Page 12 of 22
OG24.1 | Abnormal Uterine Bleeding — SDL Guide (Part 2)
Management of AUB
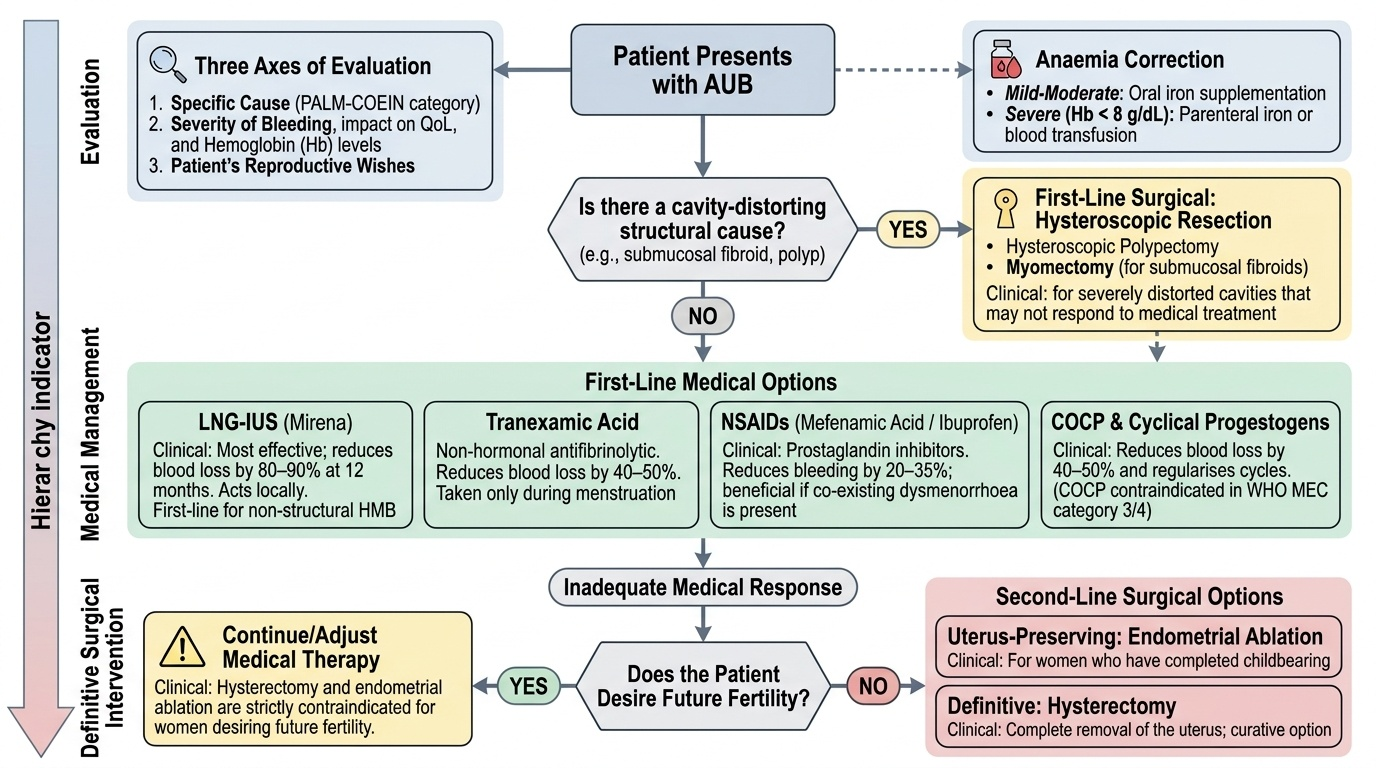
The management of AUB is guided by three axes: the specific cause (PALM-COEIN category), the severity of bleeding and its impact on quality of life and haemoglobin, and the patient's reproductive wishes. A woman who desires future fertility cannot undergo hysterectomy or endometrial ablation; a woman with a submucosal fibroid causing severe anaemia and distorted cavity may not respond to medical treatment and needs hysteroscopic resection. Management is therefore always individualised, but follows a clear evidence-based hierarchy: medical treatment before surgical intervention, and uterus-preserving options before definitive ablation or hysterectomy.
Before initiating any treatment, anaemia should be corrected — oral iron supplementation for mild-moderate anaemia; parenteral iron or blood transfusion for severe symptomatic anaemia (Hb <8 g/dL).
Medical Management — First-Line Options:
- Levonorgestrel-releasing intrauterine system (LNG-IUS, Mirena): The single most effective medical treatment for HMB — reduces blood loss by 80–90% at 12 months. Acts locally on the endometrium via high progestogen concentrations causing endometrial atrophy. First-line for HMB in women not seeking immediate fertility (WHO MEC category 1 for most women). Also treats adenomyosis effectively. NOT contraindicated by fibroids unless the cavity is significantly distorted.
- Tranexamic acid: An antifibrinolytic agent that inhibits plasminogen activator in the endometrium, reducing fibrinolysis and blood loss by ~40–50%. Non-hormonal, taken only during menstruation (500 mg–1 g three times daily during flow). Safe and effective for HMB; especially useful in women who cannot tolerate hormonal treatment or wish to preserve fertility without hormones. Does not affect cycle regularity.
- NSAIDs (e.g. mefenamic acid, ibuprofen): Prostaglandin synthesis inhibitors; reduce menstrual blood loss by ~20–35% and also reduce dysmenorrhoea. Taken during menstruation. Less effective than tranexamic acid or LNG-IUS for HMB, but beneficial when dysmenorrhoea coexists.
- Combined oral contraceptive pill (COCP): Reduces blood loss by ~40–50% and regularises cycles. Useful for AUB-O and as a second-line option when LNG-IUS is not accepted. Contraindicated by WHO MEC category 3/4 conditions (migraine with aura, smoking ≥35 yr, venous thromboembolism history).
- Cyclical oral progestogen: Norethisterone 5 mg three times daily, days 5–26 of the cycle. Less effective than LNG-IUS for HMB. Useful for anovulatory AUB-O (provides progesterone opposition to oestrogen). Also used short-term to stop acute heavy bleeding (norethisterone 5 mg three times daily for 10 days).
- GnRH analogues: Induce medical menopause — reserved for short-term use (≤6 months) to shrink fibroids preoperatively or to treat severe anaemia before surgery. Cannot be used long-term without add-back HRT (bone loss).
Cause-Specific Medical Treatment:
- AUB-O from hypothyroidism: thyroxine replacement restores ovulation and normalises cycles.
- AUB-O from hyperprolactinaemia: dopamine agonist (cabergoline) restores ovulation.
- AUB-C (von Willebrand disease): tranexamic acid + DDAVP (desmopressin, intranasal) during menstruation; specialist haematology review.
Surgical Management:
- Hysteroscopic polypectomy: Definitive treatment for AUB-P; outpatient or day-case procedure; specimen sent for histology.
- Hysteroscopic myomectomy: For submucosal fibroids (FIGO types 0–1; type 2 may require two-stage resection); fertility-preserving.
- Abdominal/laparoscopic myomectomy: For large intramural fibroids causing symptoms; fertility-preserving but significant recurrence rate (25–50% at 5 years).
- Uterine artery embolisation (UAE): Interventional radiology; effective for symptomatic fibroids; preserves uterus but may impair fertility (not first-line in women desiring pregnancy).
- Endometrial ablation: Destroys the endometrium to reduce or stop periods; suitable for completed family; contraindicated if endometrial pathology unexcluded. Second-generation techniques (thermal balloon, microwave, radiofrequency): 80–90% satisfaction rate; ~30% achieve amenorrhoea.
- Hysterectomy: Definitive curative treatment for HMB when all other options have failed or are declined; 100% satisfaction. Laparoscopic preferred over open for most indications. Must be preceded by exclusion of endometrial malignancy.
Provided image
CLINICAL PEARL
The LNG-IUS (Mirena) is the single most effective medical treatment for heavy menstrual bleeding, reducing blood loss by 80–90% — superior to all oral medical treatments including tranexamic acid and combined oral contraceptives. It is also highly effective in adenomyosis. The common misconception is that fibroids are a contraindication to LNG-IUS — in fact, fibroids are only a contraindication if they significantly distort the uterine cavity (preventing proper IUS placement), not merely if they are present. For a woman with a normal-shaped cavity, an LNG-IUS should be the first-line option offered before any surgical intervention.
Self-Assessment
The scenarios below test your ability to apply the PALM-COEIN classification, select appropriate investigations, and outline a management plan. For each scenario, start by determining the FIGO AUB category (you may assign more than one, since real patients frequently have concurrent structural and non-structural causes), then select the key investigation that would confirm your classification, and then propose a management hierarchy that respects the patient's reproductive wishes. At the final-year MBBS level, AUB questions frequently combine classification with management decision-making — demonstrating that you can apply the framework rather than merely recite the acronym is what distinguishes a high-scoring response from a rote one. Note that in scenarios involving postmenopausal bleeding or risk factors for endometrial carcinoma, the exclusion of malignancy must always be your first priority regardless of the volume of bleeding or other findings.
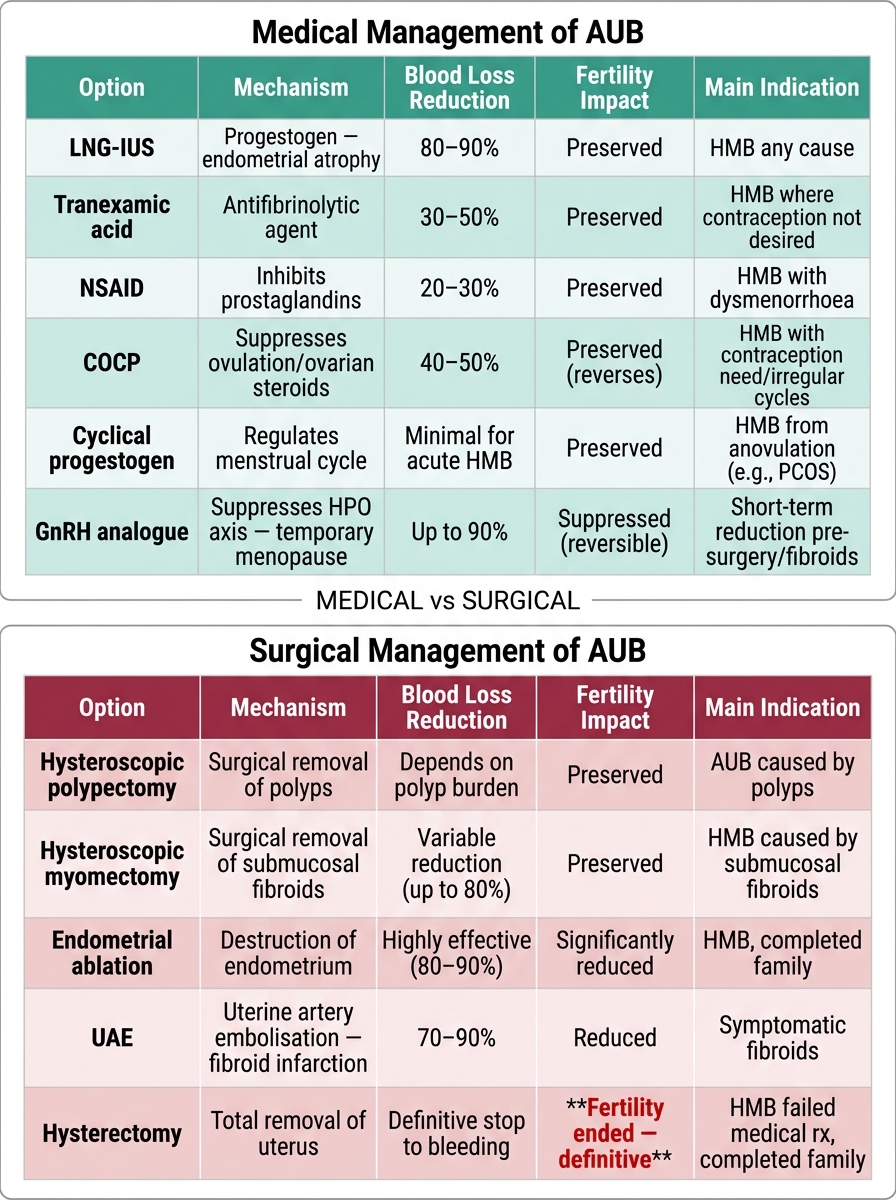
AUB Management Options: Medical vs Surgical — Mechanism, Efficacy, Fertility Impact
- A 42-year-old woman has heavy regular periods for 3 years. Ultrasound shows a 3 cm intramural fibroid and a 2 cm submucosal fibroid (type 1). Haemoglobin is 10.1 g/dL. She has one child and desires no more pregnancies. Classify and propose management.
- A 16-year-old has had heavy periods since menarche. She bleeds heavily enough to be transfused. There is no pelvic pathology on ultrasound. Her mother also had heavy periods. Coagulation screen shows a prolonged APTT. What FIGO category is this? What specific investigation confirms the diagnosis?
- A 50-year-old woman has irregular bleeding for 6 months. TSH is normal. Pelvic ultrasound shows endometrial thickness of 9 mm. She is obese (BMI 38) and nulliparous. What is your priority investigation and why?
- A 32-year-old with PCOS has irregular bleeding approximately every 3 months. Day-21 progesterone is 1.2 nmol/L. She wants to conceive. Classify and outline the immediate and fertility-focused management.
SELF-CHECK
A 35-year-old woman with FIGO AUB-L (type 1 submucosal fibroid) has completed her family and has failed tranexamic acid and LNG-IUS therapy. She has a haemoglobin of 8.5 g/dL. The most appropriate next management step is:
A. Endometrial ablation — she has completed her family
B. Hysteroscopic myomectomy — removes the submucosal fibroid and preserves the uterus for endometrial procedures
C. Immediate hysterectomy — all medical options have failed
D. GnRH analogue for 12 months to shrink the fibroid
Reveal Answer
Answer: B. Hysteroscopic myomectomy — removes the submucosal fibroid and preserves the uterus for endometrial procedures
Hysteroscopic myomectomy is the appropriate next step for a symptomatic submucosal fibroid (FIGO type 0–2) after failed medical therapy. It is a cavity-restoring, fertility-neutral, uterus-preserving procedure that directly removes the structural cause of bleeding. Endometrial ablation is not appropriate when an intracavitary fibroid is present — the fibroid must first be removed for ablation to be effective and safe. GnRH analogues are used for short-term preoperative fibroid shrinkage, not as long-term standalone therapy. Hysterectomy is a last resort when less invasive options have been tried.