Page 22 of 37
OG34.3 | Gestational Trophoblastic Disease — SDL Guide (Part 3)
Management of High-Risk GTN and Special Situations
High-risk GTN (WHO/FIGO prognostic score ≥7) requires multi-agent combination chemotherapy from the outset because single-agent methotrexate or actinomycin-D has a primary failure rate exceeding 50% in this group — the biological complexity and drug resistance mechanisms that accumulate with higher-score disease cannot be overcome by a single agent. The international standard regimen is EMA-CO, an acronym that encodes its component drugs: Etoposide, Methotrexate, Actinomycin-D (the EMA component, given on days 1 and 2) alternating with Cyclophosphamide and vincristine (Oncovin, the CO component, given on day 8), cycling every 2 weeks. This regimen was designed by Bagshawe and colleagues at Charing Cross Hospital in London, the world's first specialist GTD treatment centre, and has been validated in large cohort studies demonstrating overall survival rates of 85–95% even in Stage IV disease — a remarkable achievement for a chemotherapy regimen treating a disseminated malignancy. The key to its efficacy lies in the non-cross-resistant drug combinations and the compressed 2-week cycle, which maintains selective pressure on trophoblastic cells without allowing sufficient time for significant tumour repopulation between cycles.
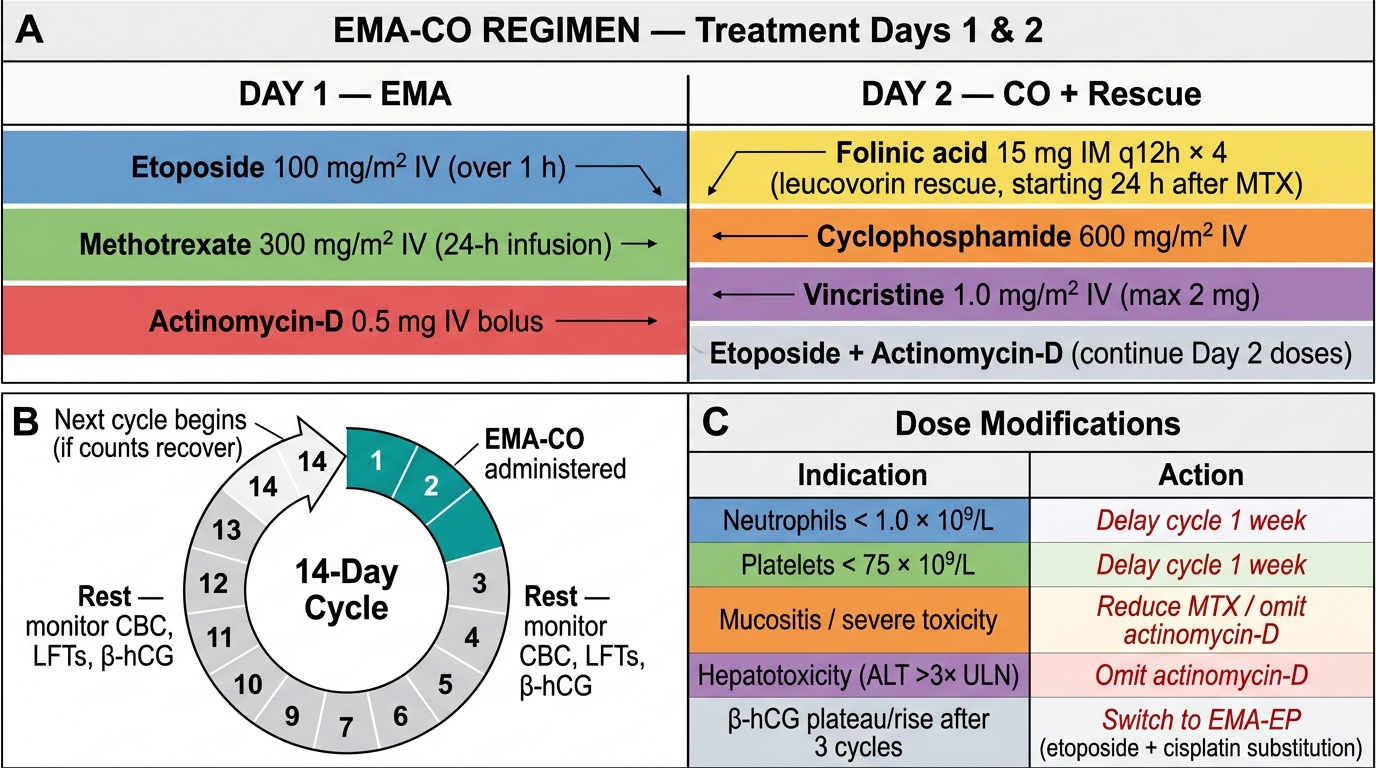
EMA-CO regimen (each cycle = 2 weeks):
- Day 1: Etoposide 100 mg/m² IV, Methotrexate 300 mg/m² IV (over 12 hours), Actinomycin-D 0.5 mg IV (EMA component)
- Day 2: Folinic acid rescue 15 mg oral every 12 hours × 4 doses (starting 24 hours after methotrexate), Actinomycin-D 0.5 mg IV (EMA component day 2)
- Day 8: Cyclophosphamide 600 mg/m² IV, Vincristine (Oncovin) 1.0 mg/m² IV (CO component)
Treatment continues until β-hCG normalises, then three consolidation courses (one more than low-risk — reflecting the higher relapse risk). Response is assessed by weekly β-hCG; a rising β-hCG on EMA-CO triggers salvage protocols.
Salvage regimens for EMA-CO failure include EMA-EP (replacing CO with cisplatin + etoposide), TP/TE (paclitaxel-cisplatin / paclitaxel-etoposide alternating), or high-dose chemotherapy with autologous stem cell rescue in selected cases. Salvage rates of 70–80% are achievable even after EMA-CO failure.
Special situations:
- Brain metastases: intrathecal methotrexate is added, or the methotrexate dose in EMA is increased to 1 g/m² with folinic acid rescue. Whole-brain radiotherapy may be considered in selected cases. Neurosurgical evacuation of a haemorrhagic cerebellar or accessible deposit may be life-saving.
- Liver metastases: particularly haemorrhage from hepatic deposits may require emergency embolisation. Liver involvement shifts the prognostic score to ≥4 for this variable (maximum weight), making high-risk classification almost inevitable.
- PSTT and ETT: because these tumours arise from intermediate trophoblast and are relatively chemoresistant, hysterectomy is the preferred treatment for Stage I disease. For metastatic PSTT/ETT, EMA-CO is given but long-term outcomes are less favourable than for choriocarcinoma.
- Fertility preservation: hysterectomy is reserved for patients with uterine perforation, uncontrolled haemorrhage, or chemotherapy failure. The majority of women with GTN can retain their uterus and fertility. After completing chemotherapy and surveillance, subsequent pregnancies have a normal incidence of congenital abnormalities — this is one of the most reassuring counselling points in oncology.
EMA-CO Chemotherapy Regimen: Schedule, Cycle Interval, and Dose Modifications
CLINICAL PEARL
GTN is the clearest example of oncological management driven by a serum tumour marker rather than imaging or histology. The diagnosis of post-molar GTN is made on β-hCG kinetics alone (plateau, rise, or failure to normalise) — a biopsy is not required and is in fact dangerous in vascular trophoblastic disease. This means a patient can be staged and treated for a potentially metastatic malignancy based entirely on serial blood tests and CT imaging. The WHO/FIGO prognostic score allocates a specific numerical weight to each risk variable — most importantly, the interval from the index pregnancy and pre-treatment β-hCG level. A woman who presents late (interval >12 months) with very high β-hCG automatically scores heavily towards high-risk. Always refer patients with WHO/FIGO score ≥7, brain or liver metastases, or stage IV disease to a specialist GTD treatment centre — outcomes at specialist centres substantially exceed those at general hospitals, and the RCOG recommends registration of all GTD patients with the national GTD registry.
SELF-CHECK
A woman with GTN has a WHO/FIGO score of 9 (high-risk) and is commenced on EMA-CO. After 3 cycles, her β-hCG has plateaued at 850 mIU/mL (previously 4,200 → 2,800 → 900 → 850 mIU/mL). What is the appropriate next step?
A. Continue EMA-CO for 3 more cycles before reassessing
B. Switch to a salvage regimen such as EMA-EP
C. Proceed immediately to hysterectomy
D. Add intrathecal methotrexate
Reveal Answer
Answer: B. Switch to a salvage regimen such as EMA-EP
A β-hCG plateau after two consecutive EMA-CO cycles indicates treatment resistance. The appropriate next step is to switch to a salvage regimen — EMA-EP (replacing the CO component with cisplatin and etoposide) is the most commonly used first salvage. Continuing EMA-CO in the face of plateau wastes cycles, allows disease to progress, and may select for further resistance. Hysterectomy is not the first response to chemotherapy resistance in high-risk GTN — systemic disease means local surgery alone is inadequate. Intrathecal methotrexate is added for documented CNS metastases, not routinely for systemic resistance.
Prognosis and Surveillance After GTD
The prognosis of GTD is exceptional relative to other malignancies and stands as a landmark achievement of modern oncology. Even high-risk, stage IV choriocarcinoma with brain metastases has an overall survival exceeding 75–80% at specialist centres, and low-risk GTN is curable in nearly 100% of cases with appropriate treatment. This extraordinary chemosensitivity, combined with the availability of a quantitative, sensitive tumour marker in β-hCG, has made GTN one of the first human malignancies to be reliably cured with systemic chemotherapy — an advance pioneered at the Charing Cross Hospital in the 1950s and 1960s that fundamentally changed the trajectory of this previously fatal disease. The clinical implication is profound: unlike most other solid tumours where metastatic disease is managed with palliative intent, metastatic GTN is managed with curative intent, and this must guide both the physician's approach and the communication to the patient. The key prognostic factors beyond stage are the WHO/FIGO score (which reflects biological aggressiveness), the timeliness of diagnosis and treatment (delayed treatment allows selection for more resistant clones), and whether the patient is managed at a specialist GTD centre (outcomes at specialist centres with high caseload and centralised β-hCG registry support are substantially better than at general hospitals).
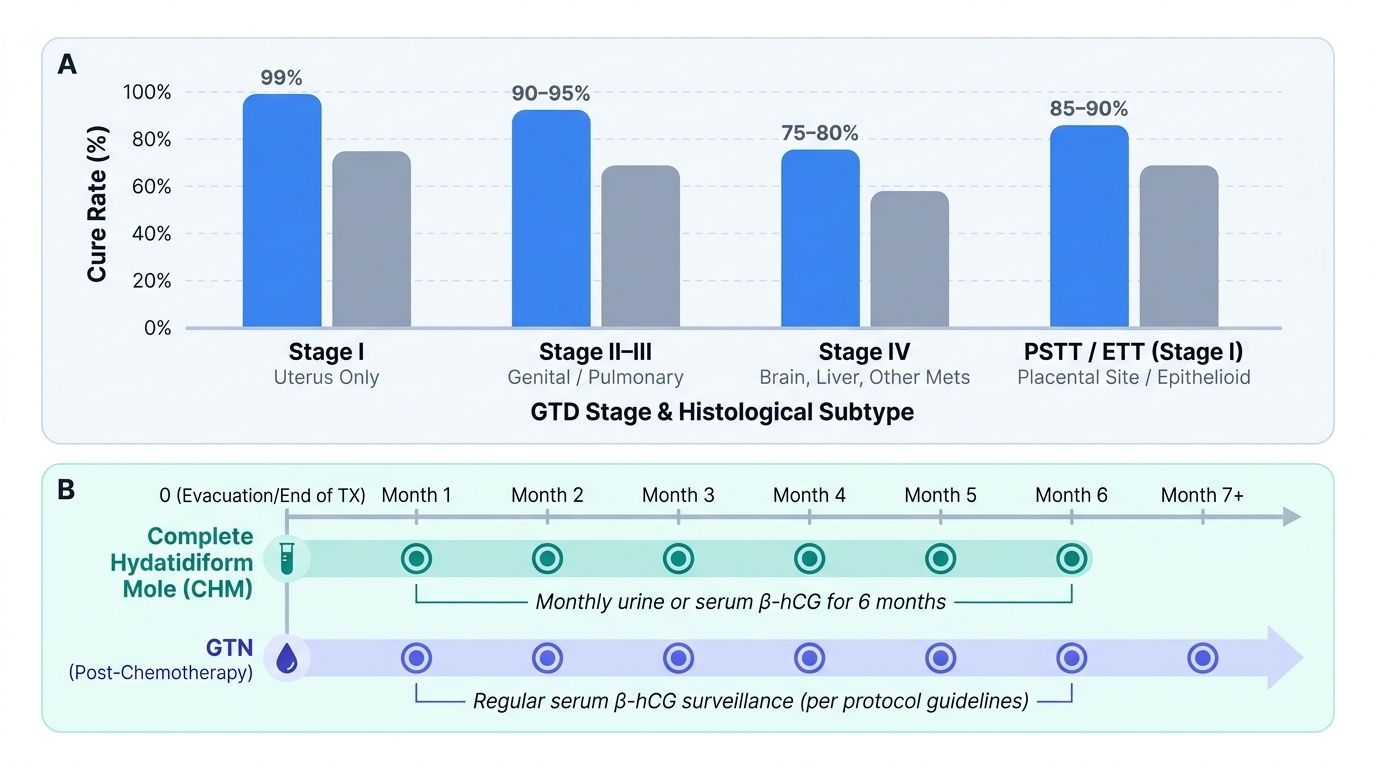
Stage-stratified outcomes (approximate):
- Stage I (uterus only): cure rate >99% with chemotherapy ± hysterectomy
- Stage II–III (genital/pulmonary): cure rate 90–95%
- Stage IV (brain, liver, other): cure rate 75–80% at specialist centres
- PSTT/ETT (Stage I): 85–90% with hysterectomy; lower for metastatic disease
Post-treatment surveillance protocol (per RCOG guidelines):
- After complete hydatidiform mole: monthly urine or serum β-hCG for 6 months if β-hCG normalises within 56 days of evacuation; extend to 6 months of monitoring if β-hCG is not normal by 56 days; patients with PHM: monthly × 6 months
- After GTN treatment: weekly β-hCG until three consecutive normals; then monthly for 12 months
- All patients: contraception (OCP preferred) for the entire surveillance period to prevent diagnostic confusion with a new pregnancy
Subsequent pregnancy outcomes: women who conceive after completing GTD surveillance have no increased risk of miscarriage, congenital abnormality, stillbirth, or obstetric complications compared with the general population — this is an important and reassuring counselling point. Pregnancy should be deferred for at least 12 months after completing surveillance (to avoid misinterpreting a new pregnancy as GTN recurrence), but there is no permanent reproductive impairment from GTD treatment.
GTD registry registration: in the UK, all patients with GTD are registered with three designated GTD treatment centres (Charing Cross, Sheffield, Dundee) which provide centralised expert oversight of β-hCG surveillance. In India, GTD registries are being established through FOGSI and ICMR; referral to a centre with GTD expertise is recommended for all high-risk GTN cases.
Provided image
SELF-CHECK
A 26-year-old woman completes successful treatment for Stage III, WHO score 5 (low-risk) GTN with methotrexate. β-hCG has been normal for 3 months. She asks when she can try for a pregnancy. What is the correct advice?
A. She may try to conceive immediately as β-hCG is normal
B. She should wait at least 12 months from the completion of surveillance before trying to conceive
C. She should never attempt pregnancy as GTN is hereditary
D. She should wait 5 years to ensure no late recurrence
Reveal Answer
Answer: B. She should wait at least 12 months from the completion of surveillance before trying to conceive
Per standard GTD guidelines (RCOG, FIGO), women should defer pregnancy for at least 12 months after completing GTD surveillance — not from the end of treatment. This ensures that any β-hCG rise from a new pregnancy cannot be confused with GTN recurrence. There is no evidence of increased hereditary risk to offspring, no increased congenital abnormality rate, and no obstetric risk in subsequent pregnancies. A 5-year wait is not required; 12 months of surveillance completion is the standard threshold.