Page 11 of 24
OG32.1 | Menopause — SDL Guide (Part 3)
HRT — Risks, Contraindications, and Duration
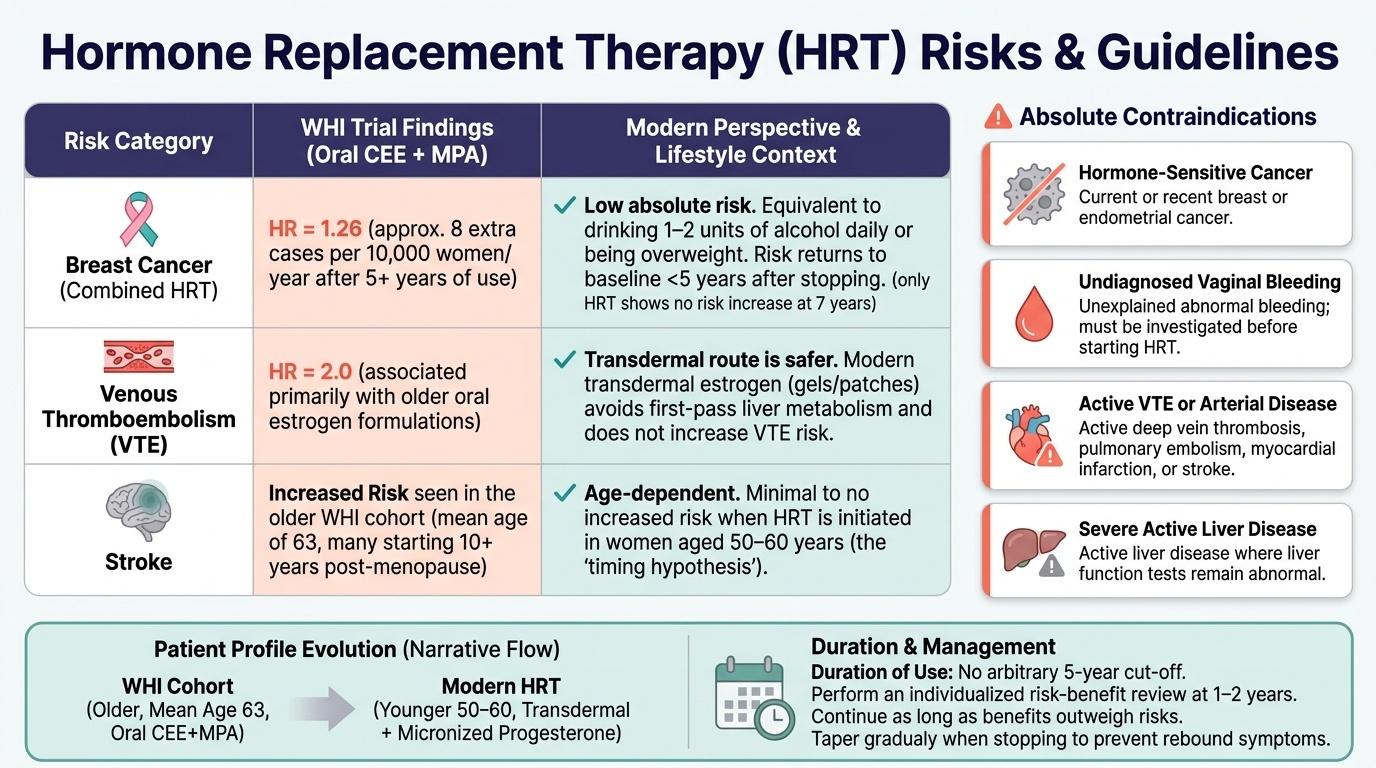
The Women's Health Initiative (WHI) trial, published in 2002, profoundly shaped perceptions of HRT risk. It enrolled postmenopausal women aged 50–79 years and found that combined conjugated equine oestrogen (CEE) + medroxyprogesterone acetate (MPA) after 5+ years was associated with increased risk of breast cancer (hazard ratio 1.26, approximately 8 extra cases per 10,000 women per year), venous thromboembolism (VTE, HR 2.0), and stroke. However, the oestrogen-only arm (in hysterectomised women) showed no increase in breast cancer risk and may even reduce it. Critical re-analysis has clarified that the WHI used an older progestogen (MPA), older women (mean age 63, many starting >10 years after menopause), and oral administration — factors that differ from current practice. Modern HRT using transdermal oestrogen + micronised progesterone in women 50–60 years carries substantially lower risks.
Provided image
Breast cancer risk in context: Current data suggest that combined HRT for 5 years carries a breast cancer risk increase similar to that of drinking one to two units of alcohol daily, or being overweight. The risk returns to baseline within 5 years of stopping HRT. Oestrogen-only HRT (in hysterectomised women) does not increase breast cancer risk at 7 years.
Absolute contraindications to HRT: (1) Current or recent hormone-sensitive cancers (breast, endometrial); (2) Undiagnosed abnormal vaginal bleeding; (3) Active VTE or arterial thromboembolic disease; (4) Severe active liver disease; (5) Known BRCA1/BRCA2 mutation (relative — discuss with specialist). Relative contraindications include: migraine with aura (especially for oral oestrogen — transdermal is safer), severe hypertension (control first), gallbladder disease, hypertriglyceridaemia.
Duration of HRT: There is no absolute time limit for appropriately prescribed HRT. The current NICE guidance recommends a risk-benefit review at 1–2 years but does not impose an arbitrary 5-year cut-off. HRT can be continued as long as benefits outweigh risks after informed discussion. The lowest effective dose should always be used. For women who wish to stop, gradual tapering reduces rebound symptoms.
SELF-CHECK
A 52-year-old woman with an intact uterus has severe hot flushes and vaginal dryness. She asks about HRT. Which formulation is most appropriate?
A. Oestrogen-only oral HRT (conjugated equine oestrogen)
B. Combined transdermal oestradiol patch with oral micronised progesterone
C. Vaginal oestrogen cream only
D. Tibolone (synthetic steroid with oestrogenic, progestogenic, and androgenic activity)
Reveal Answer
Answer: B. Combined transdermal oestradiol patch with oral micronised progesterone
A woman with an intact uterus requires combined HRT (oestrogen + progestogen) to protect the endometrium from unopposed oestrogen-induced hyperplasia. Transdermal oestradiol avoids first-pass hepatic metabolism and has a lower VTE risk than oral oestrogen. Micronised progesterone has a more favourable safety profile than synthetic progestogens. Oestrogen-only is inappropriate in a woman with a uterus. Vaginal oestrogen alone treats GSM but not systemic vasomotor symptoms. Tibolone is an alternative but is best used in established postmenopause and carries specific cancer considerations.
Non-Hormonal Management and Prevention of Long-Term Complications
Non-hormonal management is important for women who cannot or choose not to use HRT — particularly those with a history of hormone-sensitive breast cancer, active VTE, or personal preference.
Vasomotor symptoms: SSRIs (e.g. escitalopram, paroxetine) and SNRIs (venlafaxine, desvenlafaxine) reduce hot flush frequency by 50–60% through serotonergic and noradrenergic modulation of the hypothalamic thermoregulatory centre — they are the most effective non-hormonal option. Clonidine (central alpha-2 agonist) reduces flush frequency modestly. Gabapentin and pregabalin are also effective, particularly for night sweats. Fezolinetant (neurokinin 3 receptor antagonist, targeting KNDy neurones) is a new non-hormonal licensed option for vasomotor symptoms. Cognitive-behavioural therapy (CBT) and mindfulness significantly reduce the distress associated with hot flushes, even when they do not reduce frequency. Lifestyle measures: regular aerobic exercise, maintaining a healthy weight, avoiding triggers (caffeine, alcohol, spicy food, hot drinks).
Urogenital atrophy (GSM): Vaginal lubricants and moisturisers (replens, KY Jelly) alleviate dryness and dyspareunia without hormonal effect. Topical/local oestrogen (creams, pessaries, ring) is extremely effective and minimally absorbed systemically — it can safely be used long-term and even in most breast cancer survivors (with oncologist guidance). Ospemifene (selective oestrogen receptor modulator, oral) is a non-oestrogen option for dyspareunia.
Prevention of osteoporosis: Calcium (dietary target 1000–1200 mg/day; supplement if dietary intake insufficient) and Vitamin D (800–2000 IU/day; check 25-OH Vitamin D level). Weight-bearing and resistance exercise — walking, dancing, strength training — stimulates bone formation. Bisphosphonates (alendronate 70 mg weekly, risedronate, zoledronic acid) are the first-line pharmacological treatment for osteoporosis (T-score ≤ −2.5 or fragility fracture) — they inhibit osteoclast activity and increase bone mineral density. DEXA monitoring every 2–5 years for women on bisphosphonates or with POI.
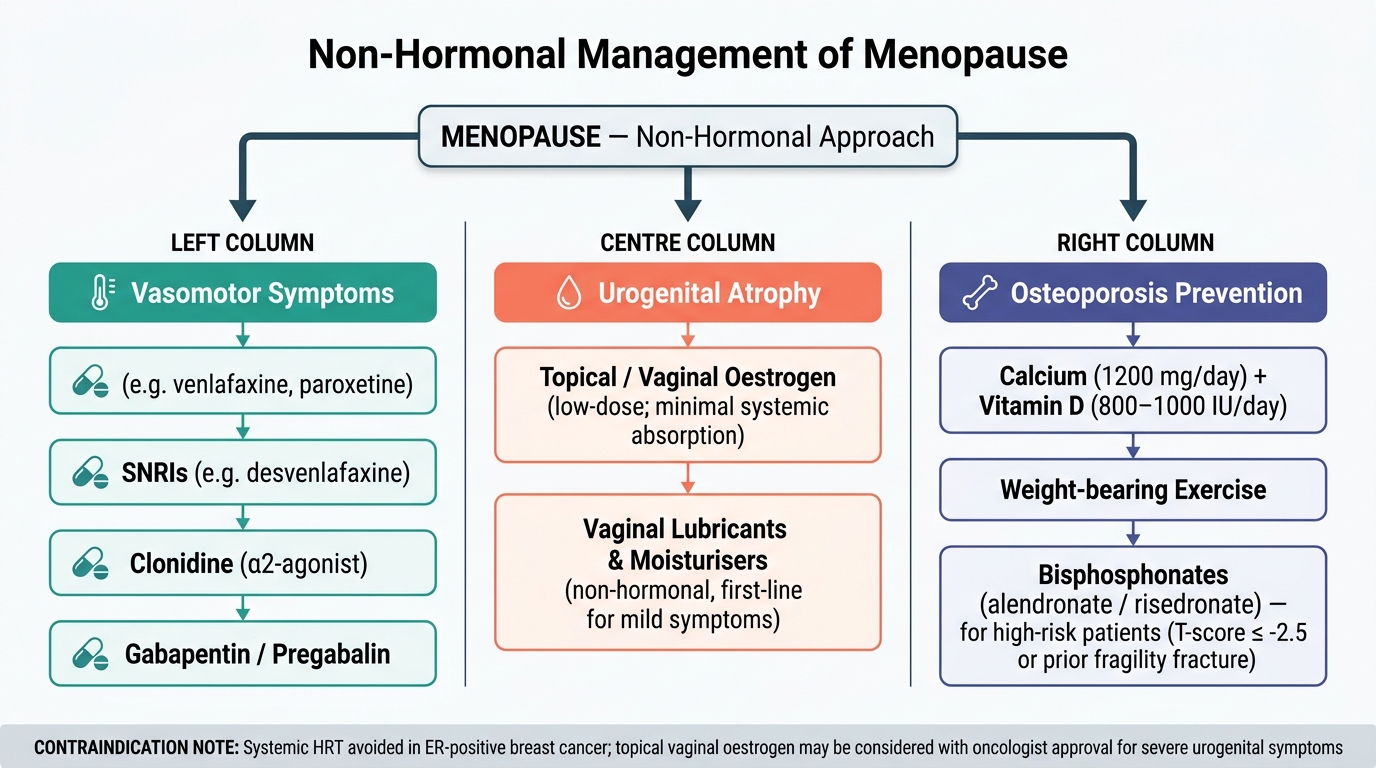
Algorithm: Non-Hormonal Management of Menopausal Symptoms
CLINICAL PEARL
The 'timing hypothesis' for HRT and cardiovascular protection: HRT started within 10 years of menopause onset or before age 60 ('early window') appears to reduce cardiovascular disease risk, whereas HRT started more than 10 years after menopause (as in the WHI trial's average participant, who was 63 years old) may increase it. The proposed mechanism is that oestrogen protects healthy, pliable endothelium but accelerates atherosclerosis once plaques have already formed. This explains why younger symptomatic perimenopausal women should not be denied HRT on cardiovascular grounds, while HRT initiation is not recommended in asymptomatic older women for primary cardiovascular prevention. For your exams: state that HRT is cardioprotective when initiated early, but the WHI tested it in older women with established cardiovascular risk and found harm — the two findings are not contradictory.
SELF-CHECK
A 56-year-old woman 5 years post-mastectomy for ER-positive breast cancer has severe vaginal dryness and dyspareunia but no hot flushes. Systemic HRT is contraindicated. What is the safest treatment for her urogenital symptoms?
A. Oral oestrogen (oestrone sulphate)
B. Transdermal oestradiol patch
C. Topical vaginal oestrogen (low-dose cream or pessary)
D. Tibolone
Reveal Answer
Answer: C. Topical vaginal oestrogen (low-dose cream or pessary)
For urogenital symptoms (GSM) in a breast cancer survivor, topical vaginal oestrogen at low doses is considered safe by most oncology guidelines because systemic absorption is minimal — blood oestradiol levels remain within the postmenopausal range. Major oncology bodies (ASCO, ESMO) permit its use with oncologist discussion. Systemic HRT (oral, transdermal, tibolone) is contraindicated in ER-positive breast cancer. Vaginal lubricants are an alternative first step but less effective for established atrophy.
Self-Assessment
Consolidate the following key concepts. Menopause is diagnosed after 12 consecutive months of amenorrhoea; perimenopause precedes it with irregular cycles and fluctuating hormones. The first hormonal change is the fall in inhibin B (not oestrogen), causing early FSH rise — a sensitive perimenopausal marker. FSH >30–40 IU/L on two occasions confirms ovarian failure; it is not routinely needed for natural menopause in women 45–55 years. Vasomotor symptoms arise from oestrogen withdrawal destabilising the hypothalamic KNDy neurones. Urogenital atrophy (GSM) does not regress spontaneously — it requires local oestrogen or lubricants. HRT is the most effective treatment: combined (oestrogen + progestogen) for women with a uterus, oestrogen-only after hysterectomy. Transdermal route is preferred (lower VTE risk, no first-pass effect). Micronised progesterone is preferred over synthetic progestogens. Absolute contraindications include hormone-sensitive cancer, undiagnosed vaginal bleeding, active VTE, and severe liver disease. The WHI data apply to older women (mean age 63) using oral CEE + MPA — not to modern transdermal HRT in peri- or early postmenopausal women. For women who cannot use HRT: SSRIs/SNRIs for vasomotor, topical oestrogen for GSM (generally safe even in breast cancer survivors), and bisphosphonates + calcium/Vit D for osteoporosis. POI requires HRT until age 50 regardless of contraceptive status.