Page 6 of 18
OG27.1 | Sexually Transmitted Infections — SDL Guide (Part 2)
Syndromic Management — NACO Guidelines
The syndromic management approach, formalised in India through NACO's STI/RTI management guidelines, is the accepted standard of care at the primary and secondary health-care level. It is grounded in the recognition that laboratory diagnosis is often unavailable, delayed, or prohibitively expensive in resource-limited primary care settings, and that the brief window at first presentation — when the patient has presented voluntarily, is symptomatic, and is potentially infectious — is the critical moment to treat and break the transmission chain. Waiting for laboratory results means the patient may not return for treatment. The approach therefore uses the clinical syndrome together with a structured epidemiological history (number and type of partners, nature of sexual contact, condom use, recent exposure, partner symptoms) to select a standardised empirical regimen that covers all pathogens statistically responsible for that syndrome. The regimen is deliberately broad-spectrum within the syndrome, accepting some over-treatment as a public health trade-off. Partner notification and concurrent partner treatment are non-negotiable components — they are explicitly required by NACO guidelines because an untreated partner guarantees re-infection and perpetuates the transmission chain.
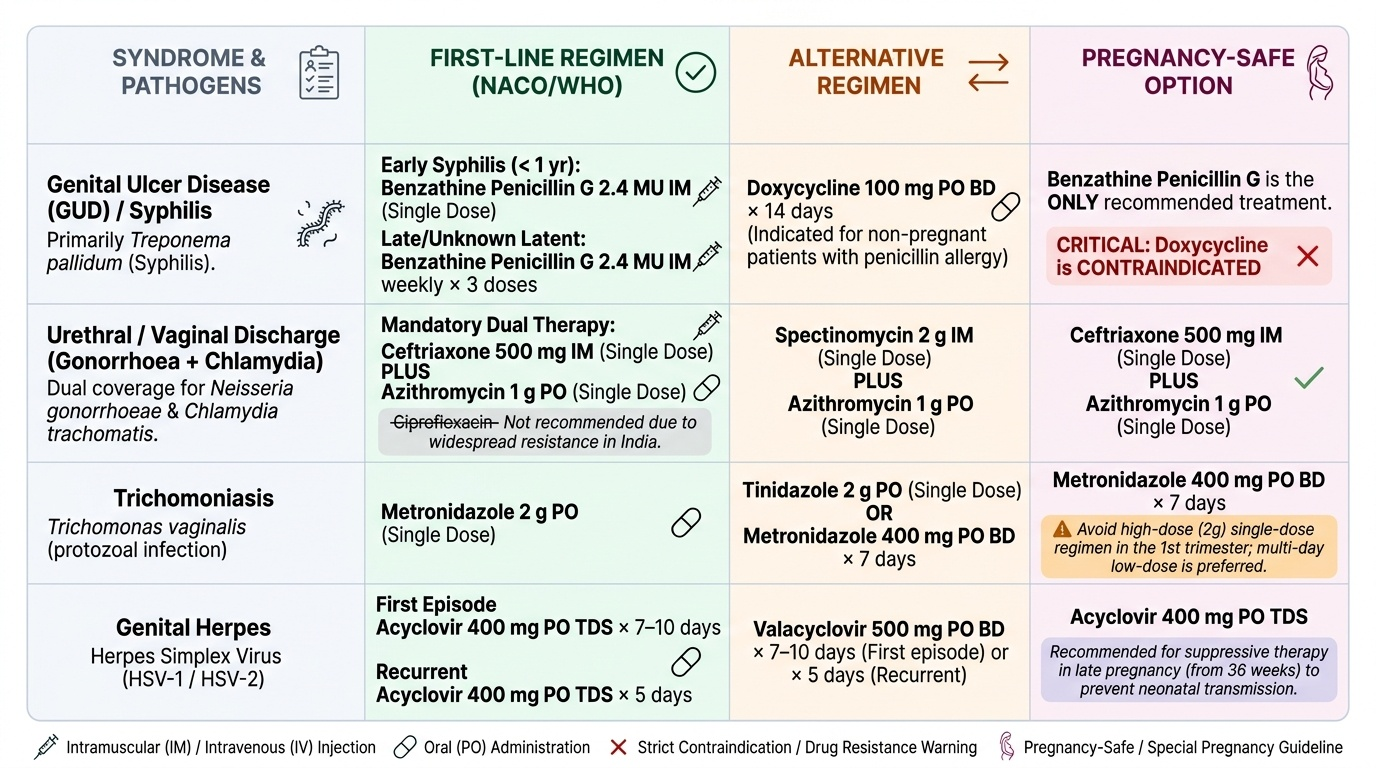
The key drug regimens for each major STI (per current NACO/MOHFW India and WHO guidelines) are:
Syphilis:
- Primary / secondary / early latent (<1 year): benzathine penicillin G 2.4 million units IM, single dose
- Late latent / unknown duration: benzathine penicillin G 2.4 MU IM weekly × 3 doses (total 7.2 MU)
- Neurosyphilis: aqueous crystalline penicillin G 18–24 MU IV daily × 10–14 days
- Penicillin allergy (non-pregnant): doxycycline 100 mg BD × 14 days (for primary/secondary/early latent)
- Pregnancy: benzathine penicillin is the ONLY recommended treatment for syphilis in pregnancy; doxycycline is contraindicated in pregnancy; erythromycin may be used but does not adequately treat the fetus
Gonorrhoea (NACO dual therapy — mandatory due to resistance):
- Ceftriaxone 500 mg IM single dose PLUS azithromycin 1 g oral single dose (for presumed/possible co-infecting chlamydia)
- Ciprofloxacin is NO LONGER recommended due to widespread fluoroquinolone resistance in N. gonorrhoeae in India
- In pregnancy: ceftriaxone is safe; azithromycin preferred over doxycycline
Chlamydia:
- Azithromycin 1 g oral single dose (preferred — single dose improves compliance)
- OR doxycycline 100 mg BD × 7 days
- In pregnancy: azithromycin 1 g single dose OR erythromycin 500 mg QID × 7 days (doxycycline is contraindicated)
Trichomoniasis:
- Metronidazole 2 g oral single dose OR metronidazole 400 mg BD × 7 days
- Treat the partner concurrently (otherwise recurrence is guaranteed)
- In pregnancy: metronidazole 400 mg BD × 7 days (avoid the 2 g single dose in first trimester per some guidelines)
Chancroid:
- Azithromycin 1 g oral single dose OR ceftriaxone 250 mg IM single dose
- Alternative: ciprofloxacin 500 mg BD × 3 days (check local resistance)
Genital herpes — first episode:
- Acyclovir 400 mg TDS × 7–10 days OR valacyclovir 1 g BD × 7–10 days
- Recurrent episodes: shorter course (5 days) or suppressive therapy (acyclovir 400 mg BD daily) for frequent recurrences (≥6/year)
- In pregnancy near term: suppressive acyclovir from 36 weeks reduces neonatal transmission risk; caesarean section considered if active lesions at onset of labour
Provided image
GUD syndromic management (NACO flowchart): At first visit, treat all genital ulcer patients with a regimen covering BOTH syphilis (benzathine penicillin 2.4 MU IM) AND chancroid (azithromycin 1 g oral or ceftriaxone 250 mg IM). If vesicles are present or there is a history of recurrent ulcers — add acyclovir (herpes treatment). Refer for VDRL/syphilis confirmatory testing. Do NOT withhold treatment while waiting for results.
Partner notification and treatment are mandatory under NACO guidelines and ethically obligatory. The patient should be counselled to inform all sexual contacts within the relevant exposure window (primary syphilis: 3 months; secondary: 6 months; gonorrhoea/chlamydia: 60 days), and these contacts should be screened and treated. Condom promotion at every contact.
SELF-CHECK
A 24-year-old pregnant woman (12 weeks) presents with vaginal discharge and is found to have gonorrhoea on NAAT. Which regimen is most appropriate?
A. Ciprofloxacin 500 mg BD × 3 days
B. Doxycycline 100 mg BD × 7 days
C. Ceftriaxone 500 mg IM single dose plus azithromycin 1 g oral single dose
D. Metronidazole 2 g oral single dose
Reveal Answer
Answer: C. Ceftriaxone 500 mg IM single dose plus azithromycin 1 g oral single dose
NACO dual therapy for gonorrhoea is ceftriaxone 500 mg IM PLUS azithromycin 1 g oral — ceftriaxone covers N. gonorrhoeae and azithromycin covers co-infecting chlamydia. Both are safe in pregnancy. Ciprofloxacin is no longer recommended due to widespread resistance. Doxycycline is contraindicated in pregnancy (affects fetal bone/teeth). Metronidazole treats trichomoniasis, not gonorrhoea.
Long-Term Implications and Prevention
The long-term consequences of untreated or inadequately treated STIs extend well beyond the primary infection, affecting reproductive health, neonatal outcomes, and HIV transmission dynamics. Every clinician managing STIs must understand these implications in order to counsel patients effectively and justify the urgency of treatment and partner management.
Reproductive tract consequences:
Gonorrhoea and chlamydia are the principal causes of pelvic inflammatory disease (PID) when they ascend from the cervix to the endometrium and fallopian tubes. PID leads to tubal inflammation, scarring, and occlusion — resulting in tubal-factor infertility (15–20% risk after one PID episode, rising to >50% after three episodes) and a 7-fold increased risk of ectopic pregnancy due to impaired tubal transport. Chronic pelvic pain and dyspareunia are additional long-term sequelae. Chlamydial infection is the most common preventable cause of infertility in women.
Neonatal and congenital transmission:
- Congenital syphilis: transplacental transmission of T. pallidum, particularly in secondary and early latent syphilis when spirochaetaemia is highest. Consequences include stillbirth, early congenital syphilis (rash, snuffles, hepatosplenomegaly, pseudoparalysis of Parrot), and late congenital syphilis (Hutchinson's triad: interstitial keratitis, eighth nerve deafness, Hutchinson's teeth). India's NHM mandates antenatal VDRL screening to prevent this.
- Neonatal conjunctivitis (ophthalmia neonatorum): acquired from gonorrhoea or chlamydia during passage through the infected birth canal. Gonococcal conjunctivitis appears within 2–5 days of birth — a hyperacute purulent conjunctivitis that can cause corneal scarring and blindness if untreated. Chlamydial conjunctivitis appears at 5–14 days. Credé prophylaxis (1% silver nitrate or antibiotic eye drops at birth) prevents gonococcal ophthalmia.
- Neonatal herpes: HSV-2 transmitted perinatally; can cause disseminated neonatal herpes (encephalitis, multi-organ failure) — high mortality. Caesarean section is recommended when active genital herpes lesions are present at onset of labour.
HIV co-infection:
Genital ulcers (from syphilis, herpes, chancroid) disrupt the mucosal barrier and increase HIV acquisition and transmission by 3–5 fold. Gonorrhoea and chlamydia increase genital tract HIV shedding even without ulceration. Effective STI treatment and management is therefore a key component of HIV prevention — this is the biological basis of the 'STI control as HIV prevention' strategy.
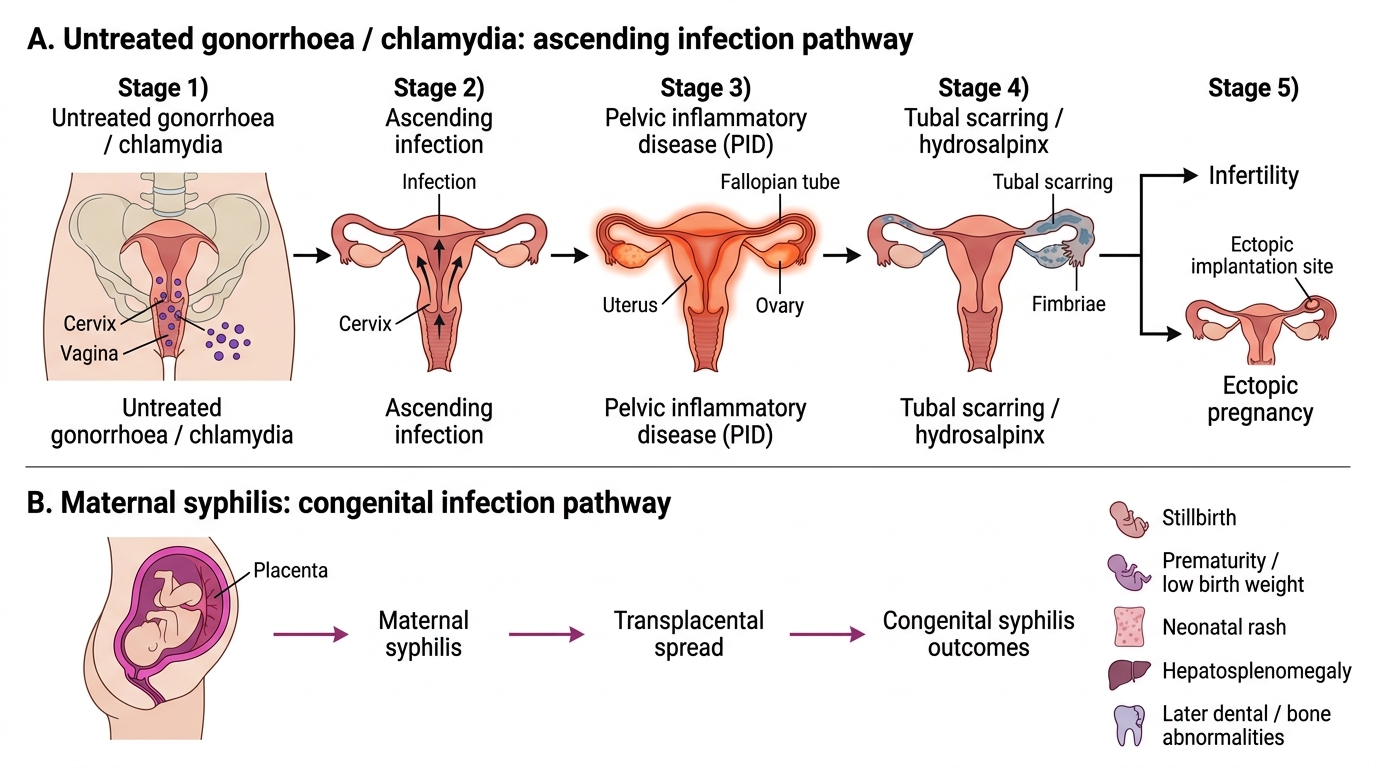
Ascending STI Infection and Congenital Syphilis Pathways
Prevention:
- Consistent condom use: male latex condoms provide ~80-85% protection against HIV, gonorrhoea, and chlamydia when used correctly; less effective against HSV and HPV (skin-to-skin contact)
- Partner notification and treatment: mandatory component of every STI management encounter
- Antenatal screening: syphilis (VDRL), HIV, and hepatitis B for all pregnant women under NHM
- Behaviour change communication: reduce number of concurrent partners, delay sexual debut
- Vaccination: HPV vaccine (Cervarix / Gardasil) given to adolescent girls as part of India's immunisation programme — prevents cervical cancer from HPV 16/18; HBV vaccine for hepatitis B
CLINICAL PEARL
Two critical drug-choice traps for the examination:
(1) Ciprofloxacin for gonorrhoea is NO LONGER recommended in India — widespread resistance means dual therapy with ceftriaxone + azithromycin is now mandatory, even in asymptomatic contacts. Any examination question offering ciprofloxacin as a 'correct' first-line for gonorrhoea in the current era is outdated.
(2) Doxycycline is CONTRAINDICATED in pregnancy — it causes discolouration and dysplasia of developing fetal bones and teeth. For syphilis in pregnancy, benzathine penicillin is the only safe option. For chlamydia in pregnancy, use azithromycin 1 g single dose (safe) or erythromycin 500 mg QID × 7 days. Tetracyclines (doxycycline, tetracycline) are universally contraindicated in pregnancy.
Self-Assessment
You have now covered the complete clinical arc for sexually transmitted infections — from the pathogen taxonomy and clinical syndrome recognition, through the pathogenesis of genital ulcer formation and ascending infection, to the NACO syndromic management flowcharts, drug regimens including pregnancy-safe alternatives, and the long-term sequelae including infertility, congenital syphilis, neonatal conjunctivitis, and HIV co-facilitation. Before attempting the integrative question below, review the three critical decision points: First — can you distinguish a painless syphilitic chancre from a painful chancroid ulcer from a cluster of herpetic vesicles at the bedside, and which investigation confirms each? Second — in a pregnant woman with reactive syphilis serology and a claimed penicillin allergy, do you know why no alternative antibiotic adequately replaces benzathine penicillin for preventing congenital syphilis, and what the correct management pathway is? Third — can you state the NACO dual-therapy regimen for gonorrhoea and explain why ciprofloxacin is no longer acceptable? The question that follows is designed to test the integration of these decision points in a realistic clinical scenario.
SELF-CHECK
A 26-year-old woman at 18 weeks of pregnancy is found to have a reactive VDRL at 1:32 and a reactive TPHA on antenatal screening. She is asymptomatic. She reports penicillin allergy. What is the most appropriate treatment for her syphilis?
A. Doxycycline 100 mg BD × 14 days
B. Azithromycin 2 g oral single dose
C. Benzathine penicillin G 2.4 MU IM after penicillin desensitisation
D. Erythromycin 500 mg QID × 14 days — safe in pregnancy and effective for syphilis
Reveal Answer
Answer: C. Benzathine penicillin G 2.4 MU IM after penicillin desensitisation
Benzathine penicillin is the ONLY reliably effective treatment for syphilis in pregnancy and the ONLY agent proven to prevent congenital syphilis. Penicillin allergy is NOT a contraindication — the patient should undergo penicillin desensitisation protocol and then receive benzathine penicillin G. Doxycycline is contraindicated in pregnancy. Azithromycin has shown resistance in T. pallidum (23S rRNA mutation) and is no longer reliably effective. Erythromycin does not adequately cross the placenta to treat fetal syphilis — the baby will require post-natal treatment even if the mother is treated with erythromycin.