Page 3 of 24
OG29.1 | Fibroid Uterus — SDL Guide (Part 3)
Differential Diagnosis
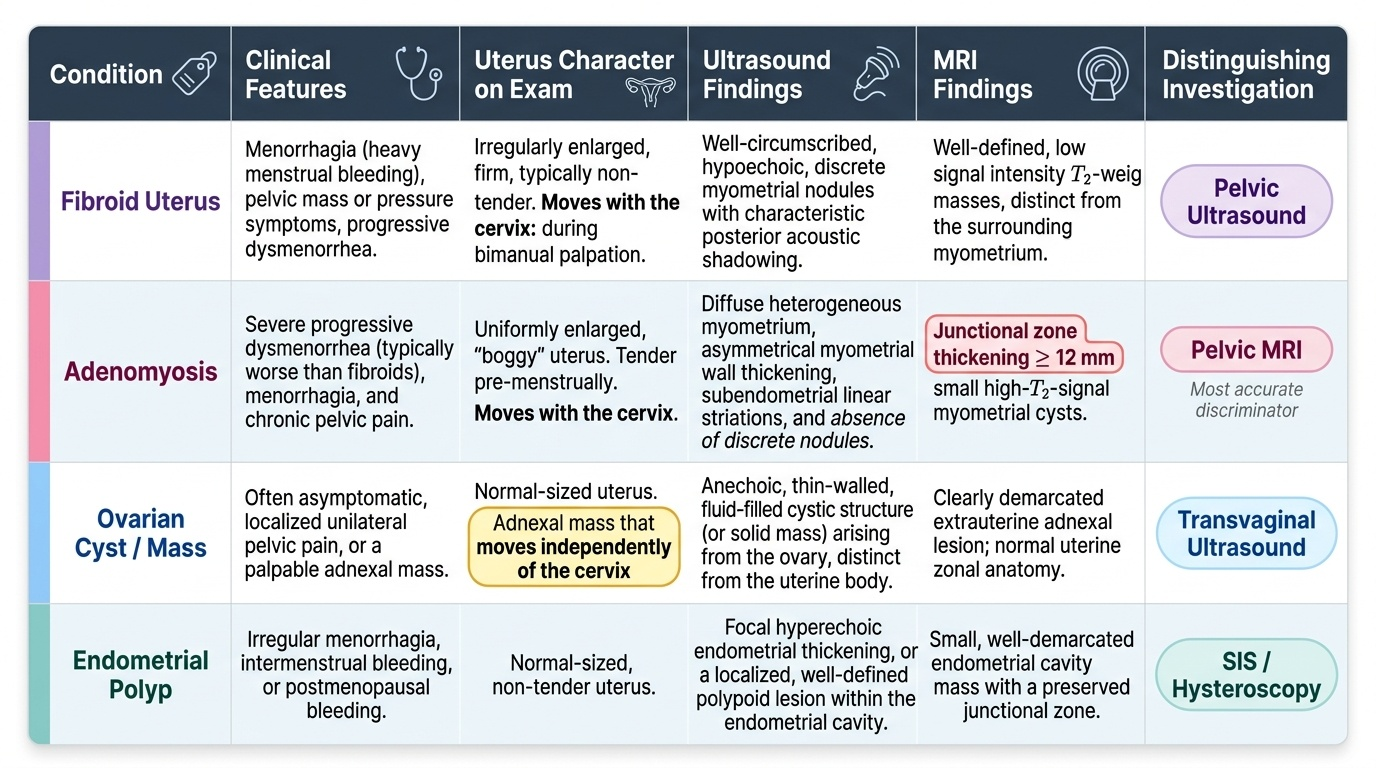
Fibroid uterus must be distinguished from several conditions that produce similar symptoms of menorrhagia, pelvic mass, or uterine enlargement. Accurate differentiation is critical because treatments differ substantially.
Adenomyosis is the most important differential diagnosis. It causes diffuse uterine enlargement, dysmenorrhoea that is typically more severe than in fibroids, and menorrhagia. The uterus is uniformly enlarged (boggy), tender pre-menstrually, and ultrasound shows heterogeneous myometrium without discrete nodules. MRI is the most accurate discriminator, showing junctional zone thickening >12 mm and myometrial cysts. Adenomyosis and fibroids may coexist.
Ovarian tumours — particularly large ovarian cysts or solid ovarian masses — can be confused with a fibroid uterus on clinical examination. The key distinguishing feature is that an ovarian mass moves independently of the cervix on bimanual palpation, whereas a fibroid moves with the uterus. Ultrasound easily differentiates the two. Endometrial polyp causes irregular menorrhagia but produces a smaller endometrial lesion and is diagnosed by SIS or hysteroscopy. Endometrial carcinoma must be excluded in women over 40 with abnormal bleeding — endometrial biopsy is mandatory. Ectopic decidua or pregnancy can simulate a fibroid but the history and serum beta-hCG clarify the diagnosis. Pelvic kidney or a retroperitoneal tumour may be confused with a posterior fibroid in unusual presentations.
Provided image
SELF-CHECK
A 42-year-old woman presents with progressively worsening dysmenorrhoea, menorrhagia, and a uniformly enlarged tender uterus. Ultrasound shows a heterogeneous myometrium with increased vascularity but no discrete nodules. The junctional zone on MRI measures 15 mm. What is the most likely diagnosis?
A. Fibroid uterus
B. Adenomyosis
C. Endometrial carcinoma
D. Ovarian cyst
Reveal Answer
Answer: B. Adenomyosis
Adenomyosis causes diffuse myometrial heterogeneity, a uniformly enlarged and tender (boggy) uterus, and dysmenorrhoea that tends to worsen with age. The MRI junctional zone >12 mm is the diagnostic criterion for adenomyosis. Fibroids produce discrete, hypoechoic nodules; endometrial carcinoma produces endometrial thickening and irregular bleeding; ovarian cysts are separate from the uterus.
Principles of Management
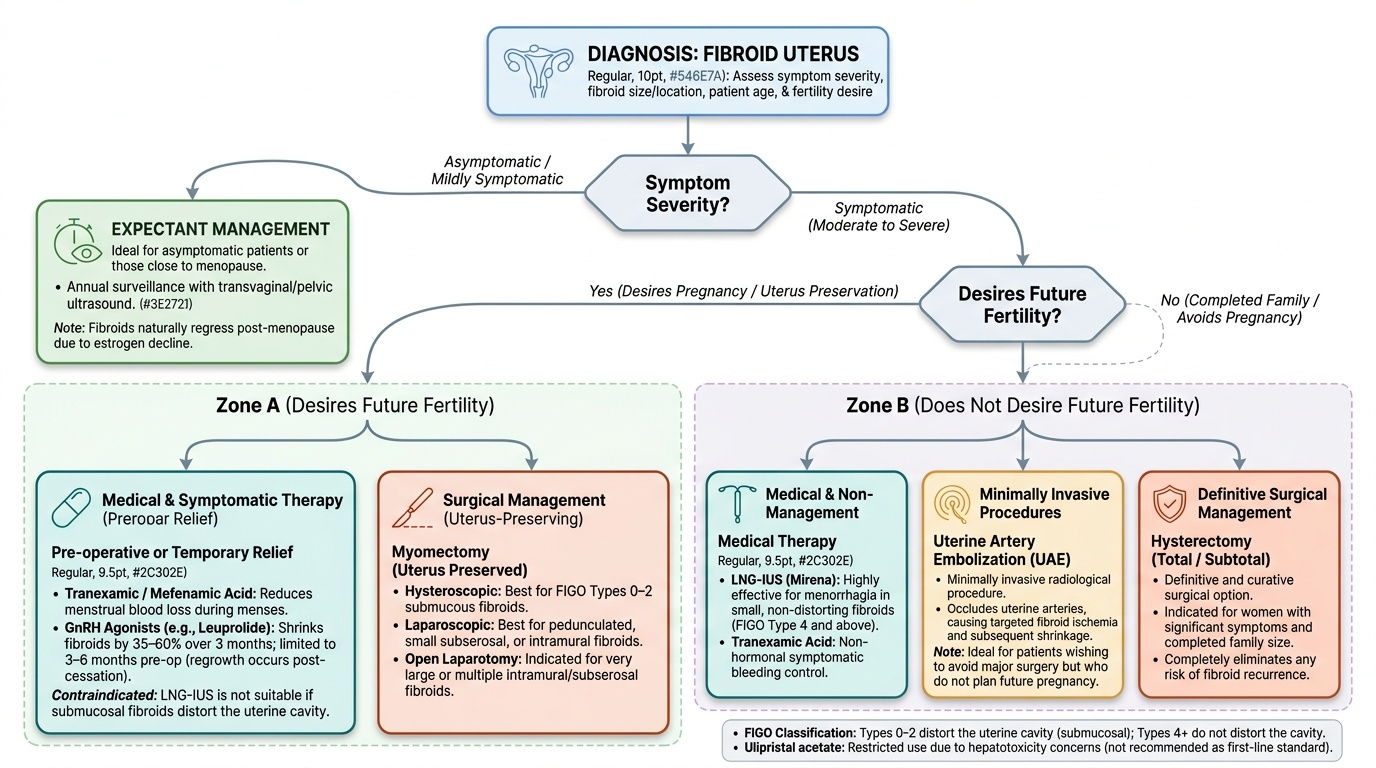
Management of fibroid uterus is individualised based on symptom severity, fibroid size and location, the patient's age, desire for fertility, proximity to menopause, and the patient's preference. The options span expectant (watchful waiting), medical, and surgical approaches.
Expectant management is appropriate for asymptomatic or minimally symptomatic fibroids, particularly in women close to menopause, since fibroids regress spontaneously after menopause due to oestrogen decline. Annual surveillance with ultrasound is advised.
Medical management is used to control symptoms and shrink fibroids preoperatively, but does not permanently cure the condition. GnRH agonists (e.g. leuprolide, goserelin) create a reversible hypoestrogenic state — they reduce fibroid size by 35–60% over 3 months and are used preoperatively to reduce blood loss and facilitate surgery. However, fibroids regrow after cessation, so they are typically limited to 3–6 months preoperatively. Levonorgestrel intrauterine system (LNG-IUS, Mirena) reduces menorrhagia effectively in women with smaller, non-cavity-distorting fibroids (type 4 and above); it is not suitable for submucous types 0–2 that distort the cavity. Tranexamic acid and mefenamic acid reduce menstrual blood loss symptomatically. Ulipristal acetate (selective progesterone receptor modulator) has been shown to reduce fibroid size and control bleeding but its use is now restricted due to concerns about hepatotoxicity.
Surgical management is the definitive treatment. Myomectomy — removal of fibroids while preserving the uterus — is the procedure of choice for women desiring fertility. It can be performed hysteroscopically (for types 0–2), laparoscopically (for pedunculated or small subserosal/intramural fibroids), or by open laparotomy (for large or multiple fibroids). Hysterectomy (total or subtotal) is curative and is appropriate for women with completed family size and significant symptoms; it eliminates all risk of recurrence. Uterine artery embolisation (UAE) is a minimally invasive radiological procedure that occludes the uterine arteries, leading to fibroid ischaemia and shrinkage; it is used in women who wish to avoid surgery but are not planning pregnancy. HIFU (high-intensity focused ultrasound) uses ultrasound energy to ablate fibroid tissue — it is investigational in the Indian context.
Provided image
Indications for surgery include: severe symptomatic anaemia unresponsive to medical therapy, significant pressure symptoms, uterine size equivalent to ≥12 weeks gestation, rapid increase in size, infertility attributable to fibroid, and suspicion of malignancy.
CLINICAL PEARL
Red degeneration (carneous degeneration) of a fibroid in pregnancy: This is the most important degeneration to recognise clinically. It presents in the second trimester with sudden localised uterine pain, low-grade fever, leucocytosis, and a tender uterus at the site of a known fibroid. The management is ALWAYS conservative — bed rest, IV fluids, and analgesics (paracetamol is preferred in pregnancy). Surgery is not indicated and carries high risk of preterm labour. The pain resolves in 4–7 days as the infarct organises. Remember: the distinctive finding is a localised area of exquisite tenderness directly over the fibroid, with a firm consistency on examination — distinguishable from placental abruption (which causes board-like uterine rigidity) and appendicitis (which is in the right iliac fossa).
SELF-CHECK
A 28-year-old primigravida at 18 weeks gestation develops acute lower abdominal pain with localised uterine tenderness over a known 5 cm intramural fibroid. Temperature is 38.1°C and WBC is 14,000/mm³. Fetal heart sounds are normal. What is the most appropriate management?
A. Emergency myomectomy under spinal anaesthesia
B. Conservative management with bed rest, IV fluids, and analgesics
C. Immediate induction of labour to deliver the pregnancy
D. GnRH agonist injection to shrink the fibroid
Reveal Answer
Answer: B. Conservative management with bed rest, IV fluids, and analgesics
This is red (carneous) degeneration of a fibroid in pregnancy. It is managed conservatively with bed rest, IV fluids, and paracetamol for analgesia. Surgery is contraindicated as it risks preterm labour and carries significantly higher intraoperative haemorrhage risk during pregnancy. GnRH agonists are contraindicated in pregnancy. The condition is self-limiting and resolves in 4–7 days.
Self-Assessment
Review the following key points to consolidate your understanding of fibroid uterus. The FIGO classification (0–8) tells you both where the fibroid is and how it should be treated: submucous types (0–2) are hysteroscopic targets; intramural (4) and subserosal (5–7) require laparoscopic or open surgery. Red degeneration in pregnancy is managed conservatively — never surgically. Sarcomatous change is rare but suspected when a postmenopausal woman has a rapidly enlarging uterus. Medical therapy with GnRH agonists shrinks fibroids but does not cure them — it is primarily a preoperative bridge. The choice of myomectomy vs hysterectomy is fundamentally driven by the woman's desire for future fertility. Always exclude endometrial carcinoma with biopsy in women over 40 with abnormal uterine bleeding, even when fibroids are present, as the two can coexist.