Page 7 of 24
OG31.1 | Uterine Prolapse — SDL Guide (Part 3)
Management — Surgical Options
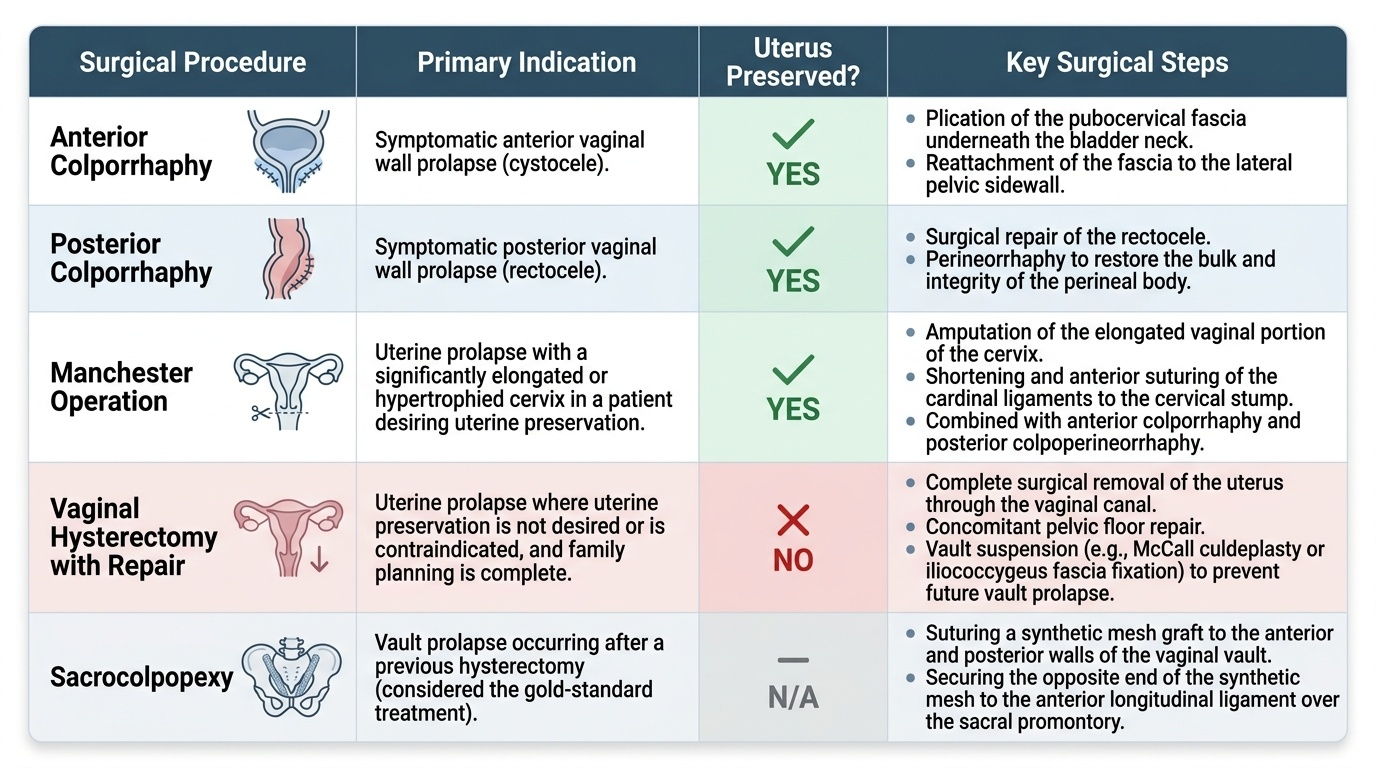
Surgery is indicated for symptomatic prolapse when conservative management has failed, when the patient is fit for anaesthesia, and when family is complete (except in uterus-preserving procedures). The choice of operation depends on the compartments involved, the patient's age and sexual activity, the surgeon's expertise, and the degree of prolapse.
Anterior colporrhaphy repairs the cystocele by plicating the pubocervical fascia under the bladder neck and reattaching it to the lateral pelvic sidewall. Posterior colporrhaphy and perineorrhaphy repair the rectocele and restore perineal body bulk. These are frequently combined with vaginal hysterectomy for uterine prolapse, after which a vault suspension (McCall culdeplasty or iliococcygeus fascia fixation) prevents vault prolapse.
The Manchester (Fothergill) operation is a uterus-preserving procedure: it combines anterior colporrhaphy with amputation of the elongated cervix and posterior colpoperineorrhaphy. The cardinal ligaments are shortened and sutured anteriorly to the cervical stump. It is indicated when the patient desires uterine preservation but has a significantly elongated or hypertrophied cervix. It is contraindicated in cases of cervical malignancy, desire for future pregnancy (cervical incompetence risk), and significant uterine pathology.
Sacrohysteropexy (open or laparoscopic) uses synthetic mesh to attach the posterior cervix to the sacral promontory, preserving the uterus — preferred for younger, sexually active women desiring uterine preservation when no cervical elongation is present. Sacrocolpopexy is the gold-standard procedure for vault prolapse after hysterectomy — mesh is sutured to the vaginal vault and the sacral promontory. Le Fort's colpocleisis (partial colpocleisis) obliterates the vaginal lumen and is reserved for very elderly, sexually inactive women with complete procidentia who are poor surgical risks — it has the lowest recurrence rate but makes the vaginal route permanently inaccessible.
Provided image
Prevention of Uterine Prolapse
Prevention of prolapse operates at three levels — primary (prevent the initial damage), secondary (early detection and treatment before progression), and tertiary (rehabilitation after surgery). Since the most critical damage occurs during childbirth, obstetric practice is central to prevention.
Antenatal: Antenatal pelvic floor muscle training (taught from the second trimester) builds levator ani strength. Nutritional support to prevent anaemia and protein deficiency strengthens connective tissue. Intrapartum: Active management of the second stage to prevent a prolonged second stage; judicious use of episiotomy (mediolateral, not routine, but when indicated to prevent a third-degree tear); avoidance of unnecessary fundal pressure; and prompt repair of all perineal tears — especially third- and fourth-degree tears — under adequate anaesthesia. Restricting instrumental delivery (forceps/vacuum) to trained obstetricians reduces levator ani avulsion injury. Postpartum: Early postnatal pelvic floor exercises beginning within 24 hours of delivery; early treatment of postnatal perineal wound complications; and delayed return to heavy manual labour.
Long-term prevention: Treatment of chronic cough (smoking cessation, asthma management), management of constipation with dietary fibre and adequate hydration, weight management, and postmenopausal hormone replacement therapy (topical oestrogen at minimum) to maintain connective tissue strength. Public health measures in rural India include improving institutional delivery rates, training traditional birth attendants, promoting small family norms, and reducing heavy agricultural labour in the early postpartum period.
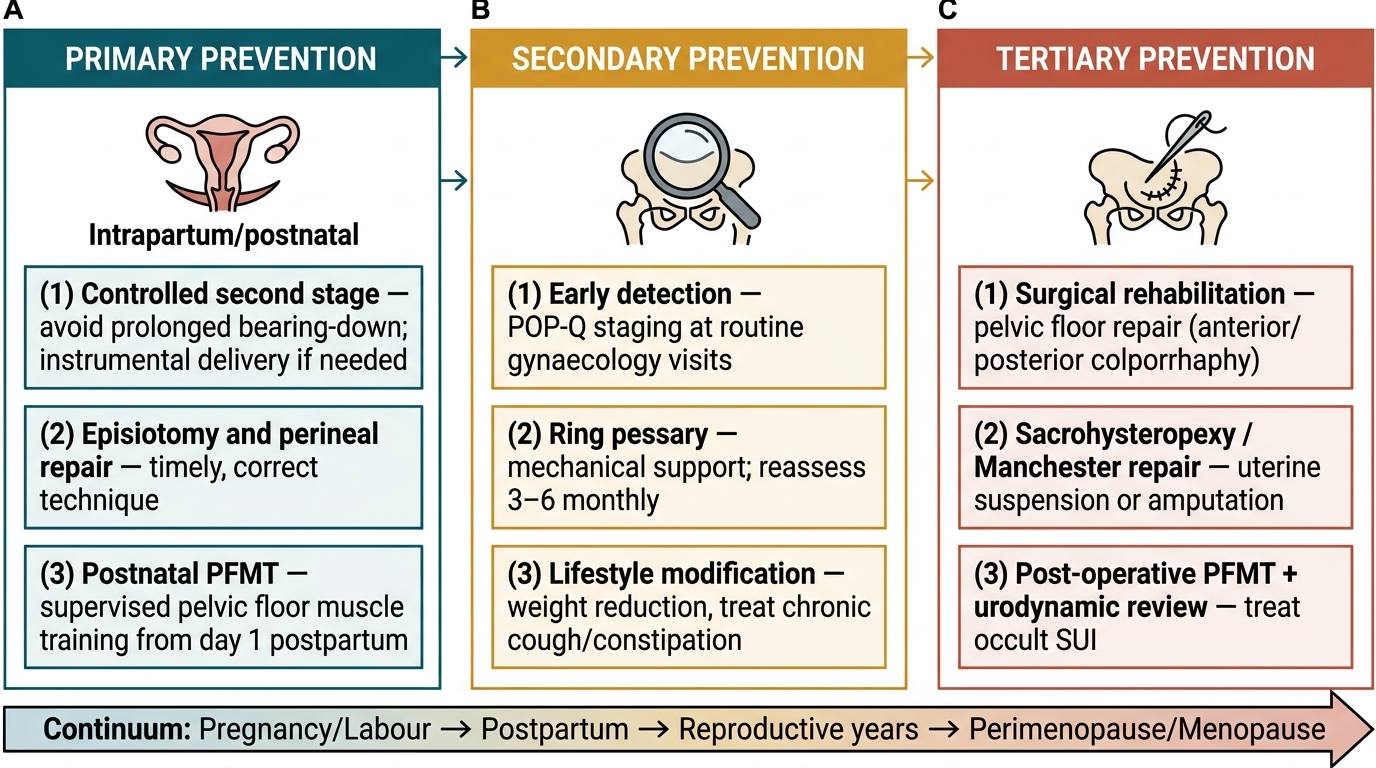
Three-Level Prevention Framework for Uterine Prolapse
SELF-CHECK
A 48-year-old woman with Stage II uterine prolapse, a cystocele, and stress urinary incontinence wishes to avoid surgery. Which is the MOST appropriate first-line management?
A. Manchester operation
B. Sacrohysteropexy with mesh
C. Ring pessary combined with pelvic floor muscle training and topical oestrogen
D. Anterior colporrhaphy alone
Reveal Answer
Answer: C. Ring pessary combined with pelvic floor muscle training and topical oestrogen
For a patient who wishes to avoid surgery with Stage II prolapse, the first-line management is conservative: a ring pessary provides mechanical support, supervised pelvic floor muscle training strengthens the levator ani, and topical oestrogen improves vaginal atrophy (she is likely perimenopausal). Manchester operation and sacrohysteropexy are surgical options. Anterior colporrhaphy alone addresses only the cystocele and not the uterine descent.
CLINICAL PEARL
The pessary-surgery decision hinge — always do urodynamics first: Before performing any prolapse repair surgery, urodynamic studies are mandatory. Up to 40% of women with prolapse have occult (masked) stress urinary incontinence that only becomes apparent after the prolapse is reduced (because the prolapse was kinking the urethra and providing an inadvertent continence mechanism). If urodynamics reveals occult stress incontinence, a mid-urethral sling procedure should be planned simultaneously with the prolapse repair. Proceeding with prolapse repair alone in these women results in de-novo severe stress incontinence post-operatively — a distressing complication that could have been predicted and treated.
SELF-CHECK
Which operation for uterine prolapse preserves the uterus by combining cervical amputation with anterior colporrhaphy and posterior colpoperineorrhaphy?
A. Sacrocolpopexy
B. Le Fort's colpocleisis
C. Manchester (Fothergill) operation
D. Vaginal hysterectomy with pelvic floor repair
Reveal Answer
Answer: C. Manchester (Fothergill) operation
The Manchester (Fothergill) operation preserves the uterus by amputating the elongated cervix, shortening and reattaching the cardinal ligaments to the cervical stump, performing anterior colporrhaphy, and posterior colpoperineorrhaphy. It is indicated for prolapse with cervical elongation in women desiring uterine preservation. Sacrocolpopexy is for vault prolapse. Le Fort's colpocleisis obliterates the vaginal lumen without preserving sexual function. Vaginal hysterectomy removes the uterus.
Self-Assessment
Review these key points to consolidate your understanding of uterine prolapse. The POP-Q system is the international standard, using the hymenal ring as the zero reference point: Stage 0 (no prolapse) → Stage I (most distal portion >1 cm above the hymen) → Stage II (within ±1 cm of the hymen, the symptomatic threshold) → Stage III (>1 cm beyond the hymen) → Stage IV (complete eversion). The traditional system grades uterine descent as 1st degree (cervix in vagina), 2nd degree (cervix at introitus), and 3rd degree/procidentia (cervix outside). DeLancey's three levels of support (Level I cardinal/uterosacral, Level II paravaginal fascial, Level III perineal body) explain why different compartments fail and guide surgical repair. The Manchester operation preserves the uterus by amputating the elongated cervix, shortening cardinal ligaments, and performing anterior and posterior repair — contraindicated when future pregnancy is desired, as cervical amputation risks incompetence. Urodynamic studies before any prolapse repair surgery are mandatory to detect occult stress incontinence in up to 40% of patients. Pessary management (ring pessary, PFMT, topical oestrogen) is first-line for those unfit for or declining surgery. Prevention starts with skilled intrapartum care: avoiding prolonged second stage, prompt repair of perineal tears, and early postpartum pelvic floor exercises.