Page 14 of 22
OG25.1 | Amenorrhea — SDL Guide
Learning Objectives
- Define primary and secondary amenorrhea with the correct age and duration thresholds
- Classify the causes of amenorrhea using a compartment-based framework (outflow/uterine, ovarian, pituitary, hypothalamic)
- Describe the clinical features and hormonal patterns that distinguish major causes within each compartment
- Outline a systematic investigation approach including β-hCG, TSH, prolactin, FSH/LH, progesterone challenge, karyotype, and pelvic ultrasound
- Discuss the principles of management tailored to each aetiology, including fertility implications and long-term considerations
INSTRUCTIONS
Amenorrhea — the absence of menstruation — is one of the most common and diagnostically rich presentations in gynaecological practice. Far from being a single diagnosis, it is a symptom whose cause can reside at any level of the hypothalamic-pituitary-ovarian-uterine axis. This module guides you through a structured compartment-based framework to localise the problem, interpret investigations logically, and apply cause-specific management. The skills you develop here — systematic hormonal thinking and pattern recognition — underpin your ability to counsel patients effectively on fertility, long-term bone health, and cardiovascular risk.
References
- DC Dutta's Textbook of Gynaecology, 8th ed., Ch. 24 — Amenorrhea (textbook)
- Shaw's Textbook of Gynaecology, 17th ed., Ch. 19 — Amenorrhea and Oligomenorrhea (textbook)
- Jeffcoate's Principles of Gynaecology, 8th ed., Ch. 22 (textbook)
- ESHRE Guideline: Management of women with premature ovarian insufficiency, 2016 (guideline)
- Endocrine Society Clinical Practice Guideline: Functional Hypothalamic Amenorrhea, 2017 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Priya is 17 years old when her mother brings her to the gynaecology outpatient department with a straightforward-sounding complaint: she has never had a period. On examination, Priya has normal breast development (Tanner stage IV), pubic and axillary hair are present, and she is of normal height and build. A vaginal examination reveals a blind vaginal pouch. Pelvic ultrasound shows no uterus, but two ovaries are present. Her serum FSH is 6 IU/L, LH 5 IU/L — both normal. What is happening? Why does she have normal secondary sexual development yet no uterus and no menses? Now consider a contrasting case: Meena, 28 years old, had regular cycles until 14 months ago when they stopped abruptly after a difficult curettage for an incomplete miscarriage. A progesterone challenge produces no withdrawal bleed. Her FSH is 7 IU/L and prolactin is normal. The same symptom — absent menses — but the anatomical level of the problem is entirely different. Understanding amenorrhea means learning to ask the right questions, read the hormonal signals, and localise the cause before you treat.
WHY THIS MATTERS
Amenorrhea reaches every branch of medicine — a gynaecologist encounters it as an endocrine puzzle, an internist as a marker of systemic disease, a paediatrician as an indicator of pubertal failure, and a psychiatrist as a consequence of anorexia. In the Indian context, the presentation is additionally shaped by delayed health-seeking, nutritional stress, tuberculosis (a leading cause of Asherman syndrome), and thyroid disease — all of which must be actively considered in the differential. For the NMC competency OG25.1, you are expected to describe and discuss causes, investigations, and principles of management at the KH (Knowledge and Understanding applied to clinical scenarios) level — meaning you must not only know the facts but be able to apply them to a patient encounter, as in the two cases above.
RECALL
Before proceeding, activate your prior knowledge. The hypothalamic-pituitary-ovarian (HPO) axis operates as a feedback loop: the hypothalamus releases gonadotrophin-releasing hormone (GnRH) in pulses, which drives the anterior pituitary to secrete follicle-stimulating hormone (FSH) and luteinising hormone (LH). FSH recruits ovarian follicles; the dominant follicle produces oestradiol, which exerts positive feedback at mid-cycle to trigger the LH surge and ovulation. After ovulation, the corpus luteum produces progesterone, which prepares the endometrium. If conception does not occur, progesterone falls, the endometrium sheds, and menstruation occurs. Disruption at ANY level — hypothalamus, pituitary, ovary, or outflow tract — can silence this cascade. Also recall from your study of puberty: the first period (menarche) requires an intact HPO axis, adequate body fat, functional ovaries, a uterus, and a patent outflow tract. Any absence of these can manifest as primary amenorrhea. Secondary amenorrhea means the system was once working and has subsequently been switched off or obstructed.
Clinical Presentation and Classification of Amenorrhea
Amenorrhea is defined not merely as the absence of menstruation, but with specific age- and duration-based thresholds that reflect clinically actionable cut-points. Understanding which definition applies is the first step in the clinical encounter.
Primary amenorrhea is the condition in which menstruation has never occurred. The two accepted thresholds are: no menarche by the age of 15 years when secondary sexual characteristics (thelarche, pubarche) are present, and no menarche by the age of 13 years when there are no secondary sexual characteristics whatsoever. The logic behind the lower threshold is that the absence of secondary sexual characteristics at 13 suggests a more fundamental failure of puberty — likely at the ovarian or hypothalamic-pituitary level — and warrants earlier evaluation. Using the higher cut-off when secondary sexual characteristics are present acknowledges that most adolescents with breast development who have not yet menstruated by 15 will have a structural anomaly of the outflow tract rather than a failure of hormonal activation.
Secondary amenorrhea is defined as the cessation of previously established menses. The conventional duration thresholds are: absence of ≥3 months in a woman who previously had regular monthly cycles, or ≥6 months in a woman who previously had irregular cycles. The rationale for the longer threshold in irregular-cycle patients is that occasional gaps are expected in anovulatory states such as polycystic ovary syndrome (PCOS), and labelling a 3-month gap as secondary amenorrhea would over-medicalise normal variation. Pregnancy must always be excluded before either category of amenorrhea is further investigated — a serum β-hCG is the mandatory first step.
The clinical evaluation begins with a careful history: when did periods start (if ever), how regular were they, was there a precipitating event (weight change, intense exercise, stress, uterine procedure, postpartum haemorrhage, systemic illness), are there symptoms of hypoestrogenism (hot flushes, vaginal dryness, dyspareunia), galactorrhoea (suggests hyperprolactinaemia), or hirsutism and acne (suggests androgen excess). The presence or absence of secondary sexual characteristics on examination directs the initial compartment hypothesis. A normal height and normal sexual development in primary amenorrhea suggests an intact hormonal axis with a structural outflow or uterine problem, while short stature with absent sexual development points strongly toward a chromosomal or gonadal cause.
Compartment-Based Causes of Amenorrhea in the HPO Axis
Physiological Basis and Compartment-Based Aetiology
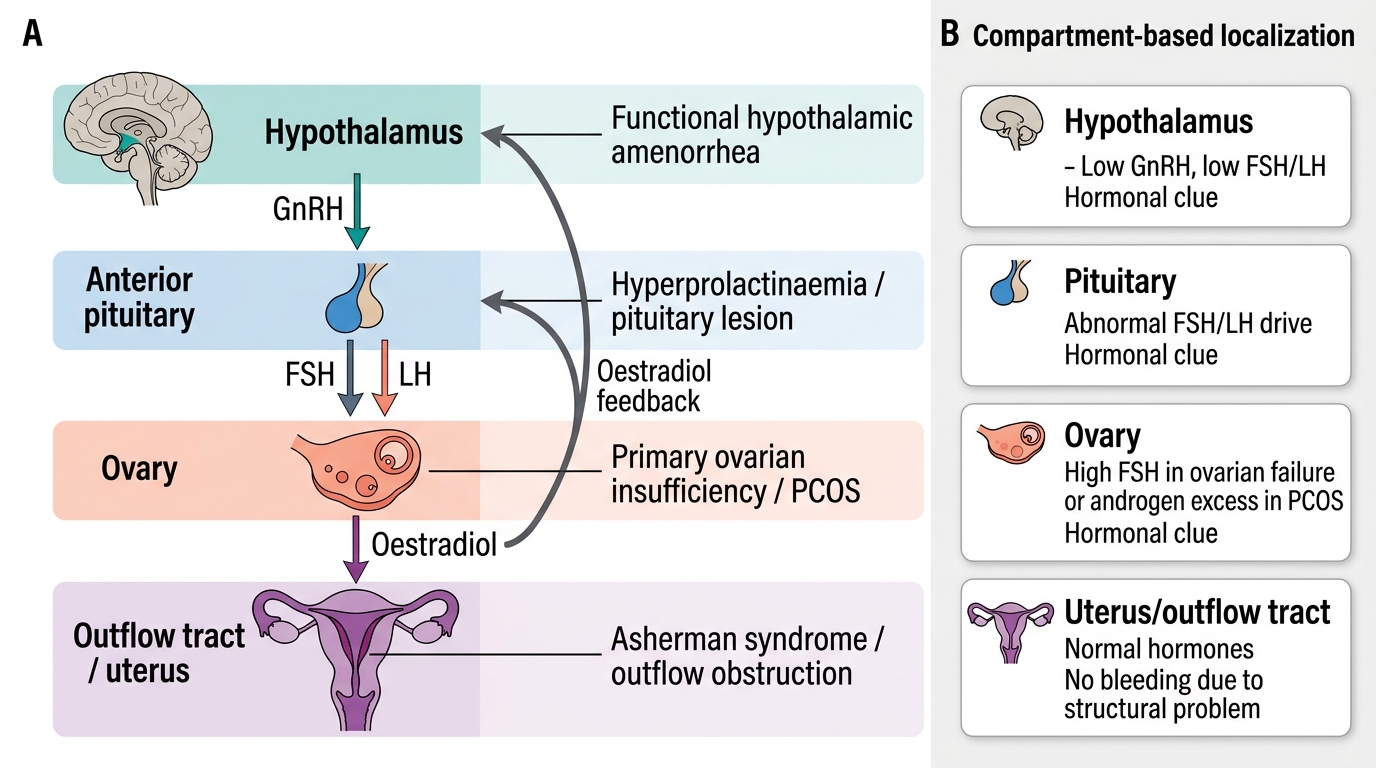
The most powerful organising principle for amenorrhea is the compartment-based aetiology framework, which asks: at which level of the reproductive axis has the menstrual process been disrupted? There are four compartments, each with a distinct hormonal signature that allows you to localise the problem with targeted blood tests before any definitive imaging. The value of this framework lies in its parsimony: rather than memorising an undifferentiated list of 20-plus diagnoses, you learn four hormonal archetypes and then populate each with its specific conditions. This approach transforms the investigation of amenorrhea from a scatter-gun hormone panel into a directed, logical sequence that conserves resources and minimises patient anxiety.
The four compartments correspond to the four anatomical levels where the menstrual process can be disrupted: (1) the hypothalamus, which generates the GnRH pulse; (2) the anterior pituitary, which converts that pulse into FSH and LH; (3) the ovary, which responds to FSH and LH by developing a follicle and producing oestradiol; and (4) the outflow tract and uterus, which responds to ovarian hormones by growing and shedding the endometrium. Because each level depends on the one above it, a lesion at any level creates a characteristic upstream-downstream hormonal pattern. Specifically: a failure at the ovary will deprive the pituitary of negative feedback, causing FSH and LH to rise — creating the hypergonadotrophic pattern. A failure at the hypothalamus or pituitary will deprive the ovary of its stimulatory signal, causing FSH and LH to fall — the hypogonadotrophic pattern. And a failure at the uterus or outflow tract does not alter the hormonal axis at all — the hormones are entirely normal, but the end-organ cannot respond or the menstrual flow cannot exit.
The four compartments and their characteristic hormonal patterns:
| Compartment | Key Causes | FSH | LH | Oestradiol | Prolactin |
|---|---|---|---|---|---|
| Hypothalamic | FHA, craniopharyngioma, Kallmann | Low | Low | Low | Normal/low |
| Pituitary | Prolactinoma, Sheehan, empty sella | Low/normal | Low/normal | Low | Elevated (prolactinoma) |
| Ovarian | Turner, POI, PCOS | Elevated (POI/Turner) / Normal (PCOS) | Elevated / Elevated LH (PCOS) | Low (POI/Turner) / Variable (PCOS) | Normal |
| Outflow/Uterine | MRKH, Asherman, imperforate hymen | Normal | Normal | Normal | Normal |
The key insight is that if the ovaries have failed (compartment III), the pituitary loses inhibitory feedback from oestradiol and drives FSH and LH upward — this is called hypergonadotrophic hypogonadism. If the problem is above the ovary (hypothalamus or pituitary), the signal to the ovary is absent and FSH/LH are inappropriately low — hypogonadotrophic hypogonadism. If the ovaries are functioning normally but the uterus or outflow is obstructed, the hormonal axis is intact and FSH/LH/oestradiol are all normal — the classic normogonadotrophic pattern. PCOS represents a distinct normogonadotrophic picture with anovulation and hyperandrogenism. This hormonal classification allows you to direct the investigation toward the correct compartment before committing to expensive imaging.
Outflow Tract and Uterine Causes
Outflow tract and uterine causes produce primary or secondary amenorrhea in the presence of a hormonally normal axis. Because the ovaries are intact and producing oestradiol, the patient has normal secondary sexual development — the hallmark of this compartment.
Müllerian agenesis (MRKH syndrome — Mayer-Rokitansky-Küster-Hauser) is the commonest structural cause of primary amenorrhea, accounting for approximately 15% of cases. The karyotype is 46XX (a normal female genotype), the ovaries are present and functional, and secondary sexual characteristics are completely normal. The defect is developmental failure of the Müllerian (paramesonephric) ducts, resulting in absence of the uterus and the upper two-thirds of the vagina. On examination, there is a short blind vaginal pouch. The FSH, LH, and oestradiol are all normal. MRKH must be distinguished from complete androgen insensitivity syndrome (CAIS), which also presents with primary amenorrhea, absent uterus, and normal female external genitalia — but the karyotype is 46XY, and serum testosterone is in the male range (because the patient has undescended testes producing testosterone that cannot be utilised at androgen receptors). Karyotype testing is therefore mandatory in every patient with primary amenorrhea and absent uterus.
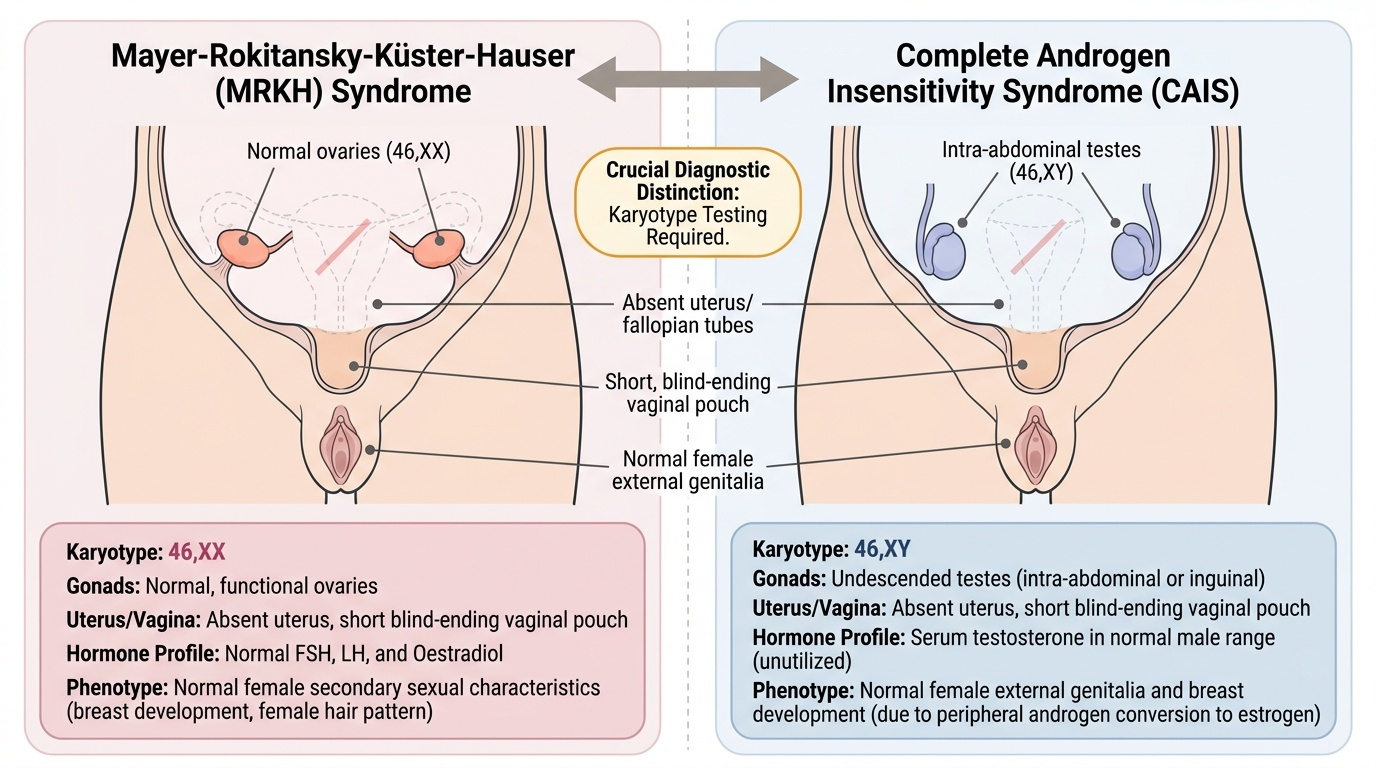
Provided image
Asherman syndrome (intrauterine adhesions, synechiae) is the commonest cause of secondary amenorrhea in the uterine compartment. It results from destruction of the basal endometrial layer, most often after dilatation and curettage (D&C) — particularly post-pregnancy curettage (for incomplete abortion, missed abortion, or postpartum retained products) where the decidualised endometrium is especially vulnerable. In India, endometrial tuberculosis is an important additional cause. The hallmark finding is that the progesterone challenge test produces no withdrawal bleed, because even if oestrogen primes the endometrium, adhesions prevent it from shedding normally. Hysteroscopy is both diagnostic (directly visualises adhesions) and the definitive treatment modality.
Other outflow tract causes include imperforate hymen (typically presents at menarche with cyclical lower abdominal pain, haematocolpos, bulging membrane at the introitus — classified as obstructive primary amenorrhea with cyclic pain rather than true hormonal amenorrhea), transverse vaginal septum, and cervical stenosis (post-cone biopsy or post-D&C).
SELF-CHECK
A 17-year-old presents with primary amenorrhea and normal secondary sexual characteristics. Pelvic ultrasound shows absent uterus. Her serum FSH, LH, and oestradiol are all within normal limits. Which investigation would BEST distinguish MRKH syndrome from complete androgen insensitivity syndrome (CAIS)?
A. Serum oestradiol level
B. Serum FSH level
C. Karyotype analysis
D. Pelvic MRI for uterine morphology
Reveal Answer
Answer: C. Karyotype analysis
Both MRKH and CAIS present with primary amenorrhea, absent uterus, and a normal hormonal profile (FSH, LH, oestradiol are all normal in both). The crucial distinction is chromosomal: MRKH is 46XX (normal female karyotype) while CAIS is 46XY. Serum testosterone can also help (male-range in CAIS), but karyotype is the definitive diagnostic test. Pelvic MRI confirms uterine absence but cannot differentiate the two conditions. FSH and oestradiol will be normal in both — they do not help in this scenario.