Page 18 of 24
OG30.2 | Hyper-Androgenism — SDL Guide (Part 2)
Investigations: Biochemical and Imaging Workup
The investigation of hyperandrogenism is guided by two clinical questions: how severe is the androgen excess (is this an emergency or a routine workup?), and which compartment — ovarian, adrenal, or peripheral — is the source? These questions should be answered in sequence, because a markedly elevated testosterone should prompt urgent imaging before the full hormone panel is even interpreted. Critically, the clinical presentation drives the investigation priority: a woman with rapid-onset virilisation and testosterone >200 ng/dL needs imaging before anything else; a woman with gradual hirsutism and oligomenorrhoea follows a more measured protocol. In routine clinical practice, blood is drawn in the follicular phase of the menstrual cycle (days 2-5) because LH, FSH, and 17-OHP are most interpretable at that time point; if the woman is amenorrhoeic, samples can be taken on any day. The investigation set is divided into a first-line biochemical screen available at any district hospital, and a second-line confirmatory tier triggered by specific abnormalities in the first line.
First-line biochemical screen (all women with significant hirsutism, mFG ≥8, or menstrual irregularity):
- Total testosterone — the most important initial test. Mildly elevated (<200 ng/dL) = PCOS or idiopathic; markedly elevated (>200 ng/dL) = urgent ovarian/adrenal imaging for tumour
- DHEAS — adrenal androgen marker; normal or mildly elevated in PCOS; very elevated (>700 µg/dL) = adrenal source (carcinoma until proven otherwise)
- LH, FSH — to assess HPO axis; FSH elevation = primary ovarian insufficiency; low LH+FSH = hypothalamic amenorrhoea
- Prolactin — to exclude hyperprolactinaemia
- TSH — to exclude thyroid disease
- Morning 17-hydroxyprogesterone (17-OHP), follicular phase — screen for late-onset CAH; >2 ng/mL → proceed to ACTH stimulation test
- Fasting glucose and lipid profile — metabolic screening (especially if PCOS suspected)
Second-line confirmatory tests (triggered by first-line abnormalities):
- ACTH stimulation test (Synacthen test) — for 17-OHP >2 ng/mL: give 250 µg synthetic ACTH IV/IM, measure 17-OHP at 60 min; peak >10 ng/mL = confirms late-onset CAH
- 24-hour urinary free cortisol or overnight low-dose dexamethasone suppression test (LDDST) — for suspected Cushing syndrome (1 mg dexamethasone at 11 PM; morning cortisol >1.8 µg/dL = abnormal)
- Free testosterone / sex hormone-binding globulin (SHBG) — for women with borderline total testosterone; low SHBG (hyperinsulinaemia) elevates free androgen fraction
Imaging:
- Pelvic ultrasound (TVS) — assess ovarian morphology (PCOM), exclude adnexal mass
- CT abdomen and pelvis — if total testosterone >200 ng/dL or DHEAS >700 µg/dL (adrenal/ovarian tumour workup)
- MRI adrenal glands — for suspected adrenal tumour when CT is equivocal
| Clinical scenario | Key investigation | Interpretation |
|---|---|---|
| Gradual hirsutism + oligomenorrhoea | Testosterone, DHEAS, 17-OHP, USG | PCOS most likely; exclude CAH (17-OHP), thyroid, prolactin |
| 17-OHP >2 ng/mL | ACTH stimulation test | Peak >10 ng/mL = late-onset CAH |
| Rapid virilisation + testosterone >200 ng/dL | CT pelvis/abdomen | Ovarian or adrenal tumour |
| Cushingoid features | 24-h UFC or overnight LDDST | Cortisol excess |
| Normal androgens + regular cycles + hirsutism | Full panel; all normal | Idiopathic hirsutism |
SELF-CHECK
A 28-year-old woman with hirsutism has a morning 17-OHP of 4.8 ng/mL (follicular phase). Her testosterone is 110 ng/dL and DHEAS is 310 µg/dL. What is the most appropriate next investigation?
A. Pelvic ultrasound to assess ovarian morphology
B. ACTH stimulation test
C. 24-hour urinary free cortisol
D. MRI of the adrenal glands
Reveal Answer
Answer: B. ACTH stimulation test
A morning basal 17-OHP >2 ng/mL (follicular phase) triggers an ACTH stimulation test to investigate for late-onset (non-classic) congenital adrenal hyperplasia due to 21-hydroxylase deficiency. A peak 17-OHP >10 ng/mL at 60 minutes after 250 µg synthetic ACTH confirms the diagnosis. Pelvic ultrasound, urinary cortisol, and adrenal MRI are appropriate in other scenarios but are not the immediate next step here.
Management of Hyperandrogenism
Management of hyperandrogenism follows two parallel tracks that must be addressed together: treating the underlying cause (cause-directed therapy) and managing the symptoms of androgen excess that are distressing the patient (symptom-directed therapy). The urgency and nature of cause-directed therapy varies enormously — from the patient watchfulness of idiopathic hirsutism to emergency surgery for a virilising ovarian tumour. Symptom management — reducing hirsutism and restoring menstrual regularity — can be initiated while investigations are ongoing, with the exception of anti-androgens (which require confirmed diagnosis and contraceptive cover before prescribing).
Cause-directed therapy by diagnosis:
PCOS: Lifestyle modification (first-line), followed by COC and/or metformin and letrozole for fertility — fully detailed in the PCOS SDL.
Late-onset CAH (21-hydroxylase deficiency): The primary treatment is low-dose hydrocortisone (10-20 mg/day in divided doses) or prednisolone, which suppresses ACTH drive and reduces adrenal androgen output. This is fundamentally different from PCOS management — the lesion is adrenal, not ovarian. Hormone replacement to near-physiological cortisol levels is the goal; over-replacement causes iatrogenic Cushing syndrome. Women with late-onset CAH who wish to conceive benefit from hydrocortisone-facilitated ovulation restoration.
Androgen-secreting tumour (ovarian or adrenal): Surgical removal is the treatment of choice. Most ovarian androgen-secreting tumours are unilateral; fertility-sparing unilateral salpingo-oophorectomy is appropriate for women of reproductive age with benign tumours. Adrenal carcinoma requires adrenalectomy with oncological follow-up.
Cushing syndrome: Treatment depends on the cause — transsphenoidal surgery for pituitary adenoma (Cushing disease), adrenalectomy for adrenal adenoma, treatment of the primary tumour for ectopic ACTH.
Symptom-directed therapy (hirsutism):
Hormonal:
- Combined oral contraceptive pill (COC) — suppresses LH-driven ovarian androgen production and raises SHBG, reducing free testosterone. Use a formulation with a non-androgenic progestogen (drospirenone, desogestrel, norgestimate). Apply WHO MEC category assessment before prescribing.
- Spironolactone (100-200 mg/day) — an aldosterone antagonist with anti-androgenic properties; blocks the androgen receptor and inhibits 5α-reductase. Effective for hirsutism and acne in women who cannot take COC (or as an add-on). Requires concurrent reliable contraception — spironolactone is teratogenic (feminises a male fetus). Monitor potassium and blood pressure.
- Finasteride (5 mg/day) — type 2 5α-reductase inhibitor; reduces DHT in hair follicles. Less used in Indian practice; requires contraception.
- Flutamide — non-steroidal anti-androgen; hepatotoxicity limits use.
Cosmetic:
- Mechanical hair removal (shaving, waxing, threading, electrolysis, laser hair removal) — address the symptom directly; no hormonal effect. Laser is most effective for long-term reduction.
- Topical eflornithine — inhibits ornithine decarboxylase in follicular cells; reduces facial hair growth rate; used adjunctively.
IMPORTANT counselling point: hormonal treatments slow new hair growth but do not eliminate existing terminal hair, which must be removed by cosmetic methods. Patients should be counselled to expect 6-12 months of treatment before a significant reduction in hair growth rate is apparent.
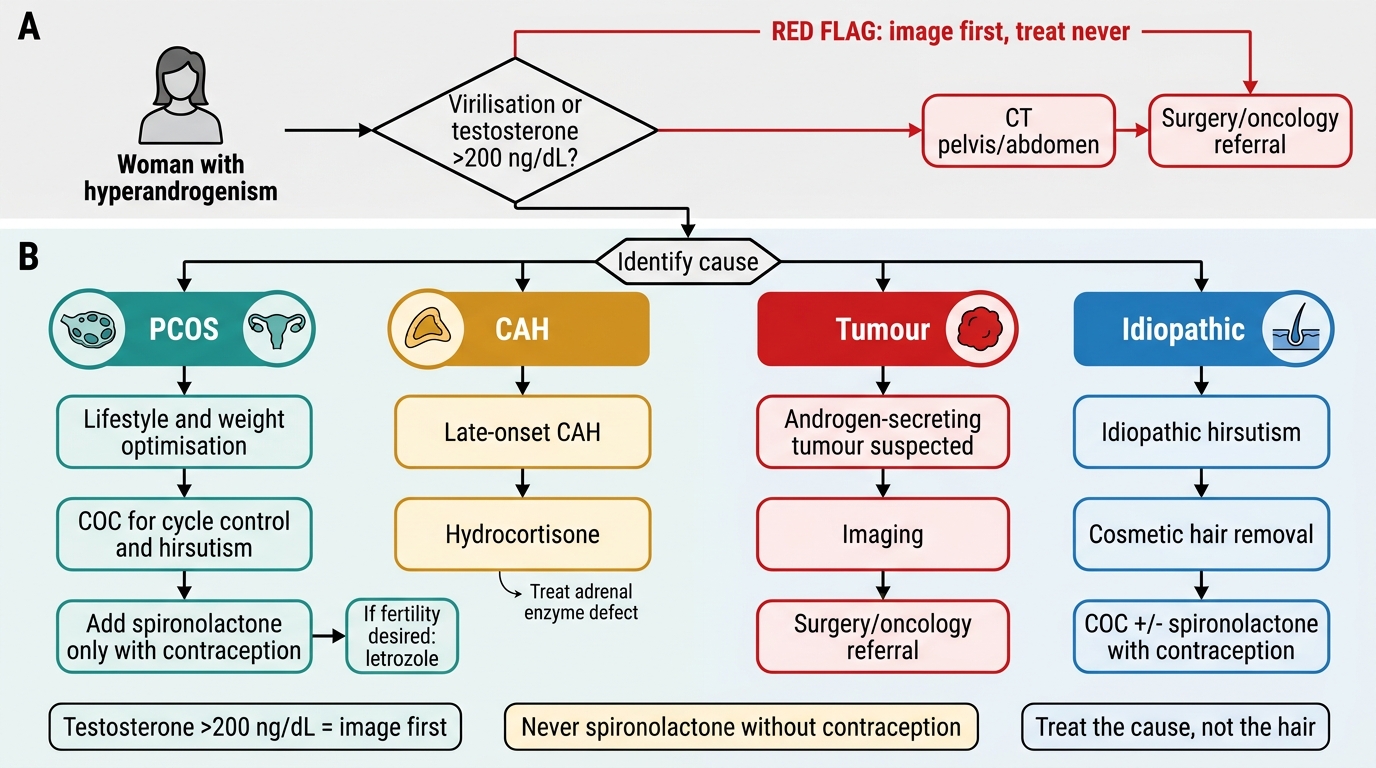
Management Algorithm for Hyperandrogenism
CLINICAL PEARL
Three clinical pearls that prevent common management errors in hyperandrogenism:
1. Testosterone >200 ng/dL = image first, treat never. A woman with this level of testosterone has an androgen-secreting tumour until proven otherwise. Starting COC while awaiting investigations delays diagnosis of a potentially malignant tumour. Order CT pelvis/abdomen before any hormonal therapy.
2. Spironolactone must never be given without contraception. It is teratogenic — it blocks androgen receptors in a male fetus, causing external genital feminisation. Every prescription should document the chosen contraceptive method.
3. Treat the cause, not the hair. Late-onset CAH requires hydrocortisone, not COC. Starting COC in late-onset CAH controls symptoms cosmetically but does not correct the adrenal enzyme defect, leaving adrenal androgens elevated and the risk of adrenal crisis in physiological stress untreated.
SELF-CHECK
A 25-year-old woman with newly confirmed late-onset CAH (non-classic 21-hydroxylase deficiency) asks for treatment. She is not planning pregnancy now but may wish to in the future. What is the first-line treatment for her condition?
A. Combined oral contraceptive pill to suppress LH
B. Spironolactone 100 mg daily to block the androgen receptor
C. Hydrocortisone 10-20 mg/day in divided doses
D. Letrozole to induce ovulation
Reveal Answer
Answer: C. Hydrocortisone 10-20 mg/day in divided doses
Late-onset CAH is caused by partial 21-hydroxylase deficiency, leading to ACTH-driven excess adrenal androgen production. The cause-directed treatment is glucocorticoid replacement with hydrocortisone (10-20 mg/day in divided doses), which suppresses ACTH and reduces adrenal androgen output. COC and spironolactone treat symptoms but do not address the underlying adrenal enzyme defect. Letrozole is for ovulation induction in PCOS and is not relevant here.
Self-Assessment: Hyperandrogenism
Use the following questions to test your understanding of the systematic approach to hyperandrogenism. Attempt each before reading the answer.
Q1. A 30-year-old woman has had coarse facial hair, temporal hair loss, and clitoral enlargement that has progressed over 9 months. Her testosterone is 310 ng/dL. What is the most urgent action?
Answer: This is rapid-onset virilisation with markedly elevated testosterone (>200 ng/dL) — a clinical emergency. The most urgent action is CT imaging of the pelvis and abdomen to identify an androgen-secreting ovarian or adrenal tumour. Hormonal therapy should be withheld until a tumour is excluded. Surgical referral should be concurrent with imaging.
Q2. A 22-year-old woman has an mFG score of 12, regular cycles, and normal serum testosterone, DHEAS, TSH, and prolactin. Morning 17-OHP is 0.8 ng/mL. What is the diagnosis?
Answer: Idiopathic hirsutism. She has significant hirsutism (mFG ≥8) but all androgens are normal, cycles are regular, and Rotterdam criteria for PCOS are not met. The mechanism is increased skin 5α-reductase activity. Management is symptom-directed: COC with a non-androgenic progestogen and/or cosmetic hair removal; spironolactone may be added with contraception.
Q3. Why does late-onset CAH cause androgen excess rather than cortisol deficiency?
Answer: Late-onset CAH is caused by a partial (not complete) deficiency of 21-hydroxylase (CYP21A2). The block is partial enough that basal cortisol secretion is near-normal at rest. However, 17-OHP accumulates behind the partial block and is shunted via CYP17A1 into the androgen pathway (producing androstenedione and DHEAS). The high ACTH drive (from incomplete cortisol feedback) amplifies adrenal androgen output further. The clinical result is hyperandrogenism with minimal cortisol deficiency.
Q4. A woman with hirsutism and PCOS is prescribed spironolactone. She asks why she also needs to take a contraceptive pill. Explain in terms suitable for patient counselling.
Answer: Spironolactone blocks androgen receptors throughout the body. During pregnancy, androgens are essential for the normal development of external genitalia in a male fetus. If a male fetus is exposed to spironolactone in the womb, its external genitalia may not masculinise normally. For this reason, spironolactone must never be taken during pregnancy. Taking a reliable contraceptive pill alongside spironolactone ensures you do not become pregnant while on this medication.