Page 3 of 22
OG23.1 | Normal and Abnormal Puberty — SDL Guide (Part 3)
Self-Assessment
The questions below are designed to test your active recall and application of the key concepts covered in this module. Rather than simply re-reading the text, attempt each question from memory first — this retrieval practice is one of the most evidence-based strategies for consolidating clinical knowledge. For each question, consider not just the answer but the clinical reasoning chain that connects the physiology to the management decision. If a question exposes a gap, return to the relevant section and then attempt an answer in your own words before reviewing the model answer.
These questions are pitched at the level of a final-year MBBS viva voce or written short answer — the same level at which this competency (OG23.1) will be assessed. Pay particular attention to the ability to classify causes systematically and to outline a structured investigation approach, as these are the skills most commonly tested at this level.
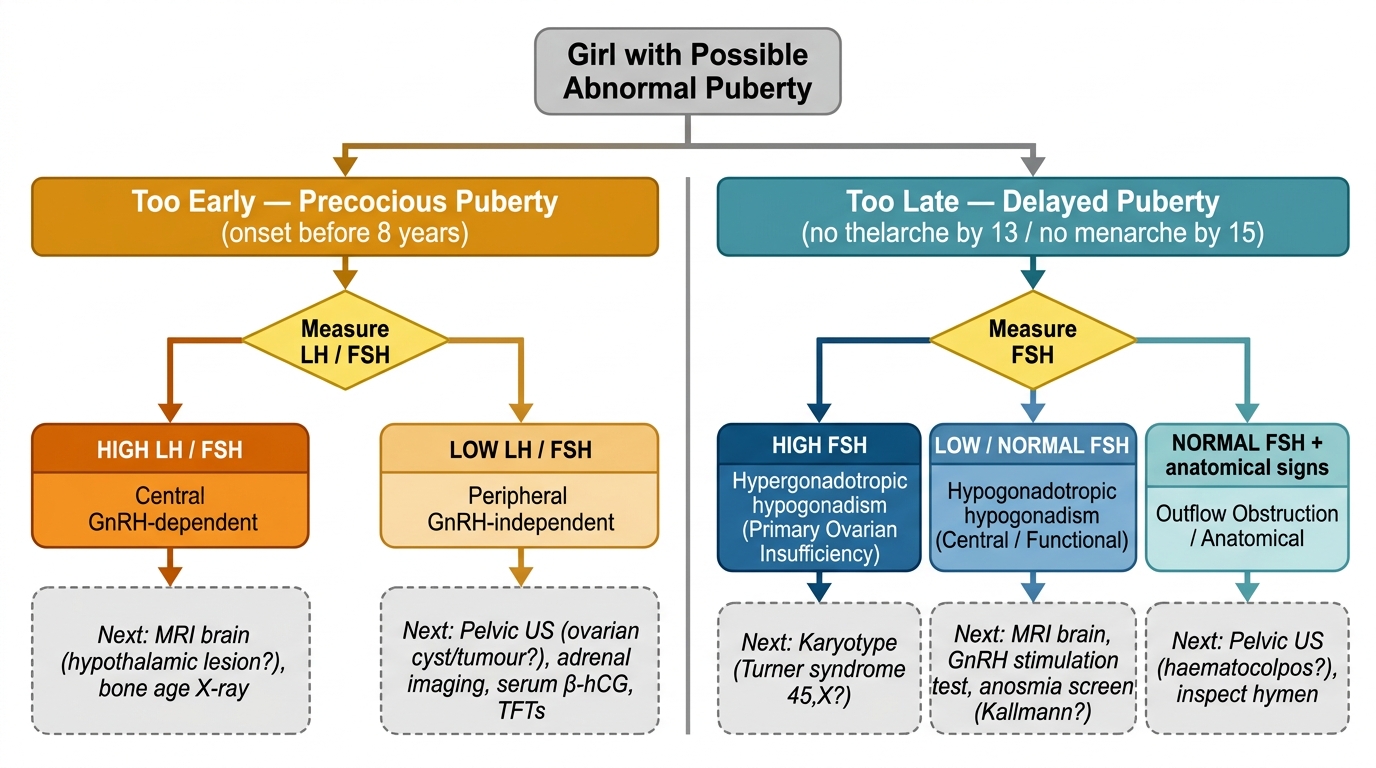
Diagnostic Algorithm for Abnormal Puberty in Girls
- Draw or describe the HPO axis as it operates during puberty: identify the hypothalamic pulse generator, the pituitary hormones released, the ovarian response, and the feedback loops.
- Tanner staging: For a girl at Tanner B4/PH3, describe the expected breast and pubic hair findings and state whether menarche has likely occurred yet.
- Classify delayed puberty in a 15-year-old with no menarche but normal breast development (B4): what anatomical category of primary amenorrhoea does she fall in? What initial investigation would you order first?
- Differentiate: A 7-year-old girl with isolated breast budding (B2) and a 7-year-old with B2 + PH2 + bone age 10 yr + accelerated growth. How do your management approaches differ?
SELF-CHECK
A 15-year-old girl has normal breast and pubic hair development (Tanner B4/PH4) but has never had a period. She has cyclical lower abdominal pain monthly. Pelvic ultrasound shows a midline cystic mass (haematocolpos). The most likely diagnosis and management is:
A. Turner syndrome — karyotype and oestrogen replacement
B. MRKH syndrome — surgical creation of neovagina
C. Imperforate hymen — hymenectomy to drain haematocolpos
D. Kallmann syndrome — GnRH pump therapy
Reveal Answer
Answer: C. Imperforate hymen — hymenectomy to drain haematocolpos
Normal secondary sex characteristics (normal oestrogen) + cyclical pain + haematocolpos = outflow tract obstruction. Imperforate hymen is the most common cause, presenting with a bluish bulging hymen at the introitus and haematocolpos on ultrasound. Treatment is surgical hymenectomy. This is eugonadism with outflow obstruction — FSH/LH are normal, which distinguishes it from Turner syndrome or Kallmann syndrome.