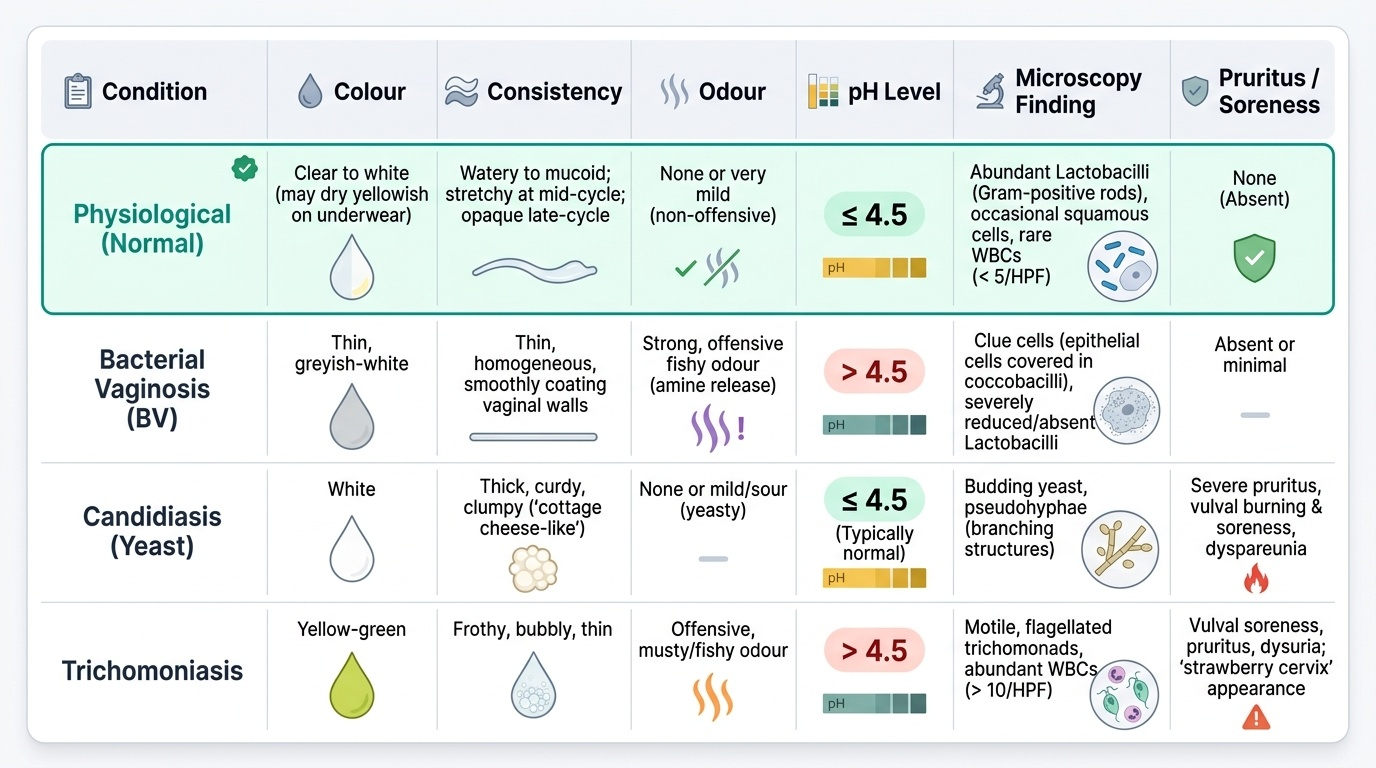
Clinical features of normal (physiological) discharge:
- Colour: clear to white; may be yellowish when dry on underwear (oxidation of cervical mucin — entirely normal)
- Consistency: watery to mucoid; mid-cycle may be stretchy/clear; late cycle more opaque
- Odour: none, or very mild non-offensive smell; absolutely no fishy, yeasty, or offensive odour
- Symptoms: no pruritus, no burning, no vulval soreness, no dyspareunia
- Volume: varies with cycle phase; premenstrual and peri-ovulatory phases produce more
- Vaginal pH: ≤4.5
- Microscopy (if done): lactobacilli (gram-positive rods), occasional squamous cells, rare white cells (<5 per high-power field)
Red flag features that indicate pathological discharge:
- Offensive or fishy odour (bacterial vaginosis — amine release)
- Thick white curdy consistency with pruritus (candidiasis)
- Yellow-green frothy discharge with fishy odour and vulval soreness (trichomoniasis)
- Yellow or mucopurulent discharge from cervical os (cervicitis — gonorrhoea, chlamydia)
- Any blood-stained discharge outside menstruation (intermenstrual/post-coital bleeding must be evaluated)
- Vaginal pH >4.5 (BV, trichomoniasis)
Genital hygiene counselling for women with physiological discharge: (1) External washing with mild soap and water is adequate; vaginal douching is harmful and must be avoided. (2) Breathable cotton underwear helps; tight synthetic fabrics increase local moisture and temperature. (3) Sanitary pads/liners can be worn to protect clothing but do not require a medical rationale; over-reliance on chemical-containing liners may cause contact dermatitis. (4) Changes in discharge noticed after starting a new sexual partner, after antibiotics, or associated with itching/odour should prompt clinical review rather than self-treatment.
Provided image
SELF-CHECK
A woman's vaginal discharge has turned yellowish on her white cotton underwear after drying. She reports the discharge is odourless and non-itchy, and her cycle is regular. What does this colour change on drying most likely represent?
A. Early bacterial vaginosis with amine production
B. Cervical ectropion with mucopurulent secretion from the columnar epithelium
C. Normal oxidation of cervical mucin on contact with air, a physiological finding
D. Evidence of low-grade Trichomonas infection that requires treatment
Reveal Answer
Answer: C. Normal oxidation of cervical mucin on contact with air, a physiological finding
Cervical mucin, when wet, is clear to white. On contact with air, mucin proteins oxidise and the discharge appears yellowish or off-white on underwear. This is a physiological artefact of drying and does not indicate infection. The absence of odour and pruritus confirms there is no bacterial or parasitic cause. Bacterial vaginosis produces a fishy odour (amines); cervical ectropion may cause mucoid discharge but is distinguished on speculum examination; Trichomonas typically causes frothy, malodorous, symptomatic discharge.
Self-Assessment: Physiological Vaginal Discharge
The questions below test your command of the concepts covered in this SDL. They are designed to bridge the descriptive physiology you have just studied to the clinical reasoning you will apply when assessing patients with vaginal discharge. For each question, attempt a written answer before checking your notes — this active retrieval practice strengthens long-term retention far more effectively than re-reading. If any question reveals a gap, return to the relevant section immediately and re-read it before your next clinical exposure. Pay particular attention to questions that ask you to distinguish physiological from pathological findings: this is the core clinical application of everything in this module, and it is the judgement that directly protects patients from both unnecessary treatment and missed infections.
- Name the four anatomical sources that contribute to physiological vaginal discharge, and state which contributes the largest volume.
- A woman's discharge is described as clear, stretchy, and non-offensive, occurring at mid-cycle. Which hormone is predominantly responsible, and what is the term for the stretchability property?
- Explain why the vaginal pH is normally 3.8–4.5 in a reproductive-age woman, and describe the biochemical mechanism by which this is maintained.
- Why does broad-spectrum antibiotic therapy predispose to vulvovaginal candidiasis? What pH finding would you expect in a woman presenting with post-antibiotic candidal discharge?
- A 50-year-old postmenopausal woman complains of increased vaginal discharge with a pH of 5.8 and no odour or pruritus. What physiological change explains the raised pH, and what is the likely diagnosis?
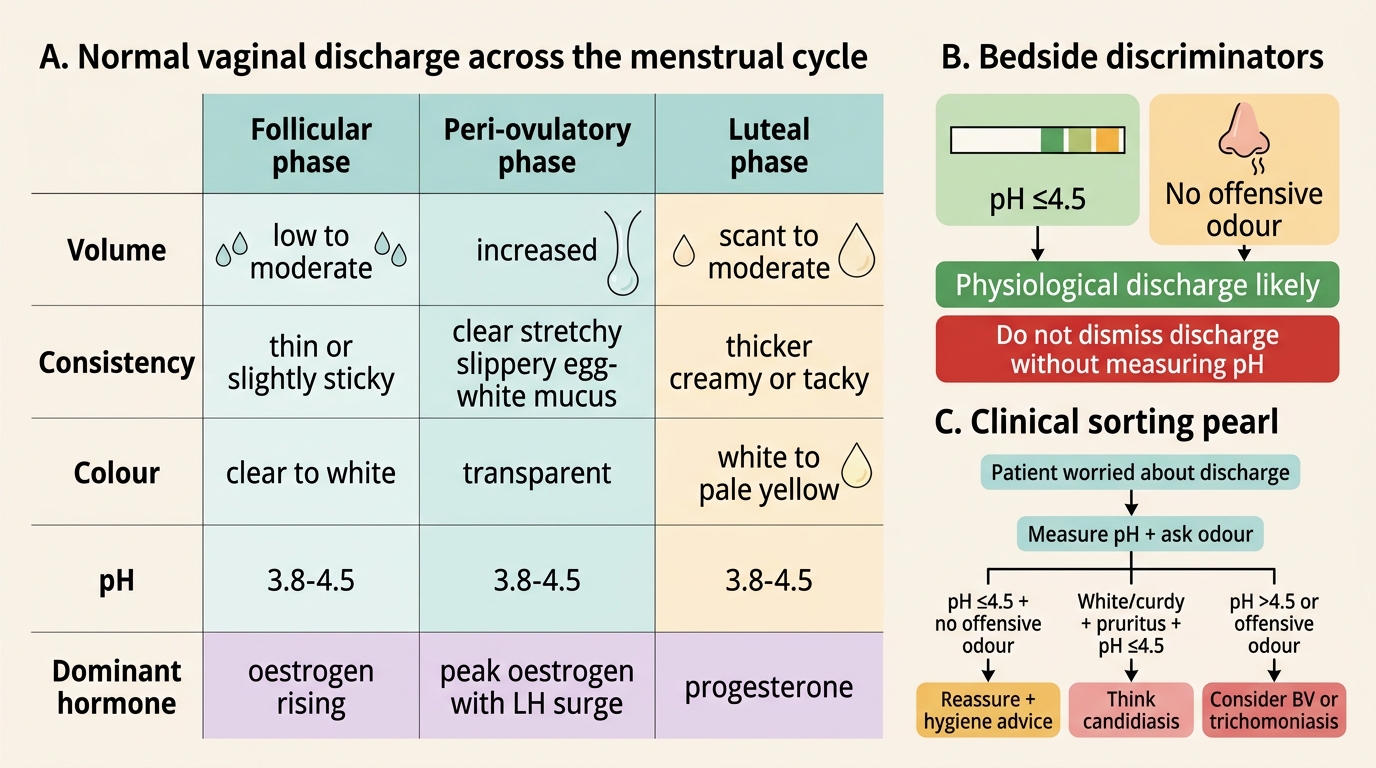
Normal Vaginal Discharge Across the Menstrual Cycle
CLINICAL PEARL
When a patient presents worried about vaginal discharge, the two most important bedside discriminators are pH and odour. A pH ≤4.5 and no offensive smell essentially excludes bacterial vaginosis and trichomoniasis — the two most common pathological causes. If the discharge is white/curdy with pruritus but pH is still ≤4.5, think candidiasis. If both pH and odour are normal, the discharge is almost certainly physiological and the patient needs reassurance and hygiene advice, not a swab panel. Conversely, never dismiss a complaint of 'just discharge' without measuring pH — a normal-looking discharge with elevated pH may be the early presentation of BV that has not yet become overtly symptomatic.