Page 8 of 24
OG28.3 | Ovulation Induction — SDL Guide (Part 2)
Management of Complications: OHSS and Multiple Pregnancy
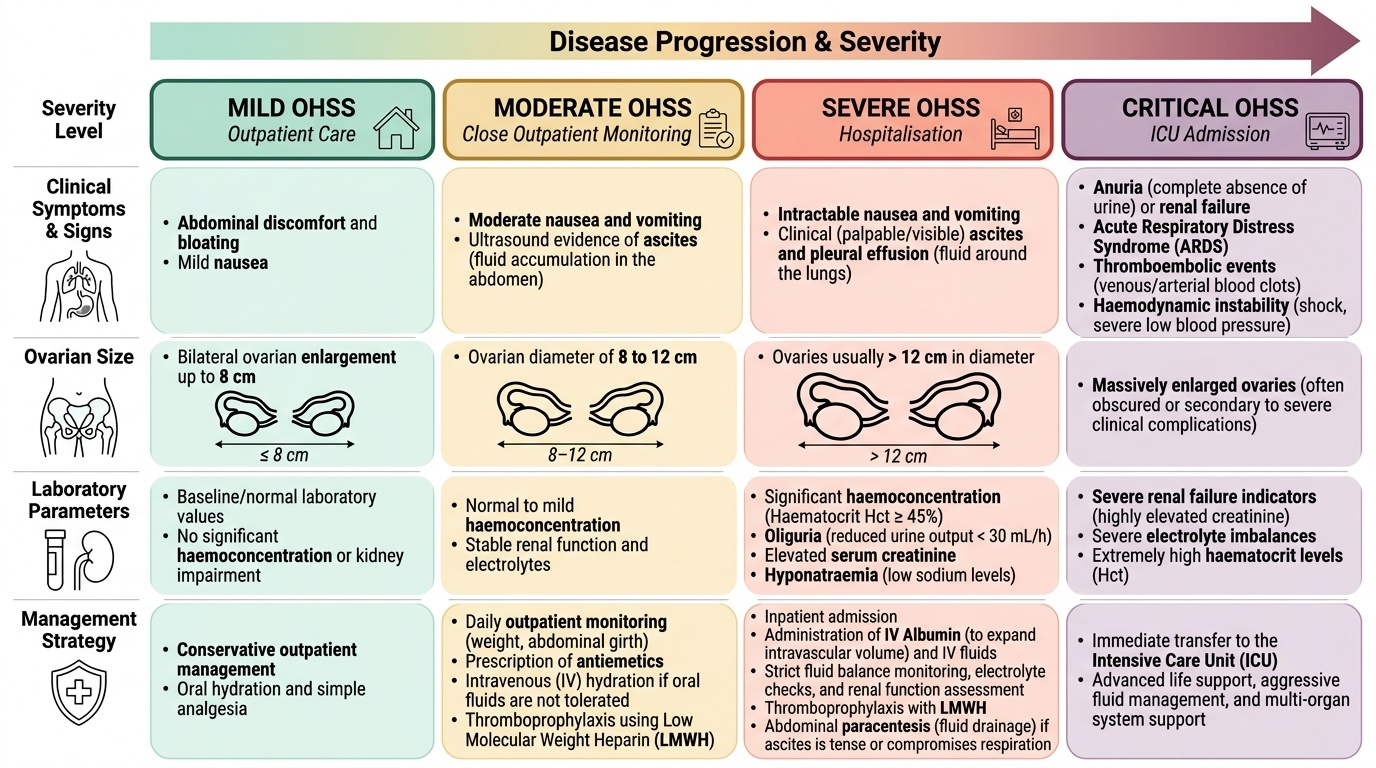
Ovarian hyperstimulation syndrome (OHSS) is an iatrogenic complication of ovulation induction that every clinician managing these patients must be able to recognise and grade quickly. It results from an excessive ovarian response to gonadotrophins — occasionally to clomiphene, and very rarely to letrozole — in which the hyperstimulated ovaries release massive quantities of vascular endothelial growth factor (VEGF) and other vasoactive substances. VEGF dramatically increases vascular permeability throughout the body, causing protein-rich fluid to leak from the intravascular compartment into third spaces: the peritoneal cavity (ascites), the pleural cavity (pleural effusion), and rarely the pericardium. As plasma volume contracts, haemoconcentration develops (rising haematocrit), with downstream effects including renal hypoperfusion, oliguria, and — most dangerously — hypercoagulability, which creates a profound risk of venous and arterial thromboembolism. The severity of OHSS exists on a spectrum, and early recognition of progression from mild to moderate or severe is what determines whether a patient can be managed safely as an outpatient or requires hospitalisation and intensive monitoring. OHSS is graded by severity:
- Mild OHSS: abdominal discomfort and bloating, mild nausea, bilateral ovarian enlargement up to 8 cm; managed conservatively as outpatient with analgesia and hydration.
- Moderate OHSS: moderate nausea and vomiting, ultrasound evidence of ascites, ovaries 8–12 cm; requires close outpatient monitoring; antiemetics, IV hydration if unable to tolerate oral fluids; thromboprophylaxis (LMWH).
- Severe OHSS: intractable nausea/vomiting, clinical ascites, pleural effusion, haemoconcentration (Hct >45%), oliguria (urine output <30 mL/h), elevated creatinine, hyponatraemia; requires hospitalisation for IV albumin (to expand intravascular volume), IV hydration, LMWH, close monitoring of fluid balance, electrolytes, and renal function. Abdominal paracentesis if ascites is tense or compromises respiration.
- Critical/life-threatening OHSS: renal failure, ARDS, thromboembolic events, haemodynamic instability; requires ICU care.
Prevention of OHSS is far preferable to treatment:
- Identify high-risk patients before starting: PCOS, young age (<30 years), low BMI, high AFC (>20), high AMH (>3.5 ng/mL), previous OHSS.
- Use the step-up gonadotrophin protocol with low starting doses.
- Strict USS monitoring: cancel the cycle if >3 dominant follicles ≥14 mm or oestradiol >2,500 pg/mL.
- Cycle abandonment: the patient is counselled to avoid intercourse or insemination; follicle aspiration may drain follicles.
- Use letrozole or clomiphene rather than gonadotrophins whenever possible.
- In ART cycles, a GnRH agonist trigger rather than hCG for final oocyte maturation, followed by a freeze-all strategy, almost eliminates early OHSS (hCG has a much longer luteal phase VEGF-driving effect than a GnRH agonist trigger).
Multiple pregnancy is the other major complication. Gonadotrophins carry a 20–30% multiple pregnancy rate if >1 follicle is triggered; clomiphene has a ~8–10% twin rate; letrozole has the lowest (~3–5%). All patients on OI must be counselled about the risks of twin and higher-order pregnancy — including preterm birth, maternal complications, and neonatal morbidity. Cycles with ≥3 mature follicles should be cancelled or converted to IVF with single embryo transfer.
Provided image
SELF-CHECK
A 27-year-old woman with PCOS on gonadotrophin stimulation is monitored by USS on day 10. She has 5 follicles ≥14 mm bilaterally and feels markedly bloated. Her serum oestradiol is 3,100 pg/mL. What is the most appropriate action?
A. Trigger ovulation with hCG 10,000 IU and advise timed intercourse
B. Increase the gonadotrophin dose to mature all follicles simultaneously
C. Cancel the cycle to prevent OHSS and multiple pregnancy; advise against intercourse
D. Reduce the gonadotrophin dose and repeat USS in 2 days
Reveal Answer
Answer: C. Cancel the cycle to prevent OHSS and multiple pregnancy; advise against intercourse
This cycle must be cancelled. Five mature follicles (≥14 mm) and an oestradiol >2,500 pg/mL are both absolute indications for cycle abandonment to prevent severe OHSS and high-order multiple pregnancy. Triggering with hCG in this situation would be dangerous. Increasing the dose would further worsen ovarian hyperstimulation. Reducing the dose at this stage when multiple dominant follicles are already present does not undo the stimulation — cancellation is the only safe option.
Self-Assessment and Clinical Decision-Making in Ovulation Induction
By now you should be able to construct the complete clinical decision framework for ovulation induction. The framework has four interlocking components that must work in sequence: first, classify the anovulation by WHO group using the hormonal profile; second, select the appropriate first-line agent based on the WHO group, the patient's BMI and insulin resistance status, and available monitoring resources; third, explain the regimen and its rationale to the patient in accessible terms, including the evidence base and the off-label status of letrozole where applicable; and fourth, monitor the cycle appropriately and recognise the threshold criteria that mandate cycle cancellation to prevent OHSS and multiple pregnancy. A clinician who can do all four of these competently is equipped to manage the vast majority of anovulatory infertility at the secondary care level. The structured self-check below tests each component. Let us consolidate with a structured review of the decision points.
Agent selection by clinical scenario:
- PCOS, BMI normal to overweight, clomiphene-naive: letrozole 2.5 mg days 2–6 (first-line, PPCOS II evidence)
- PCOS, letrozole unavailable: clomiphene 50 mg days 2–6 (second-line)
- PCOS, clomiphene-resistant, obese/insulin-resistant: add metformin + reassess; or switch to letrozole
- WHO Group I (hypogonadotrophic — hypothalamic amenorrhoea): gonadotrophins (± underlying cause correction); address weight, stress
- WHO Group II, all oral agents failed after adequate trial: injectable gonadotrophins with USS monitoring
- WHO Group III (hypergonadotrophic — POI): donor oocytes — no standard OI will work
Counselling points patients always ask:
- Twins risk: letrozole ~3–5%, clomiphene ~8–10%, gonadotrophins ~20–30% if not carefully monitored
- Letrozole off-label use in India — this should be explained; evidence base is clear (PPCOS II, 2014)
- OHSS risk: low with oral agents, significant with gonadotrophins especially in PCOS/high AFC
- Duration of treatment before escalating: 3–6 cycles of oral agents is standard
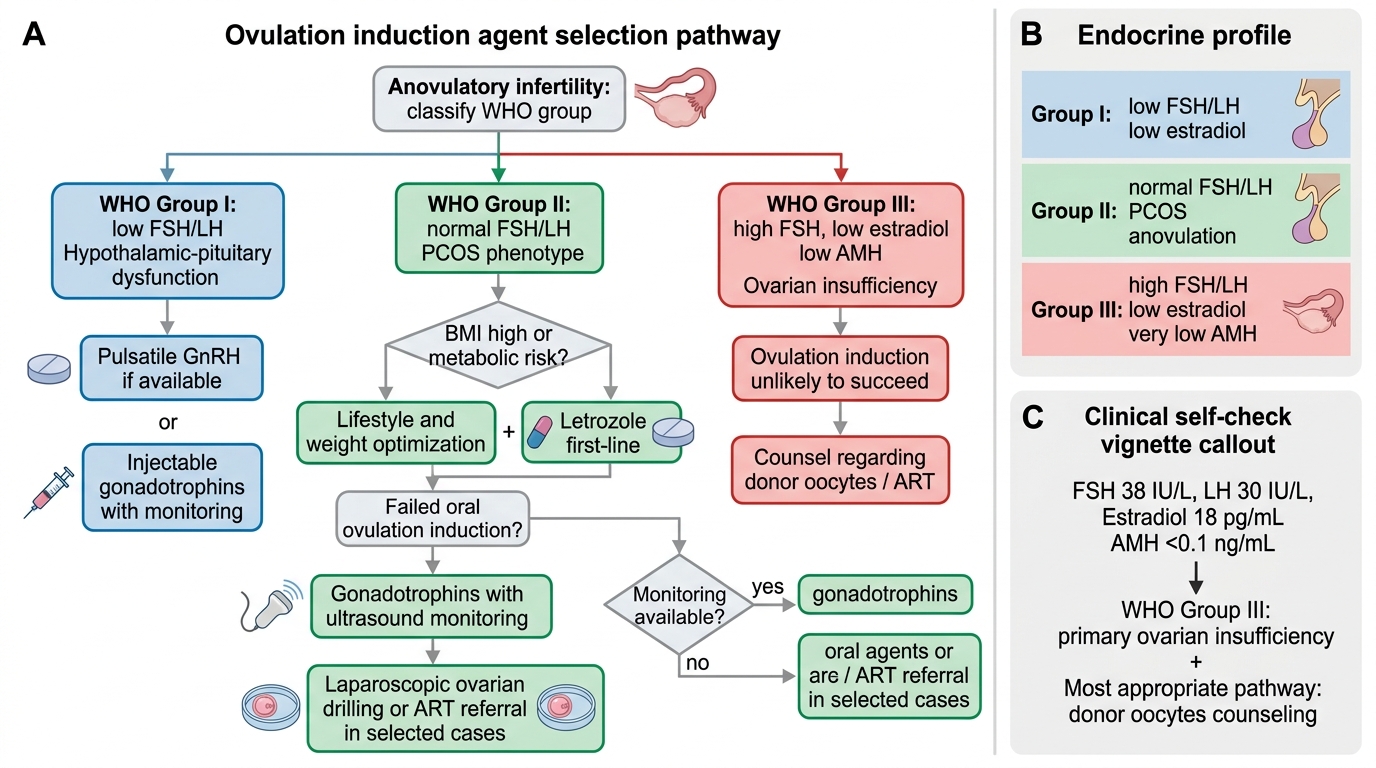
Ovulation Induction Agent Selection by WHO Anovulation Group
SELF-CHECK
A 34-year-old woman has a hormonal profile showing FSH 38 IU/L, LH 30 IU/L, oestradiol 18 pg/mL, and AMH <0.1 ng/mL. She has irregular cycles and has been trying to conceive for 2 years. What is her WHO anovulation group and the most appropriate fertility treatment?
A. WHO Group I; treat with pulsatile GnRH
B. WHO Group II; treat with letrozole first-line
C. WHO Group III; ovulation induction is unlikely to succeed — counsel regarding donor oocytes
D. WHO Group II; treat with injectable gonadotrophins
Reveal Answer
Answer: C. WHO Group III; ovulation induction is unlikely to succeed — counsel regarding donor oocytes
Elevated FSH (38 IU/L), elevated LH, very low oestradiol, and near-undetectable AMH indicate hypergonadotrophic hypogonadism — WHO Group III, consistent with premature ovarian insufficiency (POI). The pituitary is already maximally stimulating a depleted ovary. Exogenous gonadotrophins or oral agents will not restore ovarian function in true POI. Oocyte donation is the primary pathway to pregnancy. WHO Group I has low FSH/LH; WHO Group II has normal FSH/LH with the features of PCOS.
CLINICAL PEARL
Letrozole is currently used off-label for ovulation induction in many countries, including India, yet it has level-1 evidence superiority over clomiphene (PPCOS II, NEJM 2014) and is endorsed as first-line by major international societies including ESHRE and ASRM. When prescribing, always document the evidence basis and obtain informed consent for off-label use. Also remember: the absence of OHSS with oral OI agents does not eliminate all risk — clomiphene carries a ~8–10% twin rate. Every patient on any OI agent must be counselled that twins significantly increase obstetric risk, and that multiple-follicle cycles with gonadotrophins should be cancelled rather than triggered.