Page 16 of 24
OG34.6 | Endometriosis-Adenomyosis Spectrum — SDL Guide
Learning Objectives
- Describe the etiopathogenesis of endometriosis and adenomyosis, including Sampson's retrograde menstruation theory and the adenomyosis endometrial-myometrial disruption model.
- Identify the clinical features distinguishing endometriosis (dysmenorrhoea, dyspareunia, infertility) from adenomyosis (menorrhagia, bulky tender uterus).
- Select and interpret appropriate investigations: transvaginal ultrasound, MRI pelvis, diagnostic laparoscopy, and CA-125.
- Outline medical and surgical management options for both conditions, including fertility-preserving and definitive approaches.
- Explain the implications of endometriosis and adenomyosis on reproductive health and long-term fertility.
INSTRUCTIONS
Endometriosis and adenomyosis are the two most clinically important conditions caused by ectopic endometrial tissue, together accounting for a substantial burden of pelvic pain, dysmenorrhoea, and female infertility. They are frequently encountered in gynaecological outpatient practice and are tested prominently in final MBBS examinations. This module guides you through the clinical presentation, pathological basis, diagnostic approach, and management of both conditions, with an emphasis on the key features that allow a clinician to distinguish them and choose appropriate therapy. A comparison framework is used throughout to solidify understanding of where these two conditions overlap and where they diverge.
References
- DC Dutta's Textbook of Gynecology, 9th ed., Ch. 14 — Endometriosis and Adenomyosis (textbook)
- Shaw's Textbook of Gynaecology, 17th ed., Ch. 21 — Endometriosis (textbook)
- ESHRE Guideline: Management of Women with Endometriosis, 2022 (guideline)
- FOGSI Good Clinical Practice Recommendations: Endometriosis, 2021 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 28-year-old school teacher presents to the gynaecology OPD with a 4-year history of worsening dysmenorrhoea — pain that now begins 3 days before her period and persists throughout, preventing her from attending work for 2 days each cycle. She also reports deep dyspareunia and has been unable to conceive despite 18 months of unprotected intercourse. Her periods are regular, moderate in flow. Pelvic examination reveals mild tenderness in the posterior fornix and restricted mobility of the uterus. Her partner's semen analysis is normal. A 35-year-old multipara, by contrast, presents with heavy, painful periods over the last 2 years and a uniformly enlarged, soft, tender uterus on examination — her cervix is normal and the uterus is smooth, not irregular. These two women exemplify the endometriosis-adenomyosis spectrum: both involve ectopic endometrial tissue, yet differ markedly in location, pathophysiology, dominant symptoms, and management approach.
WHY THIS MATTERS
Endometriosis affects an estimated 10–15% of women of reproductive age worldwide, rising to 30–40% of women investigated for infertility — making it one of the commonest gynaecological causes of subfertility. Adenomyosis affects up to 20–35% of hysterectomy specimens and is a major contributor to menorrhagia in the 35–50-year age group. Both conditions cause significant morbidity: chronic pelvic pain, impaired quality of life, time lost from work, and, for endometriosis, the distress of delayed fertility. Misdiagnosis is common — the average delay from symptom onset to diagnosis of endometriosis is 7–10 years in many countries, partly because dysmenorrhoea is often dismissed as 'normal'. As a final-year student you will encounter these patients in OPD, casualty, and infertility clinics. Competency OG34.6 requires you to describe and discuss etiopathogenesis, clinical features, investigations, fertility implications, and management — all of which this module covers.
RECALL
Before proceeding, refresh your knowledge of the following: (1) Normal endometrial anatomy — the endometrium lines the uterine cavity and comprises a functional (shed during menstruation) and basal layer; during menstruation, blood and endometrial fragments flow out through the cervix but also, via the fallopian tubes, can reflux into the peritoneal cavity. (2) The pelvic anatomy relevant to implantation sites — the Pouch of Douglas (rectouterine pouch, most dependent part of the peritoneal cavity), uterosacral ligaments, ovarian fossae, posterior surface of the uterus, bladder peritoneum, and the broad ligaments. (3) Menstrual cycle regulation — oestrogen in the proliferative phase promotes endometrial growth; progesterone in the secretory phase differentiates it. Oestrogen-dependent stimulation is central to endometriosis pathogenesis. (4) The term 'retrograde menstruation' — the retrograde passage of endometrial cells through the tubes into the peritoneal cavity, which is demonstrable in 70–90% of women with patent tubes but causes disease in only a subset, pointing to additional immune and genetic factors.
Clinical Presentation: When to Suspect the Endometriosis-Adenomyosis Spectrum
Recognising the clinical presentation of endometriosis and adenomyosis is the essential first step, since both are diagnoses that can only be confirmed by imaging or histology but are first suspected on clinical grounds. The two conditions have distinct symptom profiles, though they may co-exist in the same patient.
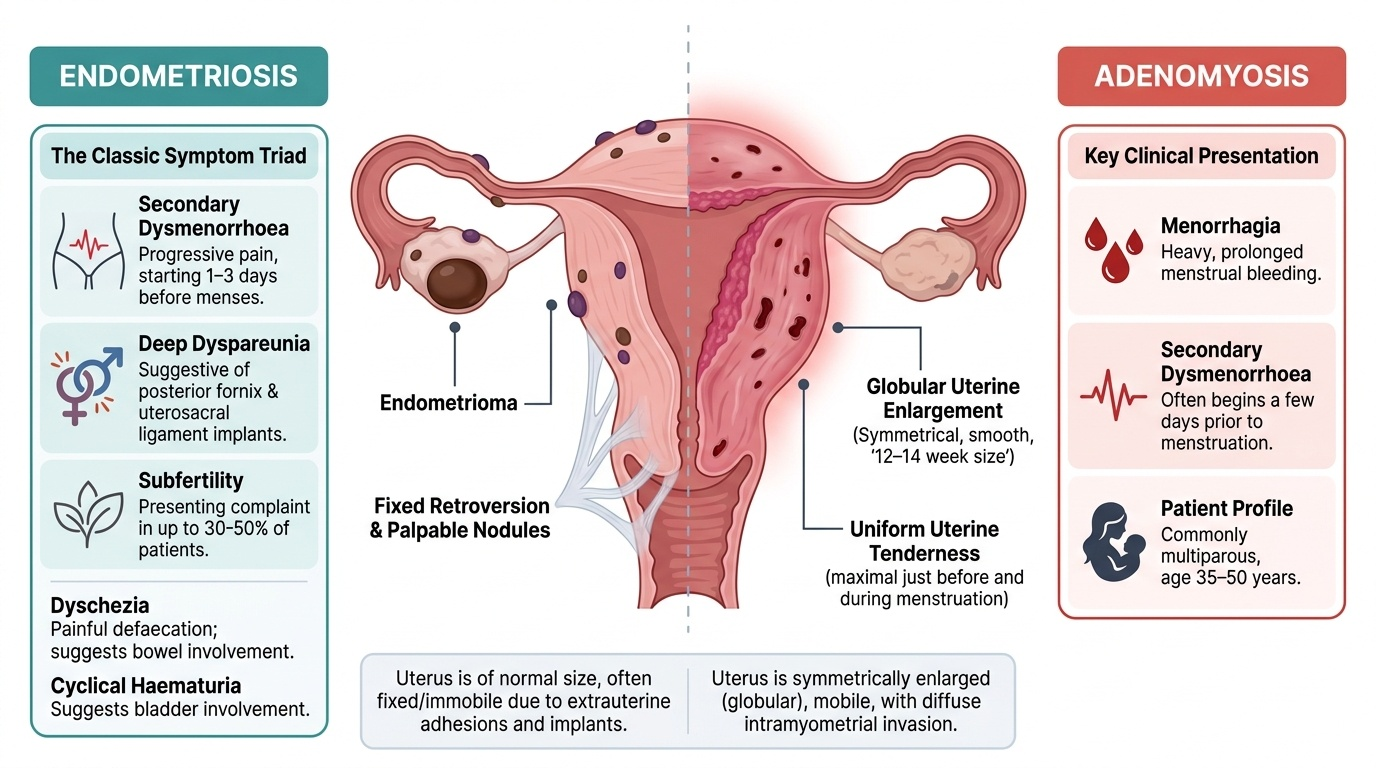
Endometriosis classically presents with the triad of secondary dysmenorrhoea, dyspareunia (deep), and subfertility. The dysmenorrhoea is characteristically secondary — meaning it begins in a patient who previously had painless periods — and progressive (worsening with each cycle). Pain typically starts 1–3 days before the period and continues throughout menstruation; in advanced disease it may become non-cyclical and persist through the cycle. Deep dyspareunia is particularly suggestive of endometriosis involving the posterior fornix, Pouch of Douglas, or uterosacral ligaments. Defaecatory pain during menstruation ('dyschezia') suggests bowel involvement. Cyclical haematuria may indicate bladder endometriosis. The absence of dysmenorrhoea does not exclude endometriosis — some patients present primarily with infertility or a pelvic mass (endometrioma).
On examination, endometriosis may produce fixed retroversion of the uterus (due to adhesions in the Pouch of Douglas), tender nodularity in the posterior fornix or along the uterosacral ligaments (palpable implants), reduced uterine mobility, and occasionally an adnexal mass (endometrioma). Clinical examination can be entirely normal in mild endometriosis.
Adenomyosis presents predominantly with menorrhagia (heavy periods), secondary dysmenorrhoea (often starting a few days before menstruation), and a uniformly enlarged, boggy, tender uterus. The uterine enlargement in adenomyosis is typically symmetrical and smooth (likened to a '12–14 week gravid uterus' in severe cases), in contrast to the irregular, non-tender enlargement of fibroids. The tenderness is characteristic and maximal just before and during menstruation. Dyspareunia may occur but is less prominent than in endometriosis. Many women with adenomyosis are multiparous and in the 35–50-year age group.
A useful clinical distinction: in endometriosis, the uterus may feel fixed (due to adhesions) but is not uniformly enlarged; in adenomyosis, the uterus is uniformly soft and boggy but mobile. The dominant symptom differs: pain dominates in endometriosis; bleeding dominates in adenomyosis.
Provided image
Pathophysiology and Basis of Disease
Understanding the pathophysiology of endometriosis and adenomyosis illuminates why each condition behaves as it does clinically and why management strategies differ.
Endometriosis — pathophysiology. The most widely accepted theory is Sampson's retrograde menstruation theory (1927): during menstruation, viable endometrial cells reflux through the fallopian tubes into the peritoneal cavity, where they implant on peritoneal surfaces, the ovary, and pelvic organs. Evidence supporting this theory includes the demonstration of retrograde menstruation in 70–90% of women with patent tubes (via laparoscopy at the time of menstruation) and the predominance of lesions in the dependent parts of the pelvis (Pouch of Douglas, ovarian fossae). However, retrograde menstruation is nearly universal, yet endometriosis develops in only 10–15% of women, implying that additional factors — immune dysregulation, altered peritoneal macrophage activity, and genetic susceptibility — determine whether implanted cells survive, proliferate, and evade immune clearance.
Alternative theories include coelomic metaplasia (Meyer's theory — multipotential peritoneal cells transform into endometrial-type tissue, explaining rare cases in men and pre-menarchal girls) and lymphovascular dissemination (accounting for distant sites such as the pleura, diaphragm, and umbilicus).
Once implanted, ectopic endometrial tissue responds cyclically to ovarian hormones — it proliferates under oestrogen and bleeds under progesterone withdrawal, just as normal endometrium does. This cyclic bleeding releases prostaglandins, interleukins (IL-1β, IL-6), and vascular endothelial growth factor (VEGF), generating local inflammation, adhesion formation, and ultimately fibrosis. The inflammatory milieu also directly impairs oocyte quality and fertilisation, contributing to infertility. Oestrogen dependence is central: endometriotic implants express aromatase (locally synthesising oestrogen) and show relative progesterone resistance, which both drives lesion persistence and explains why hormonal suppression is the cornerstone of medical therapy.
Adenomyosis — pathophysiology. Adenomyosis occurs when endometrial glands and stroma invade the myometrium, typically beyond 2.5 mm from the basal endometrium (some authorities use 1 field of high-power microscopy as the threshold). The disruption of the endometrial-myometrial junction (EMJ) — a specialised zone of smooth muscle — is central to its pathogenesis. Repeated uterine trauma (multiparity, uterine surgery, curettage) or intrinsic EMJ defects allow endometrial cells to migrate into the myometrium. Once established, the ectopic endometrial islands stimulate surrounding myometrial smooth muscle hyperplasia and hypertrophy, producing the characteristic diffuse enlargement of the uterus. Adenomyosis may be diffuse (scattered throughout the myometrium) or focal (adenomyoma — a localised nodule resembling a fibroid but without a capsule). The cyclic hormonal response of ectopic glands — bleeding within the myometrium with each menstrual cycle — causes intense prostaglandin release and myometrial spasm, producing menorrhagia (increased surface area of functional endometrium) and severe dysmenorrhoea.
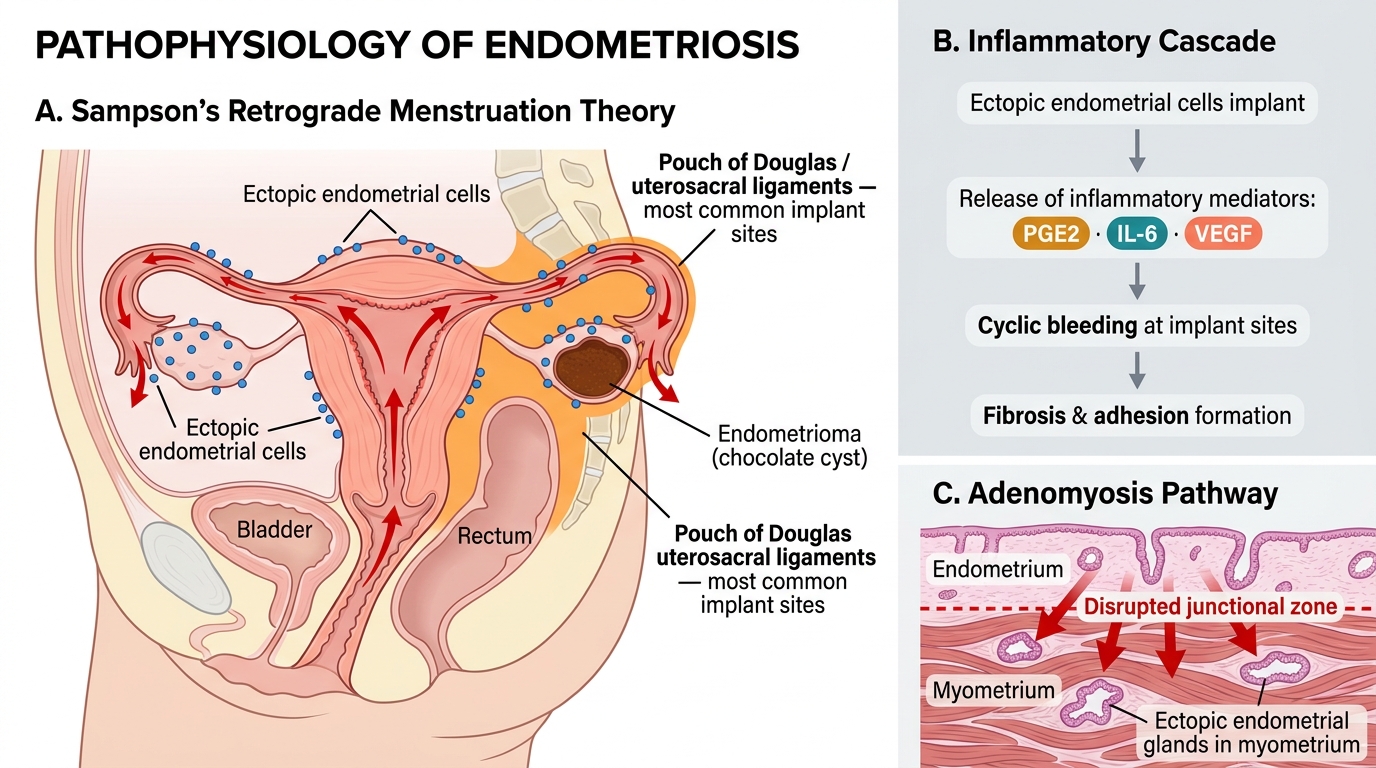
Pathogenesis of Endometriosis and Adenomyosis: Retrograde Theory and Inflammatory Cascade
Sites and Staging of Endometriosis
Endometriosis can implant on virtually any peritoneal surface, but lesion distribution follows a predictable anatomical pattern based on the dependent parts of the pelvis and the proximity to the fallopian tube openings.
The ovary is the most common site (~80% of cases). When endometrial tissue implants on the ovarian cortex and bleeds cyclically, it forms a cystic structure filled with inspissated, dark-brown old blood — the endometrioma (colloquially, 'chocolate cyst'). Endometriomas are typically unilocular or multilocular, have a thick fibrous wall, and are often adherent to the posterior leaf of the broad ligament and surrounding structures. The Pouch of Douglas and uterosacral ligaments are the next most commonly involved sites, producing the nodular, tender posterior fornix characteristic of endometriosis. The rectosigmoid colon (causing dyschezia and, rarely, rectal bleeding), bladder (cyclical haematuria), uterovesical fold, and fallopian tubes are also commonly affected. Rare sites include the umbilicus (Villar's nodule — cyclical swelling and bleeding at the umbilicus), diaphragm, pleura (catamenial pneumothorax — rare but dramatic), and surgical scars.
Deep infiltrating endometriosis (DIE) refers to lesions that penetrate >5 mm below the peritoneal surface; it is associated with the most severe pain, bowel and bladder symptoms, and the greatest surgical complexity.
The revised American Society for Reproductive Medicine (rASRM) staging system is the most widely used classification:
| Stage | Description | Score | Clinical Correlate |
|---|---|---|---|
| I — Minimal | Few superficial implants | 1–5 | May be asymptomatic or mild pain |
| II — Mild | More implants, shallow endometrioma <1 cm, limited adhesions | 6–15 | Pain + early fertility impact |
| III — Moderate | Bilateral endometriomas ≥1 cm, tubal/ovarian adhesions | 16–40 | Significant fertility impairment |
| IV — Severe | Large bilateral endometriomas, dense adhesions, obliterated Pouch of Douglas | >40 | Severe pain, infertility common |
Importantly, rASRM stage does not correlate well with pain severity — a patient with Stage I disease can have excruciating dysmenorrhoea, while a patient with Stage IV may have minimal pain. Stage does correlate (imperfectly) with fertility outcomes and guides surgical planning.
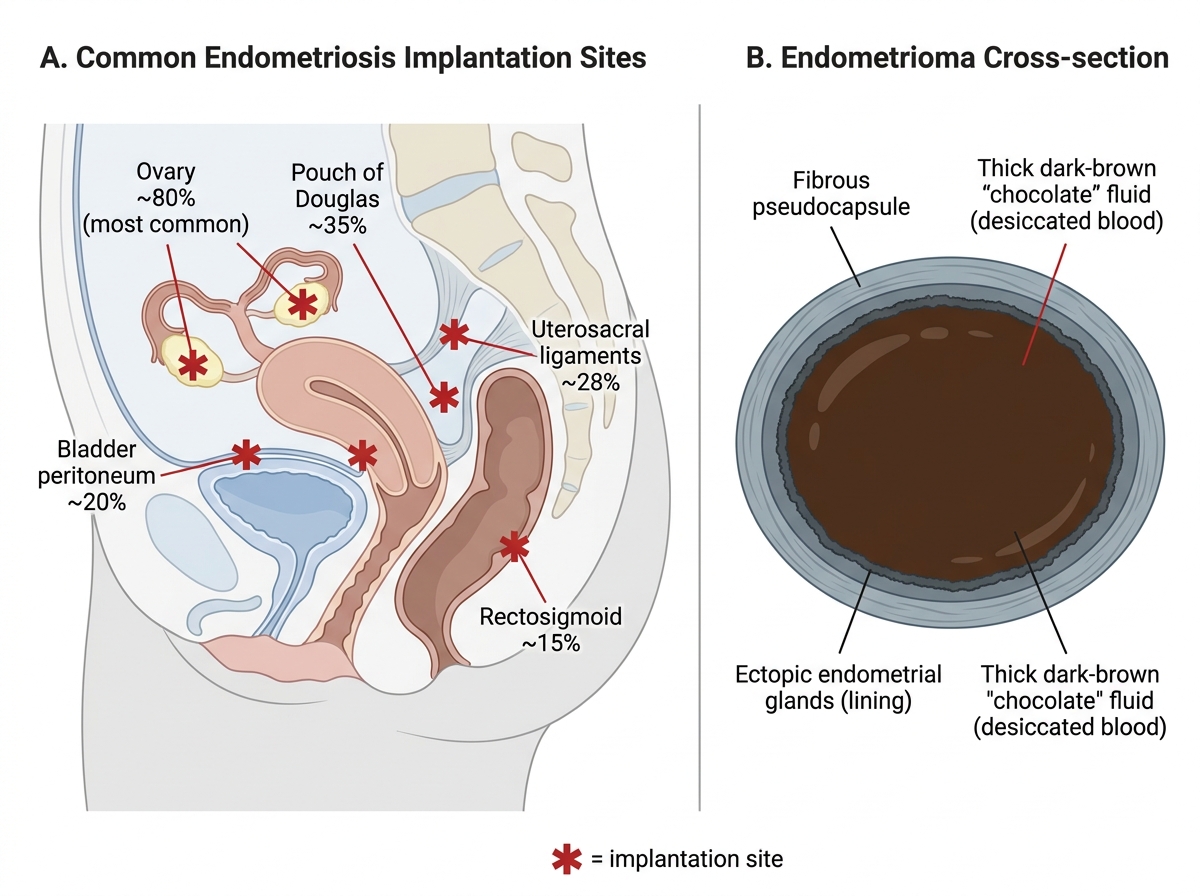
Endometriosis: Pelvic Implantation Sites and Endometrioma Morphology
SELF-CHECK
A 26-year-old woman presents with 3-year history of progressively worsening dysmenorrhoea and 18 months of infertility. Pelvic examination reveals a fixed retroverted uterus with tender nodules in the posterior fornix. Which of the following is the gold standard for definitive diagnosis?
A. Transvaginal ultrasound showing endometrioma
B. Serum CA-125 > 100 IU/mL
C. Diagnostic laparoscopy with histological confirmation
D. MRI pelvis showing deep infiltrating lesions
Reveal Answer
Answer: C. Diagnostic laparoscopy with histological confirmation
Diagnostic laparoscopy with histological confirmation of ectopic endometrial glands and stroma is the gold standard for diagnosing endometriosis. Transvaginal ultrasound is excellent for detecting endometriomas (sensitivity ~90%) but cannot diagnose peritoneal or uterosacral lesions reliably. CA-125 is non-specific and can be elevated in many conditions. MRI is valuable for mapping deep disease but remains an imaging modality — histology provides definitive diagnosis.