Page 5 of 24
OG31.1 | Uterine Prolapse — SDL Guide
Learning Objectives
- Describe the aetiology, classification, and pathophysiology of uterine prolapse
- Classify prolapse using the POP-Q staging system and the traditional grading system
- Outline the clinical features, diagnosis, and investigations of uterine prolapse
- Describe the principles of conservative (pessary) and surgical management
- Enumerate preventive strategies for uterine prolapse
INSTRUCTIONS
Uterine prolapse is a form of pelvic organ prolapse (POP) in which the uterus descends into or beyond the vaginal canal due to failure of pelvic floor support. It predominantly affects multiparous women and is a major cause of morbidity and surgical intervention in India. This module covers the internationally standardised POP-Q classification, the full range of management from pessaries to definitive surgery, and the critically important preventive measures.
References
- DC Dutta's Textbook of Gynaecology, 7th edition, Ch 19 (textbook)
- Shaw's Textbook of Gynaecology, 17th edition, Ch 14 (textbook)
- ICS POP-Q Standardisation Committee — POP-Q System (Bump et al., 1996) (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Radha, a 52-year-old farmer and mother of four, comes to the outpatient clinic with a 'something coming out' of her vagina for the past three years, which worsens on standing and is temporarily relieved by lying down. She also has difficulty initiating micturition and a dragging sensation in her lower abdomen. On examination, when she is asked to strain, the cervix appears at the introitus and the anterior vaginal wall bulges prominently. What structure has failed, how do you grade this prolapse, and what are her options — from a ring pessary to surgery?
WHY THIS MATTERS
Uterine prolapse is one of the most common gynaecological conditions in rural India, where high parity, early marriage, poor nutrition, and heavy manual labour combine to overwhelm pelvic floor support. It is the third most common indication for hysterectomy worldwide. Beyond its physical impact, prolapse profoundly affects quality of life — bowel, bladder, and sexual function are all impaired. As a final-year student you will encounter prolapse in outpatient clinics and surgical wards; you must be able to stage it accurately, counsel women about conservative options, and understand when surgery is indicated and which procedure to choose.
RECALL
From your earlier anatomy, recall the three levels of pelvic support described by DeLancey: Level I (uterosacral and cardinal ligaments suspending the uterus and upper vagina), Level II (lateral attachments of the mid-vagina to the arcus tendineus fasciae pelvis), and Level III (perineal body and perineal membrane supporting the lower vagina). Recall the levator ani muscle group (pubococcygeus, iliococcygeus, puborectalis) forming the pelvic diaphragm, and that the cardinal (Mackenrodt's) ligaments are the primary uterine support at the level of the isthmus.
Clinical Presentation of Uterine Prolapse
Uterine prolapse presents with a constellation of symptoms that reflect the descent of the uterus and the associated defects of the anterior and posterior vaginal walls. The hallmark complaint is a sensation of something coming down or a bulge at the vaginal introitus, which worsens on prolonged standing, straining, coughing, or lifting heavy loads, and is temporarily relieved by lying supine. Women often report a dragging or heaviness in the lower abdomen and perineum, particularly towards the end of the day.
Associated bladder symptoms arise from the cystocele (anterior wall descent): stress urinary incontinence (leakage on coughing/sneezing), frequency, urgency, incomplete bladder emptying, difficulty initiating micturition, and — in advanced prolapse — urinary retention requiring the patient to manually reduce the prolapse to void. Bowel symptoms from rectocele (posterior wall descent) include constipation, incomplete evacuation, and the need to digitally reduce the posterior wall to complete defaecation. Sexual dysfunction — dyspareunia and reduced sensation — is common. In the most advanced cases, the prolapsed uterus may ulcerate at the cervix due to chronic friction, causing discharge, bleeding, or secondary infection. Symptoms are invariably worse in multiparous, postmenopausal, and physically active women.
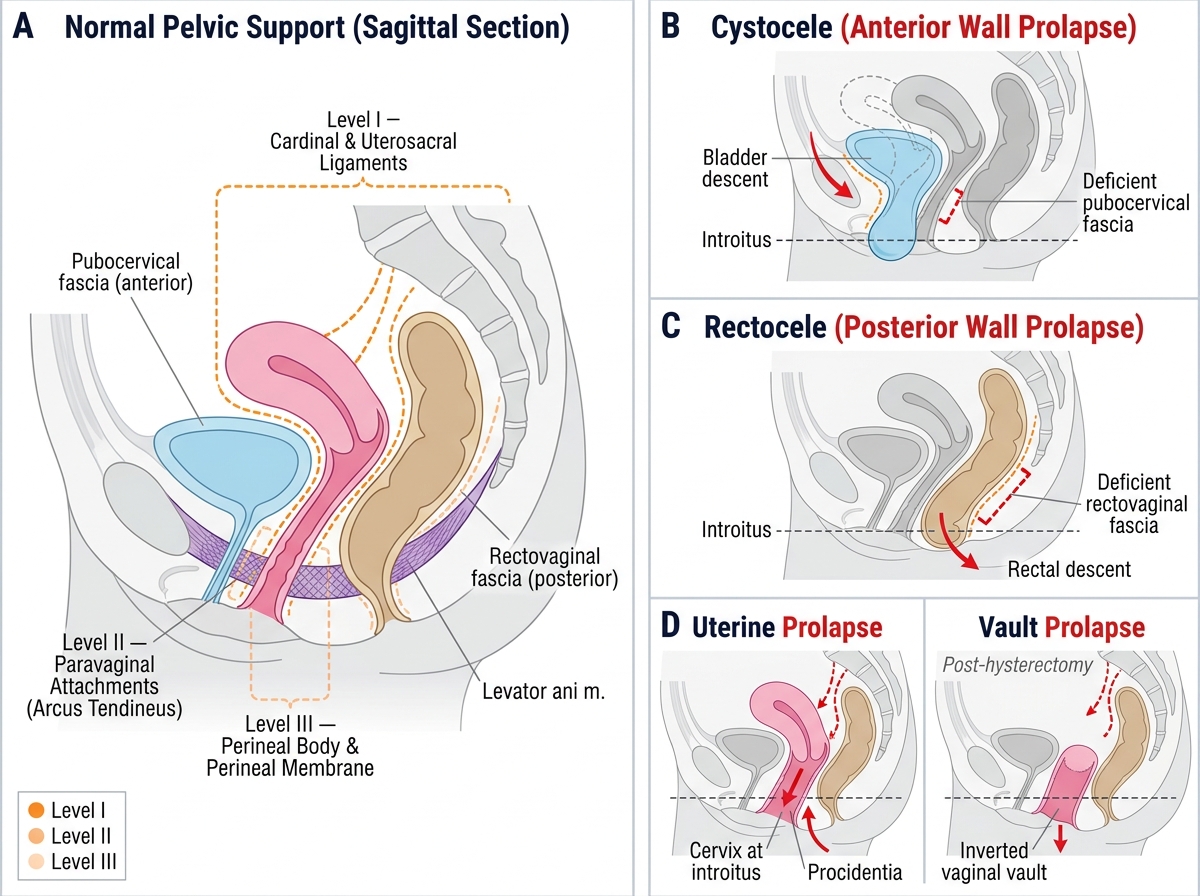
Types of Pelvic Organ Prolapse — Sagittal Anatomical Views with DeLancey Support Levels
Anatomy of Pelvic Floor Support and Aetiology
The uterus is maintained in its normal anteverted, anteflexed position by an integrated system of ligaments, fascial condensations, and muscles. DeLancey's three levels of support provide a useful anatomical framework: Level I support (apical) is provided by the cardinal (Mackenrodt's) ligaments and uterosacral ligaments, which suspend the cervix and upper vagina from the lateral pelvic sidewall and sacrum — damage here leads to uterine descent and vault prolapse. Level II support (lateral) consists of the paravaginal attachments of the mid-vaginal walls to the arcus tendineus fasciae pelvis — damage leads to cystocele and rectocele. Level III support (distal) is provided by the perineal body, perineal membrane, and external anal sphincter — damage leads to perineal descent and gaping introitus.
The levator ani muscle (comprising pubococcygeus, iliococcygeus, and puborectalis) forms the muscular floor of the pelvis and maintains the vaginal axis; its denervation or tearing during childbirth is a key contributor to prolapse. The pubocervical fascia (anterior) and rectovaginal fascia (Denonvilliers' fascia, posterior) are the connective tissue layers whose integrity prevents cystocele and rectocele respectively.
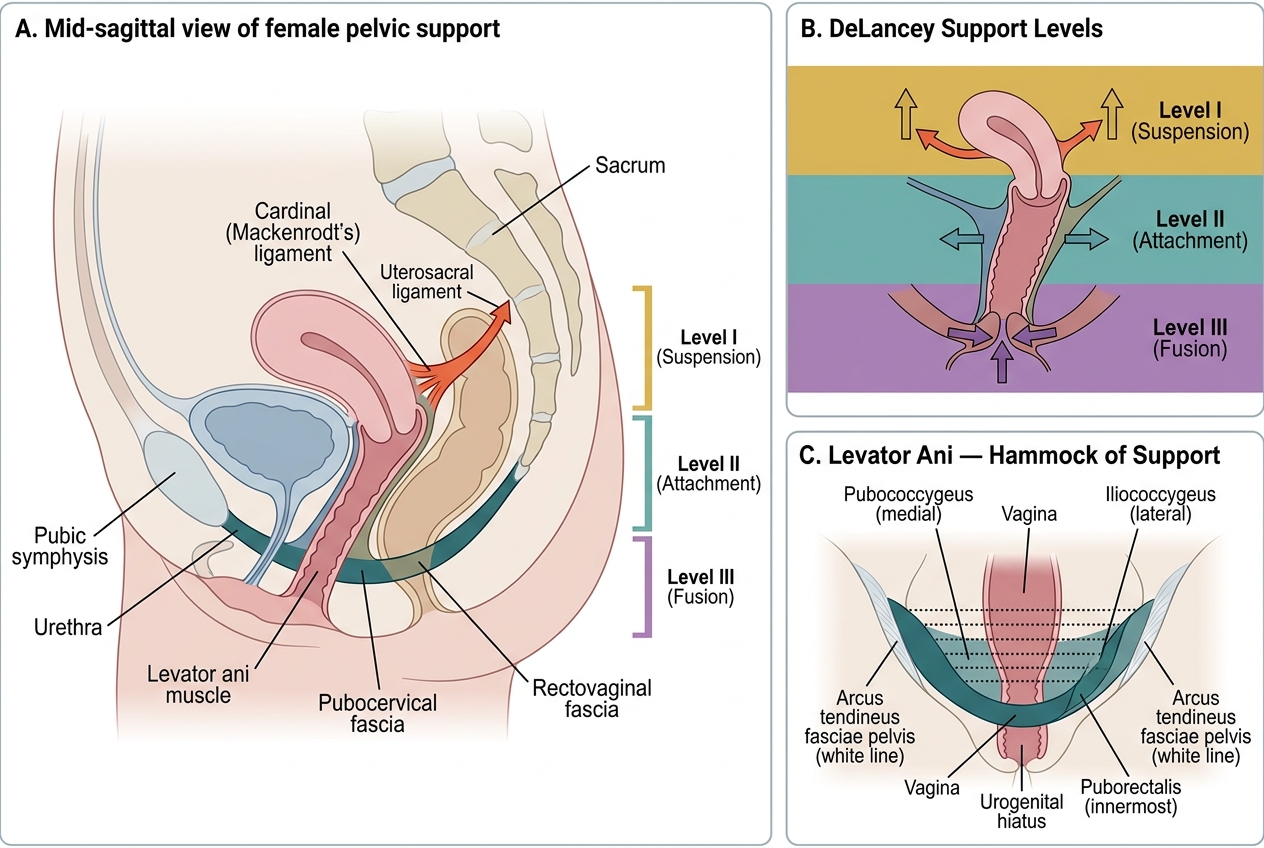
Pelvic Floor Support Structures and DeLancey's Three Levels of Vaginal Support
Aetiology and risk factors: The most important risk factor is vaginal childbirth — particularly prolonged second stage, instrumental delivery (forceps), delivery of a large baby, and unrepaired perineal tears. These injure the levator ani, stretch the ligamentous supports, and damage the pudendal nerve. Multiparity (especially ≥3 deliveries) is the single strongest risk factor in India. Menopause and oestrogen deficiency accelerate atrophy of collagen in the pelvic floor. Chronic raised intra-abdominal pressure from chronic cough, constipation, obesity, or heavy manual labour overloads the already compromised supports. Congenital connective tissue disorders (e.g. Marfan, Ehlers-Danlos) predispose even nulliparous women. Racial factors — White and Asian women have higher prolapse rates than Black women, attributed to differences in levator ani muscle anatomy.
Pathophysiology of Prolapse
The pathophysiology of uterine prolapse is best understood as a progressive failure of the integrated pelvic support system rather than a single-structure injury. Under normal conditions, the levator ani maintains the genital hiatus closed; the vagina lies horizontally over the levator plate, and the uterus is kept anterosuperior to the rectum by the cardinal-uterosacral complex. When this system fails at one or more DeLancey levels, the downward force of intra-abdominal pressure is no longer counteracted.
The primary pathological events are: (1) stretching and denervation of the levator ani during childbirth — the pubovisceral muscle is the most commonly injured component, widening the genital hiatus and converting the horizontal vaginal axis to a more vertical orientation; (2) tearing or attenuation of the fascial condensations — the cardinal and uterosacral ligaments lose collagen strength, particularly under the influence of oestrogen deficiency; (3) progressive descent — once the levator plate can no longer close the hiatus, the vaginal walls and uterus herniate downward with each Valsalva manoeuvre, analogous to a hernia through a defect. The process is typically slow and progressive over years, with menopause markedly accelerating the collagen degradation. The cervix descends first (descent), then appears at the introitus (procidentia first degree), and in the most advanced cases the entire uterus everts outside the vagina (procidentia or complete prolapse) — at which point the bladder base, rectum, and sometimes loops of small bowel (enterocele) are drawn down with it.
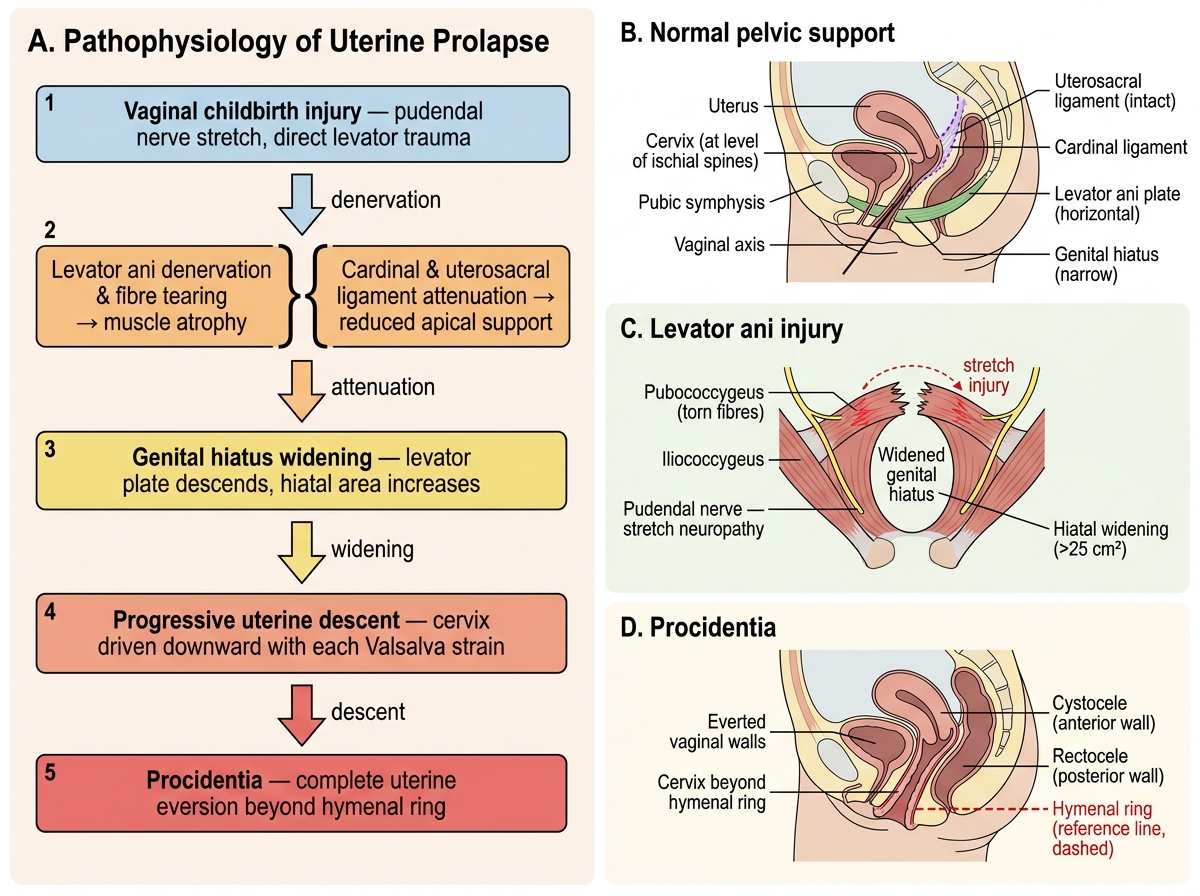
Pathophysiology of Uterine Prolapse: From Childbirth Injury to Procidentia
SELF-CHECK
A 55-year-old multiparous woman is found on examination to have her cervix 2 cm beyond the hymenal ring on maximum Valsalva. The total vaginal length is 8 cm. What is her POP-Q stage?
A. Stage I — cervix more than 1 cm above the hymen
B. Stage II — cervix within 1 cm either side of the hymen
C. Stage III — cervix more than 1 cm beyond the hymen but not total eversion
D. Stage IV — complete eversion equal to total vaginal length
Reveal Answer
Answer: C. Stage III — cervix more than 1 cm beyond the hymen but not total eversion
POP-Q Stage III is defined as the most distal prolapsed portion being more than 1 cm below the hymenal plane but not reaching total vaginal length minus 2 cm. Here the cervix is 2 cm beyond the hymen (+2 cm), which exceeds the +1 cm threshold for Stage III, and total eversion would require ≥ total vaginal length (8 cm) minus 2 cm = 6 cm beyond the hymen. Stage II would be within ±1 cm of the hymen; Stage IV would be complete eversion.