Page 6 of 22
OG23.2 | Delayed Puberty — SDL Guide (Part 2)
Management of Common Causes of Delayed Puberty
Management of delayed puberty is entirely cause-specific. The three categories require fundamentally different approaches: expectant management for CDGP, hormone replacement for gonadal failure, targeted therapy for functional suppression, and surgical correction for outflow obstruction. A clear diagnosis must precede any treatment, and the patient and family must be counselled on the diagnosis, its implications (especially for fertility and long-term health), and the treatment plan.
Constitutional Delay of Growth and Puberty (CDGP):
Reassurance and watchful waiting is the first-line approach because spontaneous puberty will occur — the only question is timing. Explain to the family that the bone age is consistent with the pubertal stage, that adult height and fertility will be normal, and that this is a variant of normal rather than a disease. If psychosocial impact is significant (peer comparison, depression, school avoidance), a short course of low-dose ethinyl oestradiol (2–5 μg/day orally for 6 months) can be offered to 'prime' puberty — this accelerates the appearance of secondary sex characteristics without significantly advancing bone age or compromising final height. Review every 6 months; most girls will show spontaneous pubertal progression within 1–2 years.
Turner Syndrome:
Requires lifelong multidisciplinary management. (a) Oestrogen replacement: Start low-dose oestrogen at age 12–13 (bone age ~10–11) to mimic the gradual rise of normal puberty — too early risks premature epiphyseal fusion; too late risks osteoporosis. Begin with low-dose oestradiol patches (transdermal preferred — avoids hepatic first-pass effect on clotting factors) or oral oestradiol, increasing slowly over 2–3 years. Add cyclical progestogen once breakthrough bleeding occurs or after 2 years of unopposed oestrogen to establish a withdrawal bleed and protect the endometrium. (b) Growth hormone: Commenced in childhood (before pubertal induction) to maximise adult height — typically 0.35 mg/kg/week SC; can add 5–10 cm to final height. (c) Cardiac surveillance: Echocardiogram/cardiac MRI — bicuspid aortic valve and aortic root dilation require monitoring; aortic root >4 cm is a contraindication to pregnancy. (d) Fertility: Virtually all Turner patients are infertile due to streak ovaries. Egg donation IVF is the primary fertility option. Rare mosaics with residual follicles may conceive spontaneously. (e) Annual surveillance: Thyroid (autoimmune thyroiditis common), blood pressure, hearing, liver function, renal imaging.
Kallmann Syndrome:
Fertility requires specialist treatment. For puberty induction: sequential low-dose oestrogen as for Turner, to develop secondary sex characteristics. For fertility: pulsatile GnRH therapy (GnRH pump — gold standard, mimics physiological pulsatility) or gonadotrophin injections (FSH + LH/hCG to stimulate ovarian development). Long-term sex hormone replacement required between fertility treatments.
Functional Hypothalamic Suppression (anorexia, female athlete triad):
Address the underlying cause: nutritional rehabilitation in anorexia (target BMI >18.5); reduced exercise load in athletes; treatment of chronic illness. FSH/LH and oestradiol normalise with weight restoration — this may take 3–6 months. If recovery is prolonged, transient oestrogen supplementation protects bone density. Multidisciplinary care (dietitian, psychiatrist, endocrinologist) is required for anorexia nervosa.
Imperforate Hymen:
Surgical hymenectomy under anaesthesia — drain the haematocolpos and create a permanent opening. Outcome is excellent with no long-term reproductive sequelae if treated before secondary damage from backflow (haematometra, haematosalpinx).
MRKH Syndrome:
No uterus — pregnancy is impossible except via gestational surrogacy. Vaginal dilators (Frank's progressive dilation technique) are the first-line approach to create a functional vagina (80–90% success). Surgical creation of a neovagina (McIndoe procedure — split-thickness skin graft over a mould) is reserved for those failing dilators. Ovaries are normal — her own eggs can be used with a surrogate if fertility is desired.
Complete AIS:
Gonadectomy is recommended, but the timing is debated. Current practice generally favours deferring until after puberty (the testes produce aromatisable androgens that oestrogen is derived from — removing them pre-puberty blunts breast development and requires immediate HRT). Post-gonadectomy: lifelong oestrogen replacement. Vaginal dilators for vaginal lengthening. Karyotype disclosure: psychological support essential — many patients are unaware of their 46,XY status.
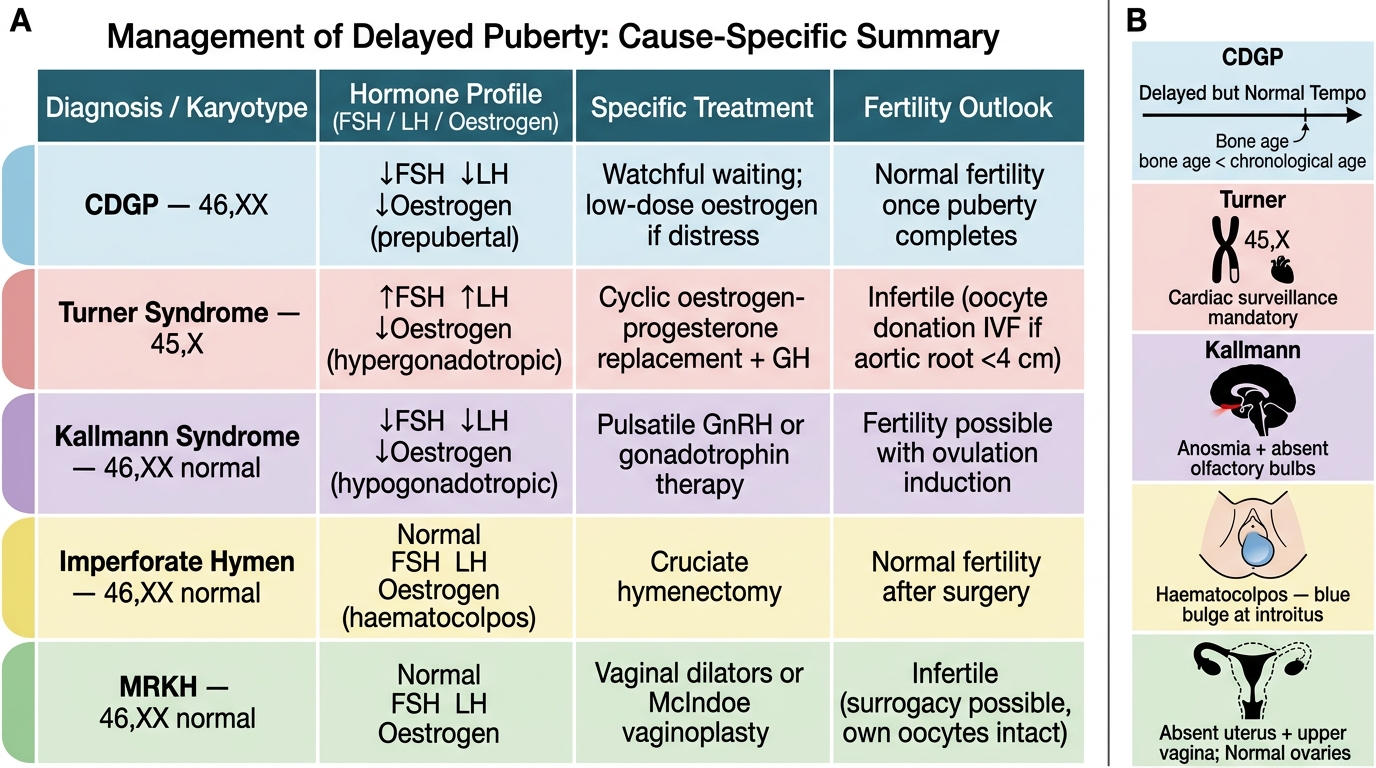
Delayed Puberty: Cause-Specific Management and Fertility Outcomes
CLINICAL PEARL
In Turner syndrome, always order a cardiac MRI in addition to echocardiography — echo misses aortic arch anomalies (coarctation, bicuspid aortic valve, aortic root dilation) in up to 20% of cases because the arch is behind the sternum. Aortic dissection is the leading cause of premature death in Turner syndrome, and the risk is dramatically increased in pregnancy (oestrogen-driven aortic wall changes). This means that before advising a Turner patient about egg donation IVF, you must obtain cardiac imaging and confirm that the aortic root diameter is below 4 cm — an aortic root >4 cm is a relative contraindication to pregnancy.
Self-Assessment
The scenarios below are designed to test your ability to apply the classification framework to clinical cases at the level expected in a final-year MBBS viva voce and written short-answer examination. Delayed puberty questions in assessments almost always require you to demonstrate three things: (1) systematic classification using the FSH/LH framework, (2) a logical investigation sequence that flows from the classification, and (3) cause-specific management principles. Practising active recall on these cases — attempting each from memory before consulting the text — consolidates the classification framework far more effectively than passive re-reading alone. For scenario-based questions, make it a habit to explicitly state your category first, then justify your investigation choice from that classification, and then outline the management plan specific to that category.
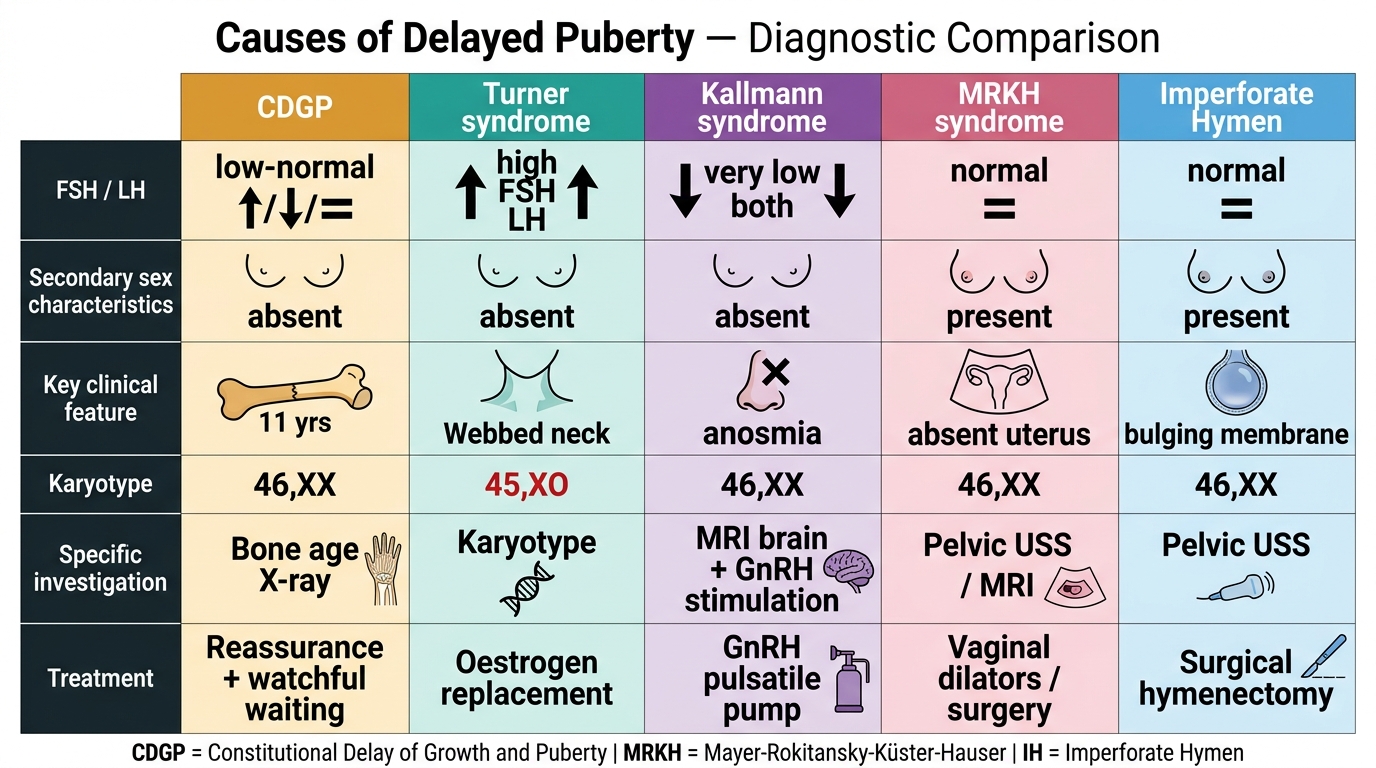
Delayed Puberty: Diagnostic Comparison of Five Key Causes
- A 15-year-old girl has no breast development. FSH is 58 IU/L. She has no webbed neck, but her height is 142 cm. What category is this? What is the single most important next investigation?
- A 16-year-old has normal breasts and pubic hair but no periods. FSH and LH are normal. Ultrasound shows no uterus. She has sparse axillary hair. What two diagnoses must be considered and what investigation distinguishes them?
- A 14-year-old has no puberty and no sense of smell. FSH and LH are both very low. Brain MRI is normal. What is the likely diagnosis and what does she need for fertility?
- Outline how you would explain CDGP to a concerned parent of a 14-year-old girl with delayed puberty and a bone age of 11 years.
SELF-CHECK
A 13-year-old girl presents with cyclical lower abdominal pain monthly for 6 months but no menstrual bleeding. Examination reveals a tense, bluish, bulging membrane at the introitus. Pelvic ultrasound shows a cystic midline mass. FSH and LH are normal. The management is:
A. Oestrogen replacement therapy to induce puberty
B. Surgical hymenectomy under anaesthesia
C. GnRH pulsatile pump therapy
D. Watchful waiting — periods will begin spontaneously
Reveal Answer
Answer: B. Surgical hymenectomy under anaesthesia
This is classic imperforate hymen presenting with haematocolpos. Normal FSH/LH confirms eugonadism (ovaries functional, HPO axis intact). The bluish bulging hymen is pathognomonic. Treatment is surgical hymenectomy — urgent if haematocolpos is large or there are signs of secondary complications (haematometra, haematosalpinx). Oestrogen replacement is not indicated as oestrogen production is normal.