Page 12 of 18
OG27.3 | Pelvic Inflammatory Disease — SDL Guide (Part 2)
Management — Antibiotic Regimens and Criteria for Admission
Management of PID is fundamentally about starting the right antibiotic combination early enough to prevent irreversible tubal damage. Every hour of untreated salpingitis is an hour during which the inflammatory process is destroying the delicate mucosal folds of the tube that are essential for ovum transport and fertilisation. The treatment framework therefore has two parallel decision points: first, the choice between outpatient oral and inpatient intravenous therapy — based on clinical severity, ability to tolerate oral medications, complication status (TOA), and ability to comply with and return for follow-up; and second, the selection of the antibiotic regimen itself, which must cover the full polymicrobial spectrum of PID. Because PID is caused by a combination of STI pathogens (N. gonorrhoeae and C. trachomatis) and endogenous anaerobes, no single antibiotic agent provides adequate coverage — combination regimens using drugs from different classes are mandatory. Monotherapy with any single agent, however broad-spectrum, is clinically inadequate for PID. The three-drug outpatient regimen (ceftriaxone + doxycycline + metronidazole) reflects this polymicrobial reality.
Criteria for hospital admission (inpatient treatment):
- Surgical emergency not excluded (rule out ectopic pregnancy, appendicitis)
- Tubo-ovarian abscess (TOA) — requires IV antibiotics; does not respond to oral therapy alone
- Pregnancy
- Failure of oral outpatient therapy (no improvement at 72 hours)
- Severe illness with nausea and vomiting precluding oral medications
- Unable to follow up outpatient regimen or ensure compliance
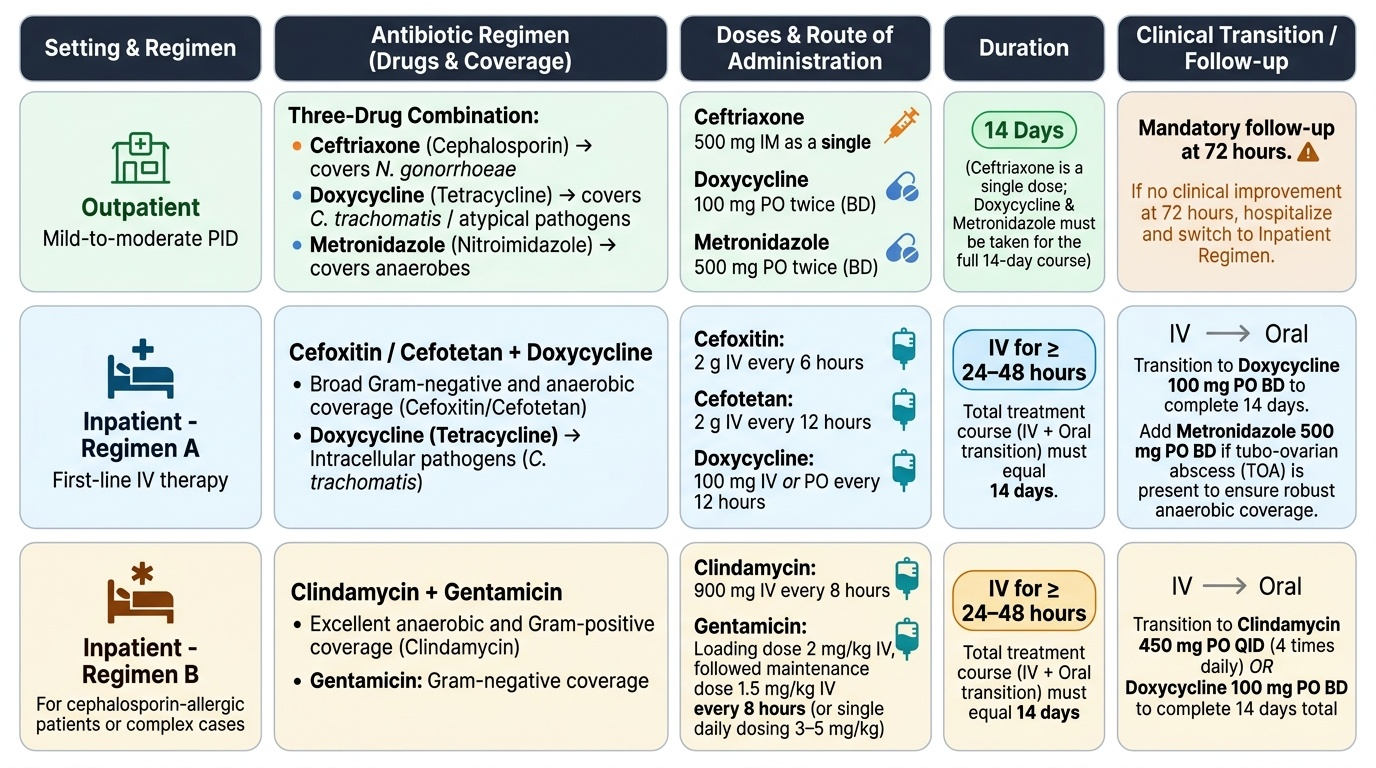
Outpatient regimen (CDC 2021):
Ceftriaxone 500 mg IM single dose PLUS doxycycline 100 mg oral BD × 14 days PLUS metronidazole 500 mg oral BD × 14 days.
- Ceftriaxone: covers N. gonorrhoeae (including reduced-sensitivity strains)
- Doxycycline: covers C. trachomatis and other intracellular organisms
- Metronidazole: covers anaerobes — added in the 2021 CDC update based on evidence that anaerobic coverage improves outcomes
- Duration: 14 days — adequate to treat chlamydial and anaerobic components
- Follow-up at 72 hours to confirm response
Inpatient regimen A (CDC 2021):
Cefoxitin 2 g IV every 6 hours (or cefotetan 2 g IV every 12 hours) PLUS doxycycline 100 mg IV or oral every 12 hours.
- Transition to oral doxycycline 100 mg BD + metronidazole 500 mg BD to complete 14 days total after clinical improvement.
Inpatient regimen B (CDC 2021 alternative):
Clindamycin 900 mg IV every 8 hours PLUS gentamicin loading dose 2 mg/kg IV, then maintenance 1.5 mg/kg IV every 8 hours (or once-daily gentamicin).
- Transition to oral clindamycin 450 mg every 6 hours or doxycycline 100 mg BD to complete 14 days.
Provided image
Tubo-ovarian abscess (TOA) management:
Most TOAs respond to inpatient IV antibiotics (Regimen B with clindamycin + gentamicin has better anaerobic coverage for TOA). Response is monitored clinically (fever resolution, pain improvement, WBC trending down) and with serial ultrasound. Surgical intervention is indicated if:
- No clinical improvement after 72 hours of IV antibiotics
- Abscess increases in size despite treatment
- Abscess ruptures (surgical emergency — immediate laparotomy/laparoscopy for drainage)
Surgical approach: drainage (percutaneous ultrasound-guided or laparoscopic) is preferred over salpingo-oophorectomy in women wishing to preserve fertility; definitive surgery in non-responsive cases.
Partner treatment and prevention of recurrence:
All sexual partners of women diagnosed with PID within the preceding 60 days should be tested and treated empirically for gonorrhoea and chlamydia — irrespective of their symptoms. Failure to treat the partner guarantees re-infection. Condom promotion at every clinical encounter. An IUD inserted within 3 weeks is a risk factor — if inserted recently and PID develops, removal is recommended (though re-insertion can be considered after treatment).
SELF-CHECK
A 26-year-old woman is admitted with severe PID. Transvaginal ultrasound reveals a 6 cm right adnexal complex mass with internal echoes consistent with a tubo-ovarian abscess. She is started on IV clindamycin + gentamicin. After 72 hours she remains febrile (38.6°C) and the mass is unchanged on repeat ultrasound. What is the next step?
A. Continue same IV antibiotic regimen for a further 5 days before reassessing
B. Switch to oral antibiotics and discharge with outpatient follow-up
C. Surgical drainage of the abscess — laparoscopic or ultrasound-guided percutaneous
D. Add oral metronidazole to the current IV regimen and reassess at 5 days
Reveal Answer
Answer: C. Surgical drainage of the abscess — laparoscopic or ultrasound-guided percutaneous
Failure to improve clinically (persistent fever, unchanged abscess size) after 72 hours of adequate IV antibiotic therapy is the criterion for surgical intervention in TOA. Continuing the same antibiotics without drainage is unlikely to be effective when the abscess has not responded within 72 hours. Switching to oral antibiotics would be inappropriate when the patient remains febrile with an unchanged abscess. Surgical drainage — laparoscopic (preferred to preserve fertility) or ultrasound-guided percutaneous — is now indicated.
Long-Term Implications and Prevention
The long-term consequences of PID are serious, cumulative with each episode, and largely preventable — which means that every clinical encounter with PID is an opportunity not only to treat the current episode but to change the patient's reproductive trajectory. A clinician who treats one episode of PID promptly with the correct regimen, ensures the partner is treated, and equips the patient with the knowledge to prevent recurrence may protect her from years of infertility, the anxiety of ectopic pregnancy, and the disability of chronic pelvic pain. Conversely, a missed or undertreated episode, an untreated partner, or a regimen without anaerobic coverage silently adds another layer of tubal scarring and compounds the long-term risk. The data on cumulative risk are unambiguous and must inform every clinical decision about the urgency and adequacy of PID management. These consequences also explain why PID prevention — through STI control, early diagnosis, and condom promotion — is a cost-effective public health intervention: every case of PID prevented avoids the far greater cost of infertility investigation and treatment.
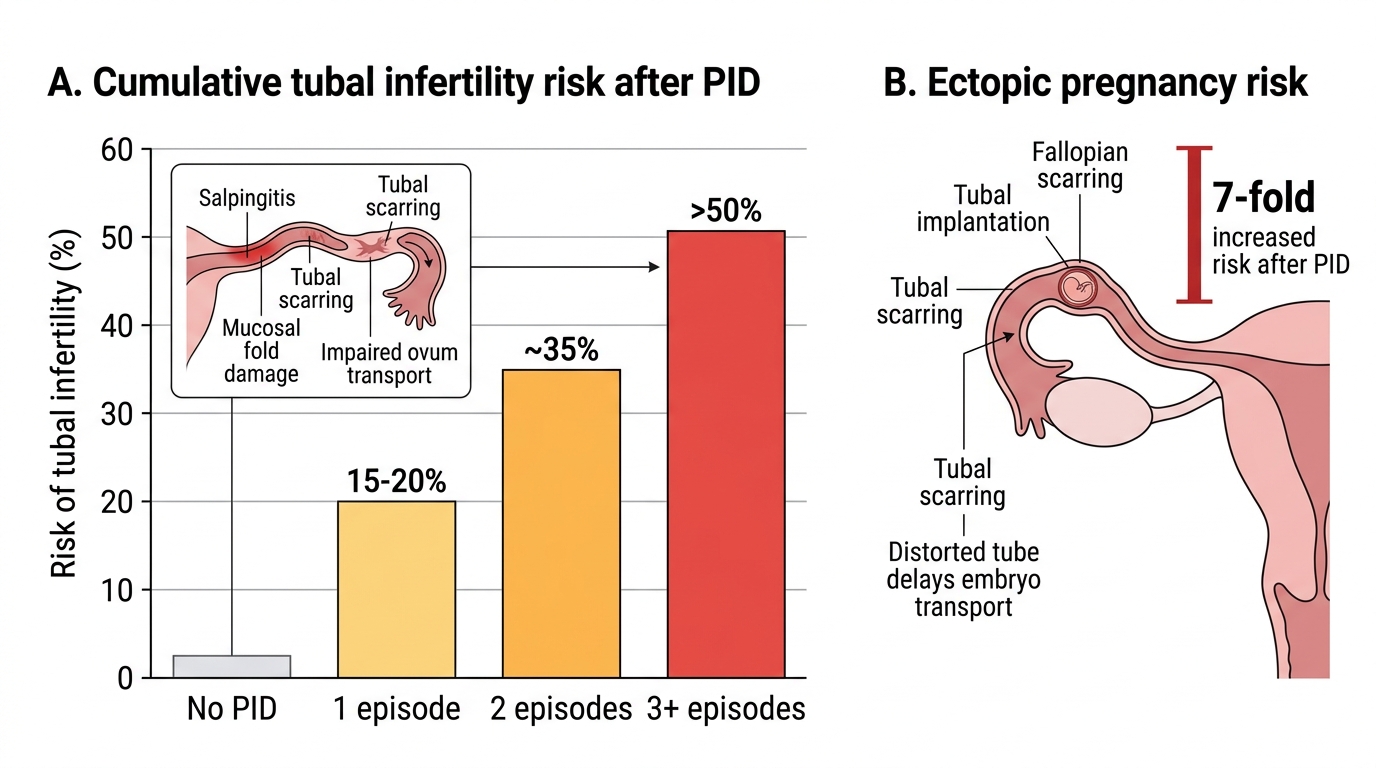
Tubal infertility — the most devastating consequence:
Each episode of salpingitis destroys a portion of the tubal mucosal folds (plicae), replacing functional epithelium with scar tissue. The cumulative data are stark:
- After one episode of PID: 15–20% risk of tubal-factor infertility
- After two episodes: approximately 35% risk
- After three or more episodes: >50% risk of infertility
Mild, subclinical PID (which goes undiagnosed and untreated) carries the same infertility risk as symptomatic disease — because the tubal damage is identical at the microscopic level.
Ectopic pregnancy:
Tubal scarring from PID creates partial obstruction — enough to trap a fertilised ovum in the tube but not enough to prevent sperm ascent. The risk of ectopic pregnancy is seven-fold higher in women with a history of PID compared to those without. In clinical practice, a history of PID is one of the most important risk factors to elicit in any woman presenting with early pregnancy symptoms.
Chronic pelvic pain and dyspareunia:
Peritoneal adhesions, hydrosalpinx, and periovarian scarring contribute to chronic pelvic pain and deep dyspareunia in approximately 18% of women following PID. Fitz-Hugh-Curtis adhesions may cause persistent right upper quadrant or right subcostal pain that mimics biliary disease.
Recurrence:
Women who have had one episode of PID are at increased risk of recurrence — because the damaged cervical and tubal barriers are less effective at excluding ascending pathogens, and because risk behaviour may persist. Each recurrence adds to the cumulative tubal damage.
Long-Term Reproductive Risks After PID
Prevention:
- Consistent condom use: the single most effective personal prevention strategy
- STI screening and treatment: regular NAAT screening for chlamydia (and gonorrhoea) in sexually active women under 25, and in older women with risk factors — treating asymptomatic STIs prevents them from progressing to PID
- Partner notification and treatment: without treating the partner, re-infection and recurrence are inevitable
- Prompt treatment of STIs: a treated chlamydial infection cannot ascend to cause PID
- Safe IUCD insertion technique: peri-insertion antibiotic prophylaxis is not routinely recommended but NAAT screening before insertion is advised in high-risk women
CLINICAL PEARL
The CDC minimum criteria exist to protect the fallopian tube, not to protect diagnostic accuracy. The threshold for empirical PID treatment is deliberately low — CMT alone, or adnexal tenderness alone, or uterine tenderness alone is sufficient to start antibiotics in a sexually active woman. This is because the sensitivity of clinical diagnosis is imperfect, but the consequence of missing a mild PID episode and allowing tubal damage to accumulate silently is severe. The PEACH trial confirmed that outpatient treatment of mild-to-moderate PID achieves the same long-term fertility outcomes as inpatient treatment — the key is that treatment is started immediately. Do NOT wait for NAAT results. Also remember: always check a pregnancy test before treating pelvic pain as PID — ectopic pregnancy must be excluded, because both conditions can present with CMT and adnexal tenderness, but ectopic pregnancy is a surgical emergency.
Self-Assessment
You have now completed the full clinical arc for pelvic inflammatory disease — from the acute presentation dominated by cervical motion tenderness and bilateral adnexal pain, through the polymicrobial ascending pathophysiology in which STI pathogens initiate cervical breach and endogenous anaerobes amplify the infection, the CDC minimum criteria that justify immediate empirical treatment before laboratory confirmation, the triple-antibiotic outpatient and inpatient regimens that cover gonorrhoea/chlamydia/anaerobes simultaneously, the criteria for hospital admission and the management algorithm for tubo-ovarian abscess including the 72-hour surgical trigger, and the cumulative long-term consequences of infertility, ectopic pregnancy, and chronic pelvic pain that accumulate with each untreated or recurrent episode. You have also learned the unique features of Fitz-Hugh-Curtis syndrome and why PID must enter the differential diagnosis of any young woman presenting with right upper quadrant pain. Before attempting the question below, confirm in your mind the three components of the current outpatient regimen and the specific clinical threshold that would require this patient to be admitted instead of managed as an outpatient.
SELF-CHECK
Which of the following is the most appropriate outpatient antibiotic regimen for mild-to-moderate PID per CDC 2021 guidelines?
A. Azithromycin 1 g oral single dose plus doxycycline 100 mg BD × 7 days
B. Ceftriaxone 500 mg IM single dose plus doxycycline 100 mg BD × 14 days plus metronidazole 500 mg BD × 14 days
C. Ciprofloxacin 500 mg BD × 14 days plus metronidazole 500 mg BD × 14 days
D. Amoxicillin-clavulanate 875/125 mg BD × 14 days
Reveal Answer
Answer: B. Ceftriaxone 500 mg IM single dose plus doxycycline 100 mg BD × 14 days plus metronidazole 500 mg BD × 14 days
The CDC 2021 recommended outpatient PID regimen is: ceftriaxone 500 mg IM single dose (covers N. gonorrhoeae) PLUS doxycycline 100 mg oral BD × 14 days (covers C. trachomatis) PLUS metronidazole 500 mg oral BD × 14 days (anaerobic coverage — added in the 2021 update). Azithromycin single dose does not provide the prolonged coverage needed for chlamydia in PID (14 days required). Ciprofloxacin is no longer recommended for gonorrhoea due to resistance. Amoxicillin-clavulanate does not reliably cover C. trachomatis or N. gonorrhoeae.