Page 9 of 24
OG32.1 | Menopause — SDL Guide
Learning Objectives
- Define menopause, perimenopause, and premature ovarian insufficiency with diagnostic criteria
- Describe the hormonal changes of menopause including FSH rise, oestrogen decline, and loss of inhibin
- Explain the physiological mechanisms underlying vasomotor symptoms, urogenital atrophy, and osteoporosis
- Outline the clinical features of menopause by time of onset (early, medium, long-term)
- Describe the principles, types, benefits, risks, and contraindications of hormone replacement therapy (HRT)
- Enumerate non-hormonal management options and strategies to prevent long-term complications
INSTRUCTIONS
Menopause is the permanent cessation of menstruation resulting from loss of ovarian follicular activity. Every woman who lives into middle age will experience it. As a doctor, you will counsel women about this physiological transition, manage its symptoms, prescribe HRT where appropriate, and prevent its long-term complications — particularly osteoporosis. This module focuses on the physiology, consequences, and evidence-based management of menopause.
References
- DC Dutta's Textbook of Gynaecology, 7th edition, Ch 20 (textbook)
- Shaw's Textbook of Gynaecology, 17th edition, Ch 15 (textbook)
- NICE Guideline NG23: Menopause: diagnosis and management (2015, updated 2019) (guideline)
- WHI Investigators. Risks and Benefits of Estrogen plus Progestin in Healthy Postmenopausal Women. JAMA 2002 (journal)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Mrs Kamala, a 49-year-old accounts officer, consults you with distressing hot flushes 8–10 times a day including at night, difficulty sleeping, and vaginal dryness causing dyspareunia. Her periods have been irregular for the past 18 months and she has not menstruated for 14 months. She is anxious about 'HRT causing cancer' and is asking whether she really needs it. Her FSH is 58 IU/L and oestradiol is 32 pmol/L. How do you explain what is happening hormonally, and how do you counsel her about the safety and appropriateness of HRT?
WHY THIS MATTERS
Menopause is an inevitable physiological transition experienced by all women in the fifth decade of life. The average age of natural menopause in India is approximately 45–47 years — slightly earlier than the global average of 51 years — meaning Indian women may spend a third of their lives in the postmenopausal state. The short-term symptoms (hot flushes, sleep disturbance) are disabling for many women, and the long-term consequences — osteoporosis, urogenital atrophy, and increased cardiovascular risk — carry significant morbidity. A final-year doctor must be able to diagnose menopause confidently, counsel women accurately about HRT risks and benefits based on current evidence (not media fear), prescribe the correct type of HRT, and manage those who cannot or prefer not to use hormones.
RECALL
Recall the hypothalamic-pituitary-ovarian (HPO) axis from physiology: GnRH from the hypothalamus drives FSH and LH release from the anterior pituitary; FSH stimulates ovarian follicle development and oestrogen secretion; oestrogen and inhibin B (from granulosa cells) provide negative feedback to suppress FSH. Recall that oestradiol (E2) is the predominant oestrogen in reproductive women, while oestrone (E1) predominates after menopause. Recall also the role of oestrogen in maintaining bone density by inhibiting osteoclast activity and promoting osteoblast function.
Orientation: What Is Menopause and Why Does It Matter?
Menopause is defined as the permanent cessation of menstruation resulting from loss of ovarian follicular activity, diagnosed retrospectively after 12 consecutive months of amenorrhoea with no other pathological or physiological cause. It is a normal biological event, not a disease, yet its consequences have profound health implications. The perimenopause (climacteric) is the transitional period leading up to the final menstrual period and extending to one year after it — characterised by irregular cycles, fluctuating hormone levels, and the emergence of symptoms. The postmenopause begins after the 12-month amenorrhoea criterion is met.
Premature ovarian insufficiency (POI) is defined as menopause occurring before age 40, affecting approximately 1% of women. POI can be spontaneous (autoimmune, genetic — Turner syndrome, fragile X permutation carriers) or iatrogenic (bilateral oophorectomy, chemotherapy, pelvic radiation). POI carries unique health implications including a significantly increased risk of osteoporosis and cardiovascular disease, and HRT is recommended until at least the natural age of menopause (50 years) in women with POI.
The average age of natural menopause in India is 45–47 years, and globally approximately 51 years. Factors that lower the age of menopause include: smoking, lower socioeconomic status, nulliparity, and certain genetic factors. Factors associated with later menopause include: higher parity and obesity (due to peripheral aromatisation of androgens to oestrone). Surgical menopause (bilateral oophorectomy) causes an abrupt and often more severe menopausal syndrome than natural menopause.
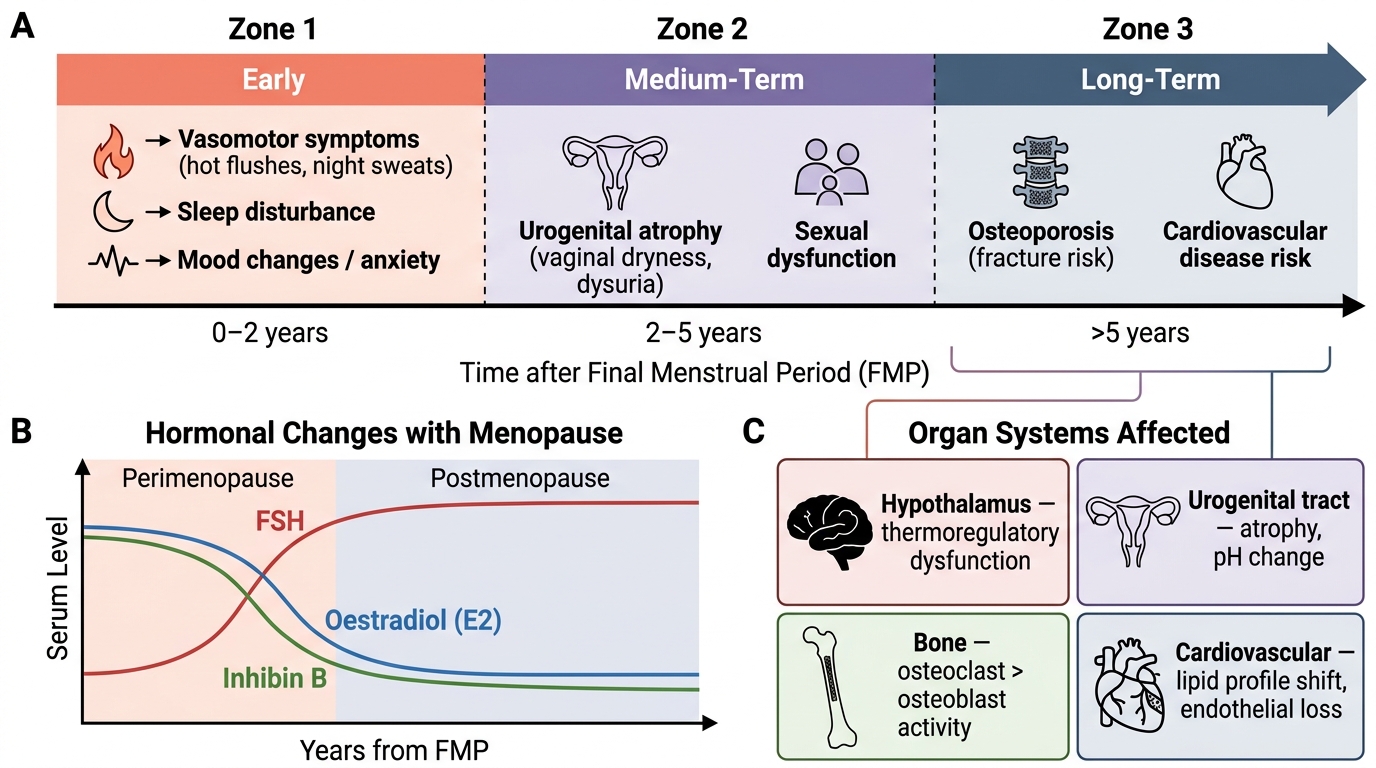
Timeline of Menopausal Symptoms and Organ System Consequences After Final Menstrual Period
Hormonal Changes in Menopause
The hormonal transition of menopause results from progressive depletion of the ovarian follicular reserve, which begins before birth and accelerates markedly in the final decade before menopause. Each woman is born with approximately 1–2 million primordial follicles; by menarche this falls to ~400,000; and by menopause only a few hundred remain, insufficient to mount a follicular response to FSH stimulation.
The key hormonal changes are: (1) Fall in inhibin B — granulosa cells of developing follicles secrete inhibin B, which normally suppresses FSH; as follicles deplete, inhibin B falls first (even before oestrogen declines significantly), causing an early, subtle rise in FSH. This is the earliest biochemical marker of the perimenopause, occurring years before symptoms. (2) Rise in FSH (and LH) — as inhibin B falls, FSH rises progressively, driven by loss of negative feedback. In the postmenopause, FSH typically rises to 40–200 IU/L (compared to 2–15 IU/L in the follicular phase). LH also rises but to a lesser degree. (3) Fall in oestradiol — initially fluctuating (and sometimes paradoxically elevated in the perimenopause as the ovary responds to high FSH with bursts of oestrogen), oestradiol eventually falls to <30 pmol/L in the postmenopause. The predominant postmenopausal oestrogen is oestrone (E1), produced by peripheral conversion of androstenedione (from the adrenal cortex) in adipose tissue. (4) Fall in progesterone — anovulatory cycles in the perimenopause mean progesterone secretion is absent or minimal, leading to unopposed oestrogen effects on the endometrium and irregular, sometimes heavy, bleeding. (5) Anti-Müllerian hormone (AMH) decline — AMH, secreted by small antral follicles, declines progressively from the late reproductive years and approaches zero by menopause; it is the best predictor of ovarian reserve and timing of menopause.
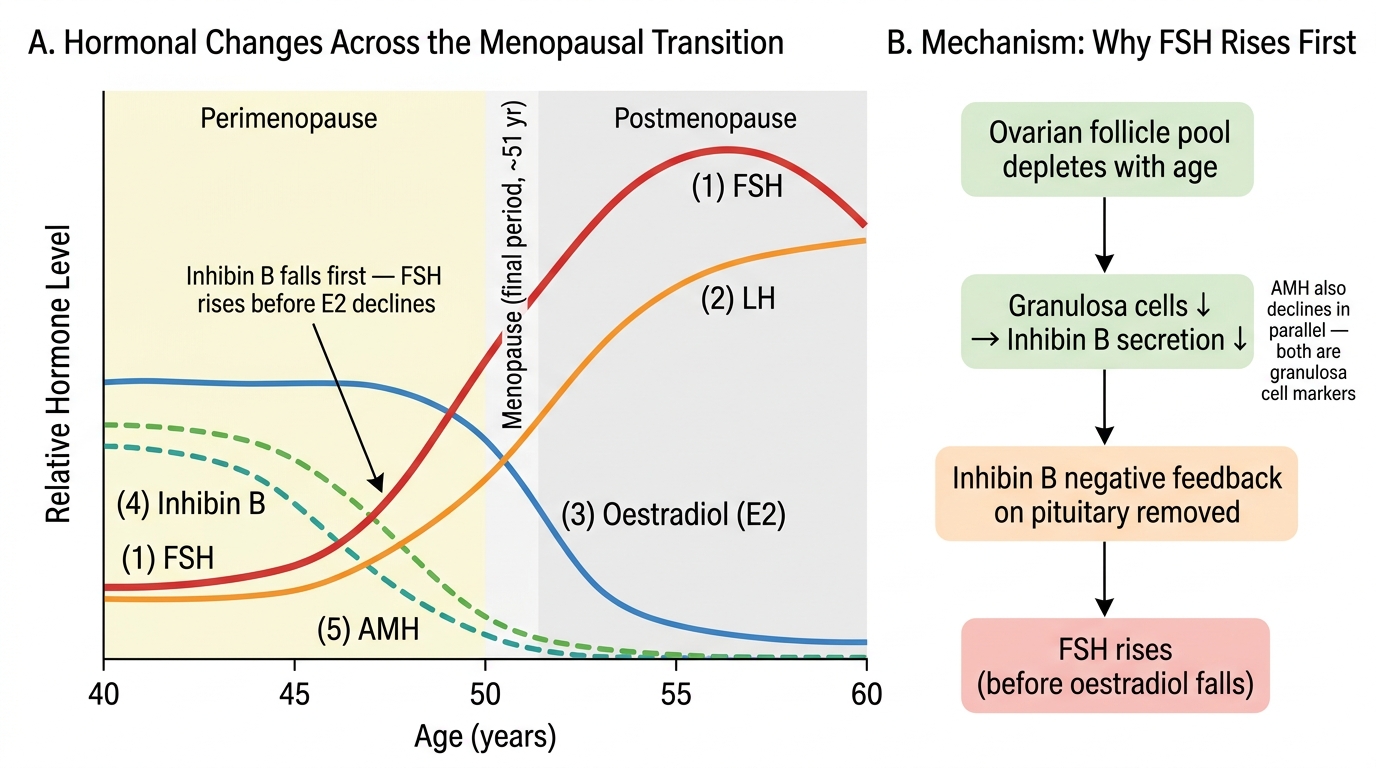
Hormonal Changes Across the Menopausal Transition and the Inhibin B–FSH Mechanism
SELF-CHECK
A 44-year-old woman with irregular periods for 6 months has an FSH of 18 IU/L (elevated for her age) and oestradiol of 180 pmol/L (still normal). Which hormonal change explains the FSH rise BEFORE oestradiol falls?
A. Early rise in LH suppressing oestrogen production
B. Decline in inhibin B from depleting granulosa cells reducing FSH negative feedback
C. Rise in AMH stimulating the pituitary to secrete more FSH
D. Premature luteinisation of follicles increasing androstenedione
Reveal Answer
Answer: B. Decline in inhibin B from depleting granulosa cells reducing FSH negative feedback
Inhibin B is secreted by granulosa cells of developing follicles and is the primary suppressor of FSH secretion. As follicles deplete with advancing age, inhibin B falls first — even before oestradiol declines — removing FSH suppression and causing the earliest measurable perimenopausal change: a rise in FSH. AMH declines in parallel but does not stimulate FSH; LH does not suppress oestrogen; luteinisation produces progesterone not androstenedione in this context.
Mechanisms and Consequences of Oestrogen Deficiency
Oestrogen receptors (ERα and ERβ) are distributed throughout the body — in the hypothalamus, vagina, urethra, bladder, bone, cardiovascular system, skin, and brain — which explains why oestrogen deficiency produces such a wide range of symptoms and long-term consequences.
Vasomotor symptoms (hot flushes and night sweats) — the most characteristic and distressing symptom — arise from disruption of the hypothalamic thermoregulatory centre. Oestrogen normally stabilises the hypothalamic set-point by modulating noradrenergic and serotonergic pathways; its withdrawal narrows the thermoneutral zone (the range of core temperature over which sweating and shivering are not triggered), so minor fluctuations in core temperature trigger disproportionate sweating and flushing. The neurokinin B–kisspeptin–neurokinin B (KNDy) neurones in the arcuate nucleus are activated by oestrogen withdrawal and are the key mediators of hot flushes — a discovery that has led to neurokinin 3 (NK3) receptor antagonists (e.g. fezolinetant) as new non-hormonal treatments.
Urogenital atrophy (genitourinary syndrome of menopause, GSM) results from oestrogen deficiency in the lower urogenital tract. The vaginal epithelium, which is normally thick and glycogen-rich (supporting Lactobacillus and maintaining acid pH), becomes thin, pale, and atrophic. Vaginal pH rises from <4.5 to >5.0, predisposing to dysbiosis and recurrent UTIs. Symptoms include vaginal dryness, dyspareunia, burning, pruritus, urinary frequency, urgency, and dysuria. Unlike vasomotor symptoms, GSM is progressive and does not resolve without treatment.
Bone loss and osteoporosis — oestrogen suppresses osteoclast activity (bone resorption) via RANKL/OPG pathway modulation and promotes osteoblast survival. With oestrogen deficiency, osteoclast activity is unchecked, causing accelerated bone loss — up to 2–5% per year in the first 5 years after menopause. This rapid phase is followed by slower age-related bone loss. The cumulative result is osteoporosis (T-score ≤ −2.5 on DEXA) and a markedly elevated fragility fracture risk — vertebral, hip, and distal radius fractures.
Cardiovascular effects — oestrogen has multiple cardioprotective effects: it raises HDL, lowers LDL, reduces fibrinogen, and has direct vasodilatory effects on the endothelium. Its loss is associated with an unfavourable lipid profile, increased arterial stiffness, and greater cardiovascular disease risk — though the timing of HRT initiation relative to menopause significantly modifies this ('timing hypothesis'). Psychological and cognitive effects include mood disturbance, anxiety, irritability, and difficulty with concentration ('brain fog'); formal dementia risk increases after menopause, though causality with oestrogen deficiency is not fully established.
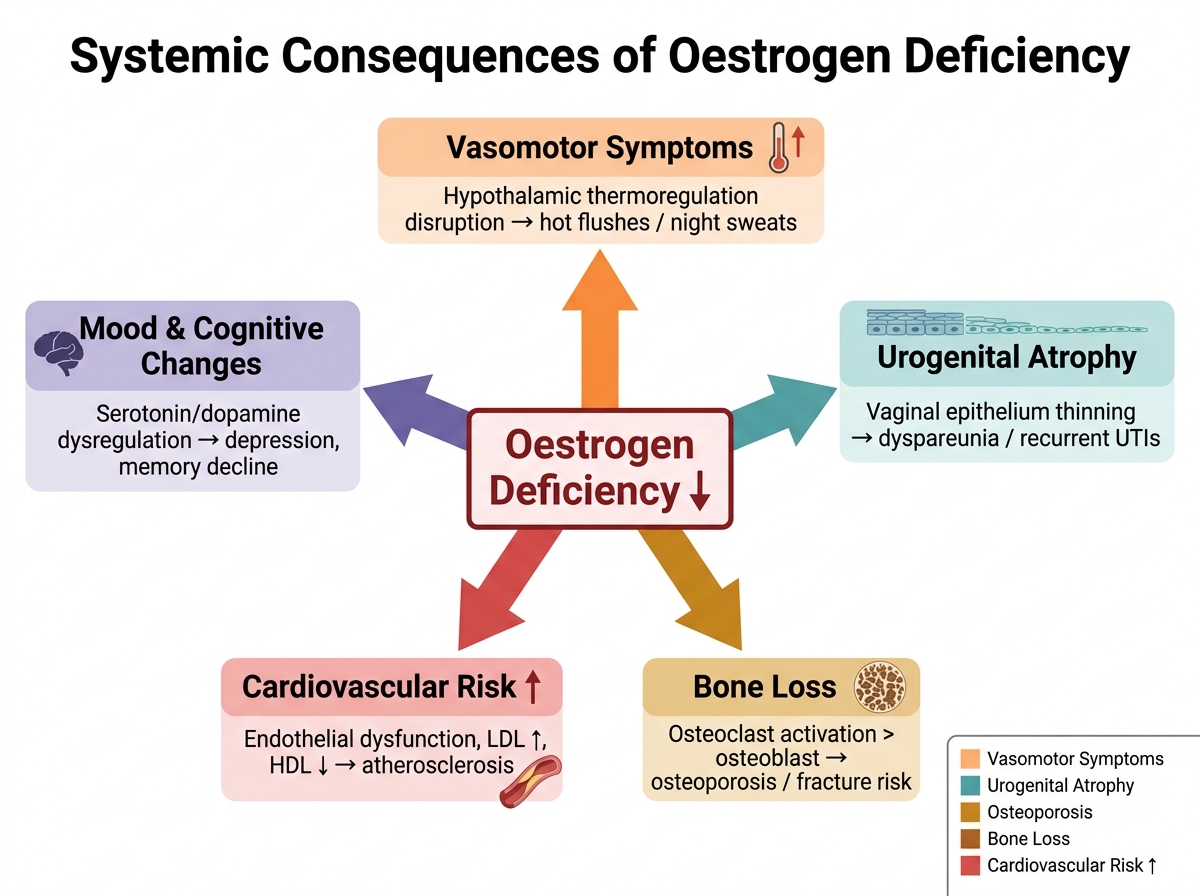
Systemic Consequences of Oestrogen Deficiency