Page 4 of 24
OG28.2 | Tubal Patency Assessment — SDL Guide
Learning Objectives
- State the clinical indications for assessing tubal patency in the infertile couple
- Describe the technique and findings of hysterosalpingography (HSG) and its limitations
- Compare HSG, saline sonohysterography (SSG/HyCoSy), and diagnostic laparoscopy with chromopertubation as methods of tubal assessment
- Interpret common findings on tubal patency assessment: normal, proximal block, distal occlusion, hydrosalpinx
- Outline surgical and ART options for restoration of tubal patency and indications for each
INSTRUCTIONS
The fallopian tubes are the site of fertilisation and of the first days of embryo transport — their patency is a prerequisite for natural conception. Tubal disease accounts for up to 30% of female infertility, yet it is clinically silent: there is no symptom that reliably distinguishes a patent from a blocked tube. This SDL teaches you the investigative toolkit — from the outpatient HSG to the gold-standard laparoscopic dye test — so that you can select, interpret, and act on tubal patency assessments appropriately.
References
- DC Dutta's Textbook of Gynaecology, 8th edition, Ch 18 (Infertility — Tubal Factor) (textbook)
- Shaw's Textbook of Gynaecology, 17th edition, Ch 23 (textbook)
- NICE Fertility Guideline CG156, updated 2017 — Tubal assessment section (guideline)
- Strandell A et al. Hydrosalpinx and IVF outcome — RCT evidence (Lancet 1999) (journal)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 29-year-old woman presents with two years of primary infertility. Her cycles are regular at 28 days, ovulation is confirmed by mid-luteal progesterone, her hormonal profile is normal, and her husband's semen analysis is normal. There is no history of pelvic infection, surgery, or dysmenorrhoea. The only remaining question is: are her tubes patent? You order a hysterosalpingogram. The radiologist's report reads: 'Right tube fills and spills freely. Left tube fills to the isthmus only — no spill. Features consistent with left cornual block, possibly spasm-related.' What do you do next — and what does this finding actually mean?
WHY THIS MATTERS
Tubal factor infertility is responsible for approximately 25–35% of female infertility, making it one of the two most common identifiable causes alongside ovulatory dysfunction. What makes tubal disease particularly challenging is that it produces no reliable symptoms in many women — a woman with bilateral hydrosalpinges and irreversibly damaged tubes may have perfectly regular cycles and no pelvic pain. The only way to detect tubal disease is to specifically test for it. As a final-year student and future clinician, you must understand which test to select for which clinical scenario, what the findings mean, and how to translate those findings into a management decision — including the critical question of when surgery can restore fertility versus when IVF is the better path.
RECALL
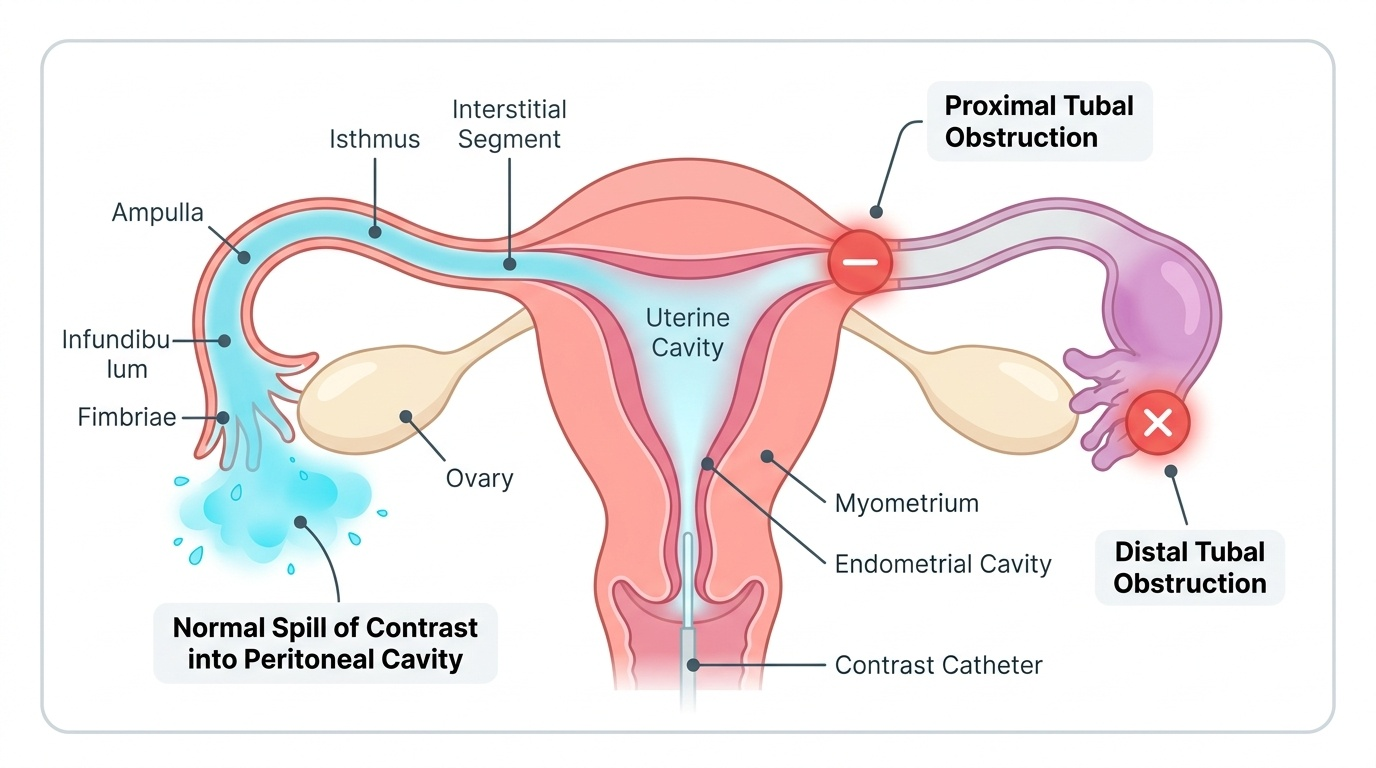
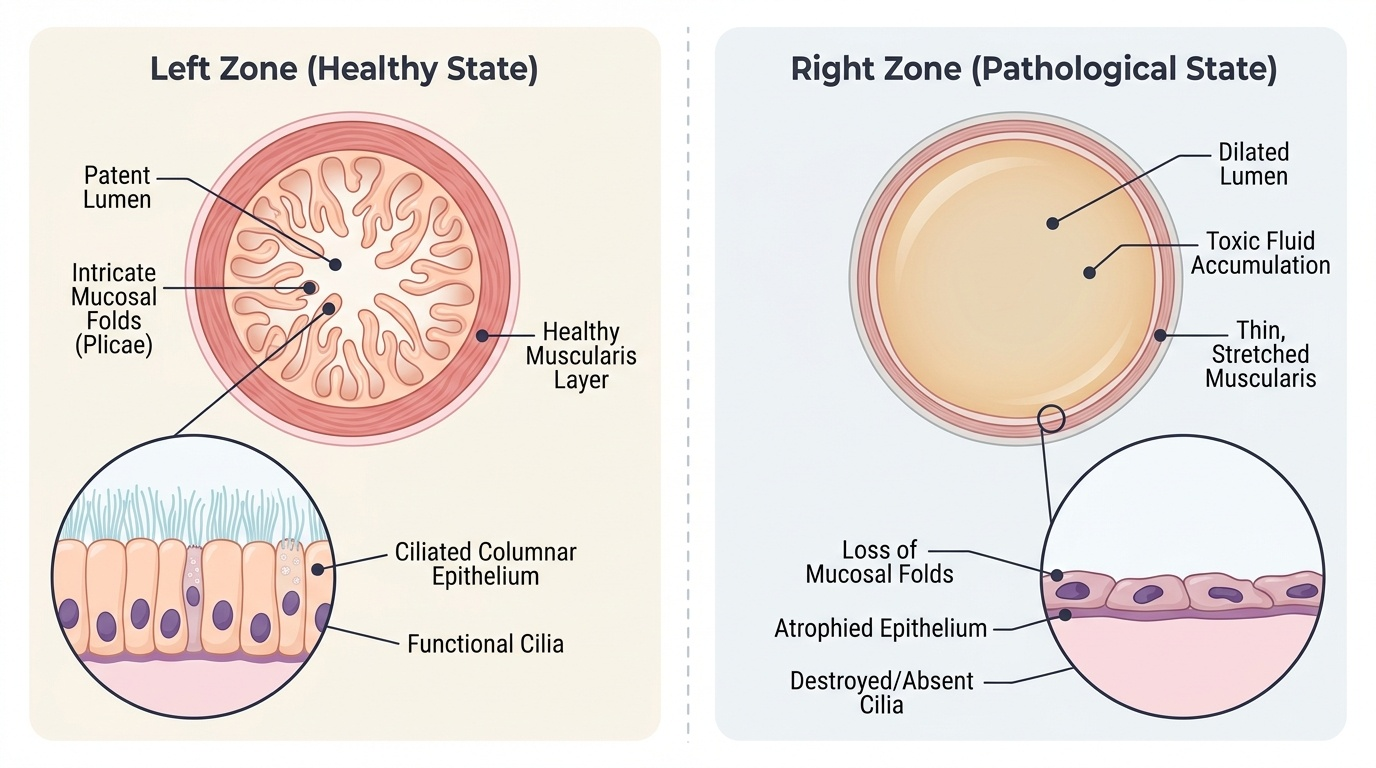
Recall from Anatomy: the fallopian tube has four segments — the intramural (interstitial) segment traversing the uterine wall; the narrow isthmus; the wider ampulla (the usual site of fertilisation); and the infundibulum with its fimbriated end that captures the ovulated oocyte. Tubal obstruction at the proximal (cornual/isthmic) end prevents sperm entry; obstruction at the distal (fimbrial/ampullary) end prevents oocyte pick-up and traps fluid to form a hydrosalpinx. Recall also from Physiology: ciliary transport in the ampulla moves the fertilised egg towards the uterus over 3–4 days; even a 'patent' tube with damaged cilia or abnormal mucosal folds may fail to transport embryos effectively.
Clinical Indication and the Role of Tubal Assessment
Tubal patency assessment is indicated in any woman undergoing investigation for infertility as part of the standard tripartite workup (ovulatory status + semen analysis + tubal patency). It is particularly important — and should be prioritised — in women with a clinical history suggesting increased risk of tubal disease: previous pelvic inflammatory disease (PID), previous ectopic pregnancy, previous pelvic or abdominal surgery (appendicectomy with perforation, ovarian cystectomy, myomectomy), known or suspected endometriosis, or a history of sexually transmitted infection (especially Chlamydia trachomatis). The presence of any of these risk factors raises the pre-test probability of tubal disease substantially, which in turn affects the choice of test and the threshold for proceeding to laparoscopy.
In a woman with no risk factors for tubal disease, ovulatory infertility is more likely and it is reasonable to begin ovulation induction while deferring tubal assessment — but this should not be deferred beyond 3–6 months, since proceeding with ovulation induction cycles while a bilateral tubal block is unrecognised wastes both time and resources.
Chlamydia antibody testing (IgG serology) offers a non-invasive, inexpensive first-line screen for tubal damage from prior chlamydial PID. A positive chlamydia IgG titre correlates with a 3–5-fold increased risk of tubal damage and identifies women who should proceed directly to laparoscopy rather than HSG, as they are likely to have peritubal adhesions not visible on HSG. The NICE fertility guideline recommends that women with a positive chlamydia antibody test should be offered laparoscopy as first-line tubal assessment.
Provided image
Anatomy and Governing Principles of Tubal Patency Testing
All methods of tubal patency assessment share the same fundamental principle: introduce a substance — radio-opaque contrast, saline with microbubble echogenic medium, or coloured dye — into the uterine cavity via the cervix under gentle pressure, and confirm that it flows freely along the length of the fallopian tube and spills into the peritoneal cavity from the fimbriated end. Failure to demonstrate spill at the fimbrial end indicates obstruction at some level between the uterine cornua and the peritoneum. The anatomical segment where obstruction occurs determines the specific pattern seen on the test and has major implications for treatment. The difference between the available modalities lies in how the flow of contrast medium is visualised — fluoroscopic X-ray in HSG, real-time ultrasound in HyCoSy, or direct human vision at laparoscopy — as well as what additional information can be obtained beyond simple patency (uterine cavity morphology, peritubal adhesions, endometriosis deposits, ovarian pathology), the safety and comfort profile for the patient, the requirement for general anaesthesia, and the overall cost and complexity of the investigation.
Key anatomical landmarks in interpreting patency tests:
- The cornual opening (tubal ostium) where the tube enters the uterine cavity is the commonest site of apparent proximal block on HSG — but a significant proportion (~15%) are false positives due to tubal spasm at the cornual junction induced by the contrast injection or cervical cannulation. The smooth muscle of the isthmus is exquisitely sensitive to mechanical and chemical stimulation and can constrict transiently, mimicking true occlusion.
- The ampullary lumen is 1–2 mm wide and tortuous — mucosal adhesions here from salpingitis may impair tubal function even without complete obstruction.
- The fimbrial end traps the oocyte by a combination of ciliary currents and muscular activity — fimbrial agglutination from PID or endometriosis may cause the classic 'clubbed tube' appearance on HSG or laparoscopy.
- A hydrosalpinx is a fluid-filled, distended tube that has lost its fimbrial opening; on HSG it appears as a dilated, contrast-filled tube without spill. Hydrosalpinx fluid contains cytokines and prostaglandins that are embryotoxic, which explains why hydrosalpinx reduces IVF implantation rates by approximately 50%.
Provided image
Procedures and Techniques for Assessing Tubal Patency
Each of the three main modalities serves a distinct role in the clinical assessment ladder, and understanding the technique, findings, and limitations of each is essential for appropriate test selection.
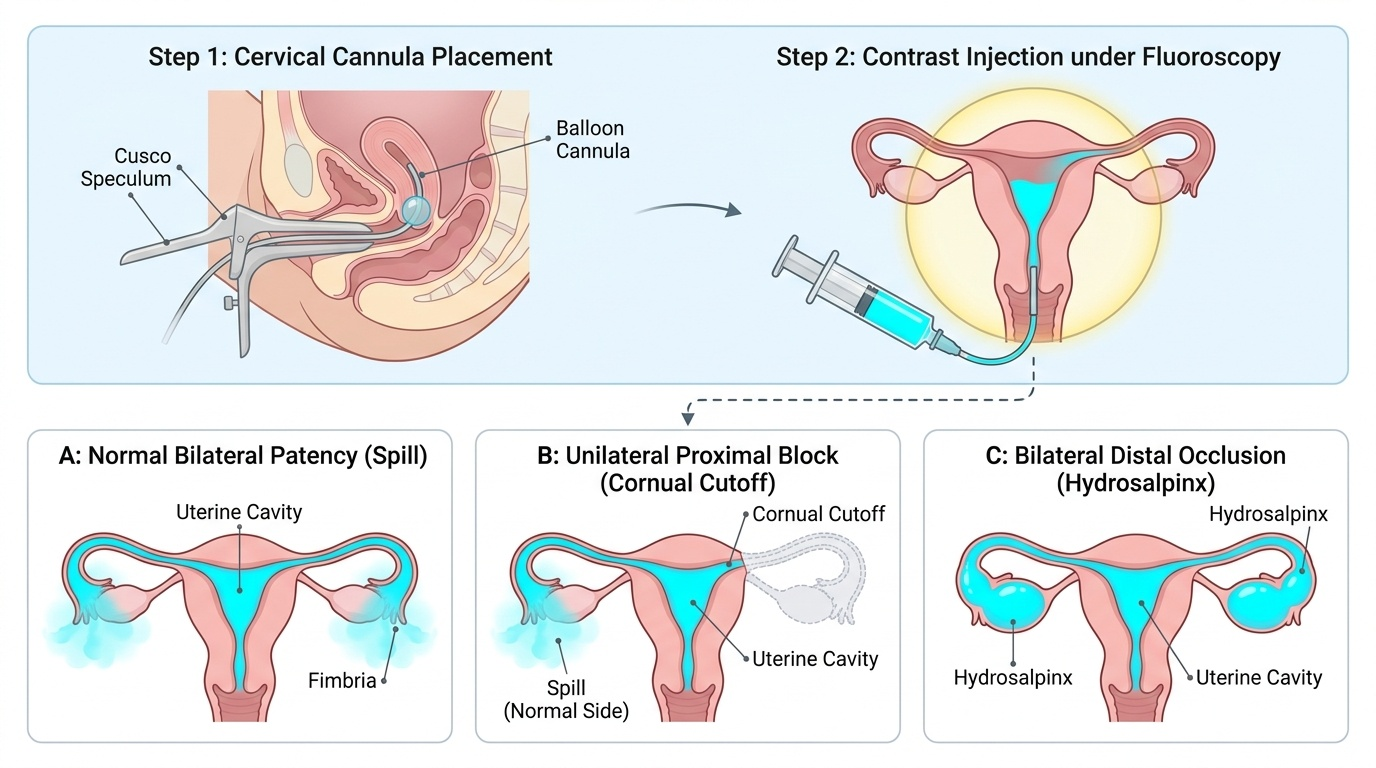
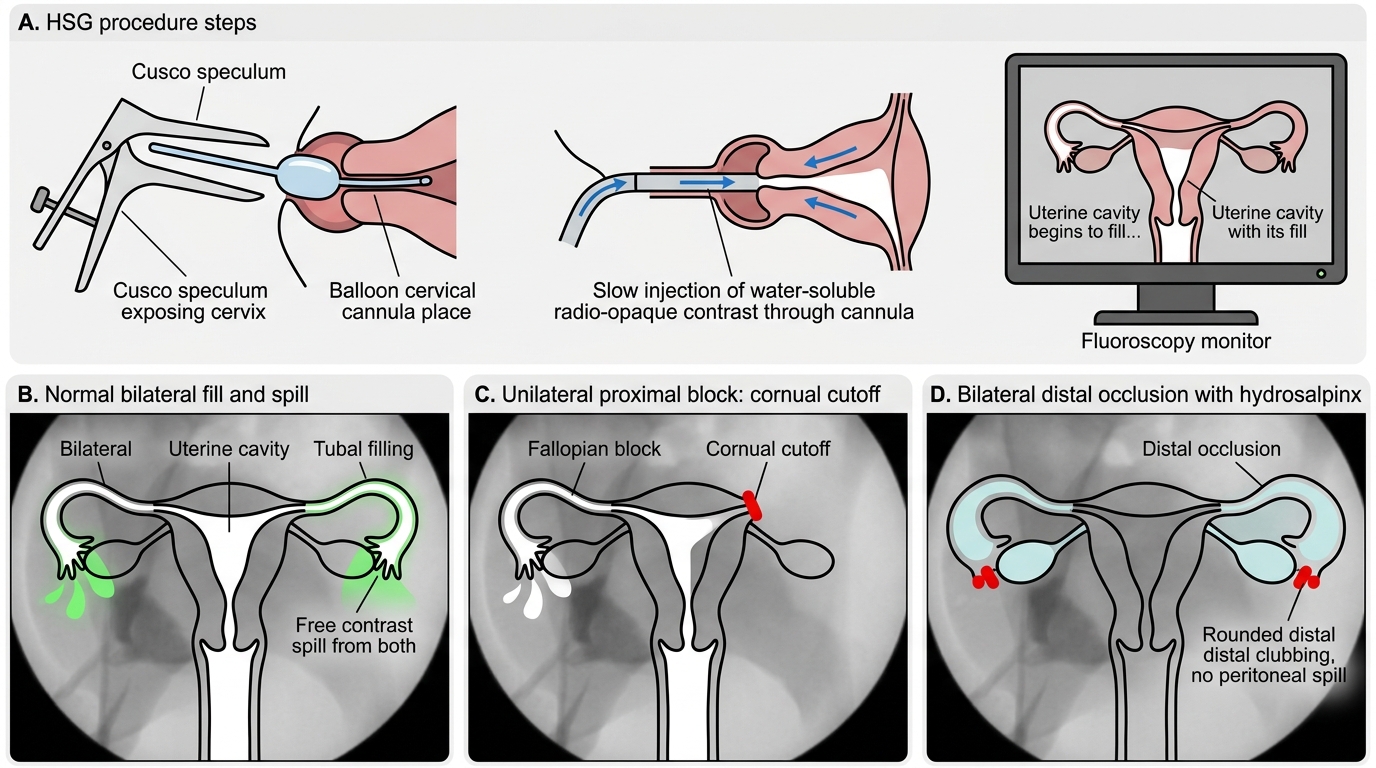
Hysterosalpingography (HSG) is a radiological outpatient procedure performed in the first half of the menstrual cycle (days 7–10), after menstrual flow has ceased but before ovulation. It is contraindicated in active pelvic infection and should be preceded by a chlamydia swab or prophylactic antibiotics (doxycycline 100 mg BD for 5 days, or azithromycin 1 g single dose) in high-risk women. Technique: the cervix is visualised with a Cusco speculum; a Leech-Wilkinson or balloon cannula is inserted into the cervical os; 5–10 mL of water-soluble radio-opaque contrast (e.g. iohexol) is injected slowly under fluoroscopic screening. Normal findings show bilateral filling of the uterine cavity and tubes with contrast spill from both fimbriated ends into the peritoneal cavity. Findings on an abnormal HSG include unilateral or bilateral non-fill (proximal block), dilatation of the tube without spill (hydrosalpinx), or a peritubal loculation. The uterine cavity is also assessed — endometrial polyps, submucous fibroids, and uterine septum produce filling defects or distortion.
Limitations of HSG: false-positive proximal block in ~15% of cases (tubal spasm); it cannot detect peritubal adhesions, endometriosis, or ovarian pathology; radiation exposure (minimal but real); discomfort during the procedure; risk of infection activation in women with silent chlamydia infection.
Saline sonohysterography / HyCoSy (hystero-contrast sonography) uses ultrasound imaging with a small volume of saline or agitated echogenic contrast (ExEm foam) injected via a balloon catheter. It combines assessment of the uterine cavity and tubal patency in one outpatient setting, without radiation. It is particularly useful when a baseline pelvic USS is already being performed as part of the infertility workup. Limitations: operator-dependent; less standardised than HSG; does not provide permanent image documentation; cannot assess mucosal detail.
Diagnostic laparoscopy with chromopertubation (dye test) is the gold standard for tubal patency assessment and provides the most comprehensive evaluation of the pelvis. Technique: performed under general anaesthesia; CO₂ pneumoperitoneum established; a 10 mm laparoscope introduced through the umbilicus; dilute methylene blue (or indigo carmine) dye injected via a uterine manipulator. Direct visualisation confirms dye passage through each tube and spill from the fimbriae. Crucially, laparoscopy simultaneously visualises peritubal adhesions, endometriosis deposits, ovarian cysts, and uterine surface abnormalities — none of which are visible on HSG. Adhesions can be divided and endometriosis deposits treated at the same sitting.
Provided image
Hysterosalpingography: Procedure and Tubal Patency Patterns
SELF-CHECK
A 31-year-old woman with infertility has a positive chlamydia IgG antibody titre on screening. She has no active symptoms. According to current guidelines, which tubal patency assessment should be offered first-line?
A. HSG as the standard first-line tubal test for all infertile women
B. Saline sonohysterography (SSG) as it avoids radiation
C. Diagnostic laparoscopy with chromopertubation
D. Repeat chlamydia IgG in 3 months before any procedure
Reveal Answer
Answer: C. Diagnostic laparoscopy with chromopertubation
NICE recommends that women with positive chlamydia antibody titres should be offered diagnostic laparoscopy as first-line tubal assessment, because the positive serology indicates prior pelvic chlamydial infection and a high probability of peritubal adhesions. HSG misses peritubal adhesions and endometriosis. Delaying further testing is not appropriate in the infertility setting.