Page 28 of 37
OG34.5 | Major Operative Gynaecology — SDL Guide
Learning Objectives
- State the clinical indications and surgical approach selection (abdominal vs vaginal vs endoscopic) for major gynaecological procedures
- Describe the anatomical basis of safe hysterectomy, including the three danger points of the ureter
- Outline the steps of total abdominal hysterectomy (TAH) and its variants (subtotal, radical Wertheim's, with/without BSO)
- Describe abdominal myomectomy, ovarian cystectomy/salpingo-oophorectomy, and the principles of staging laparotomy
- Outline vaginal hysterectomy and pelvic floor repair (anterior/posterior colporrhaphy, Fothergill's operation)
- Describe the principles of laparoscopy (pneumoperitoneum, trocar placement) and hysteroscopy (distension media, fluid deficit monitoring)
- Identify and manage post-operative complications of major gynaecological surgery
- Describe the expected intraoperative findings and what to look for when observing these procedures in theatre
INSTRUCTIONS
Major operative gynaecological procedures — hysterectomy, myomectomy, pelvic floor repair, laparoscopy, and hysteroscopy — represent the surgical core of gynaecological practice. These are the operations you will observe, assist at, and eventually perform under supervision. Understanding the surgical anatomy, operative steps, and complication profiles is essential both for patient safety when you are involved in care and for OSCE, viva, and written examination. This module provides the conceptual framework; surgical competence is built through supervised theatre experience, simulation, and senior mentorship.
References
- DC Dutta's Textbook of Gynecology, 7th ed., Ch 35-37 — Major Gynaecological Operations (textbook)
- Shaw's Textbook of Gynaecology, 17th ed., Ch 35–37 — Operative Gynaecology (textbook)
- TeLinde's Operative Gynecology, 12th ed., Ch 28–32 — Hysterectomy and Pelvic Surgery (textbook)
- RCOG Green-top Guideline No. 29 — Laparoscopic Injuries (2008) (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 45-year-old woman with multiple symptomatic uterine fibroids (the largest 8 cm, causing menorrhagia and bulk symptoms) is listed for a total abdominal hysterectomy. During the consent consultation, she asks three questions: 'Will the surgery affect my ovaries?' 'What are the chances of damaging my bladder or kidney tube?' 'How long will I be in hospital?' She has also heard from a friend that sometimes surgeons 'cut the ureter by mistake'. Meanwhile, in the next operating theatre, a 68-year-old woman with uterovaginal prolapse is undergoing a vaginal hysterectomy and pelvic floor repair. And in the laparoscopy suite, a 32-year-old is undergoing a diagnostic laparoscopy for chronic pelvic pain. How do the principles of these three different operative approaches connect — and what anatomical knowledge keeps the pelvic structures safe in each?
WHY THIS MATTERS
Hysterectomy is the second most common gynaecological surgical procedure worldwide (after caesarean section), with approximately 600,000 performed annually in the USA alone, and a high burden in India driven by fibroids, abnormal uterine bleeding, and pelvic organ prolapse. As a final-year student you will assist at these operations, participate in post-operative rounds, clerk patients being consented, and be expected to counsel patients about what to expect. Laparoscopy is now the preferred diagnostic approach for chronic pelvic pain, endometriosis, and ectopic pregnancy, and laparoscopic hysterectomy is increasingly performed for benign disease. Hysteroscopy has transformed the diagnosis and treatment of intrauterine pathology. Understanding the anatomy, operative steps, and complication profiles of these procedures is not just exam knowledge — it is the knowledge that enables you to identify a post-operative complication, escalate appropriately, and contribute to safe patient care from your very first day on a gynaecological ward.
RECALL
Activate prior anatomical knowledge. From your anatomy studies, recall the relations of the ureter in the pelvis: the ureter crosses the pelvic brim at the bifurcation of the common iliac artery, then travels along the lateral pelvic wall, passes under the uterine artery ('water passes under the bridge'), and runs close to the lateral vaginal fornix before entering the bladder trigone. This course explains why the ureter is at risk at three specific points during hysterectomy. Recall the ligamentous supports of the uterus: the round ligaments (traction, not support), the broad ligament (a peritoneal fold containing the fallopian tubes, round ligaments, and ovarian vessels), the infundibulopelvic (suspensory ovarian) ligament (contains ovarian vessels — clamped if ovaries are removed), the cardinal (transverse cervical) ligaments (primary uterine support from the lateral cervix to the pelvic side wall), and the uterosacral ligaments (posterior support). From your surgical training, recall the principles of haemostasis (ligate before divide), the importance of good exposure (adequate incision, correct retraction), and the role of surgical planes (fascial layers guide dissection and reduce bleeding).
Clinical Indications and Relevance of Major Gynaecological Surgery
The selection of the appropriate major gynaecological procedure — and the appropriate surgical approach — is a clinical decision driven by the indication, the patient's anatomy and comorbidities, the surgeon's skill, and the available resources. The three principal approaches to major gynaecological surgery are abdominal (laparotomy), vaginal, and endoscopic (laparoscopic and hysteroscopic), and each has specific advantages and limitations.
Hysterectomy (removal of the uterus) is indicated for: symptomatic uterine fibroids unresponsive to medical treatment (the most common indication in India), endometrial carcinoma, cervical carcinoma, adenomyosis with intractable menorrhagia, uterovaginal prolapse, and occasionally for PPH (emergency peripartum hysterectomy). The choice of route — abdominal, vaginal, or laparoscopic — depends on: uterine size (large fibroids favour abdominal route), vaginal access (a narrow vagina or nulliparity may favour abdominal), presence of adnexal disease (favours abdominal or laparoscopic), and surgeon training. The vaginal route is preferred for uterovaginal prolapse (a small, mobile uterus accessible from below). Laparoscopic hysterectomy (LAVH or TLH) is increasingly used for benign disease, offering faster recovery and less blood loss than open surgery.
Myomectomy (fibroid removal with uterine preservation) is indicated in women who wish to preserve fertility or who refuse hysterectomy. The surgical approach depends on fibroid characteristics: hysteroscopic resection for submucosal (FIGO type 0/1/2) fibroids; laparoscopic for small-to-moderate intramural or subserosal fibroids; abdominal (open) for large, multiple, or deeply embedded fibroids.
Staging laparotomy is indicated for suspected ovarian malignancy — the surgical steps are detailed in og16-ovarian-cancer (OG34.2). The operative principles (midline incision, systematic exploration, TAH+BSO+omentectomy+node dissection) are shared with other major abdominal gynaecological procedures.
Vaginal hysterectomy + pelvic floor repair is the standard surgical treatment for uterovaginal prolapse with symptomatic cystocoele or rectocoele. Fothergill's Manchester operation is reserved for cervical elongation with moderate prolapse when uterine preservation is preferred — it combines cervical amputation with anterior colporrhaphy and fixation of the cardinal ligaments.
Laparoscopy is the gold standard for diagnosing pelvic pain, endometriosis, and adnexal masses, and is the approach for laparoscopic salpingectomy (ectopic), ovarian cystectomy, and laparoscopic hysterectomy.
Hysteroscopy provides direct visualisation of the uterine cavity for diagnosis (polyp, submucosal fibroid, AUB, uterine anomaly) and operative intervention (polypectomy, myomectomy, endometrial ablation, septum resection).
Ureteric Course and the Three Danger Points in Gynaecological Surgery
Anatomy and Governing Principles of Gynaecological Surgery
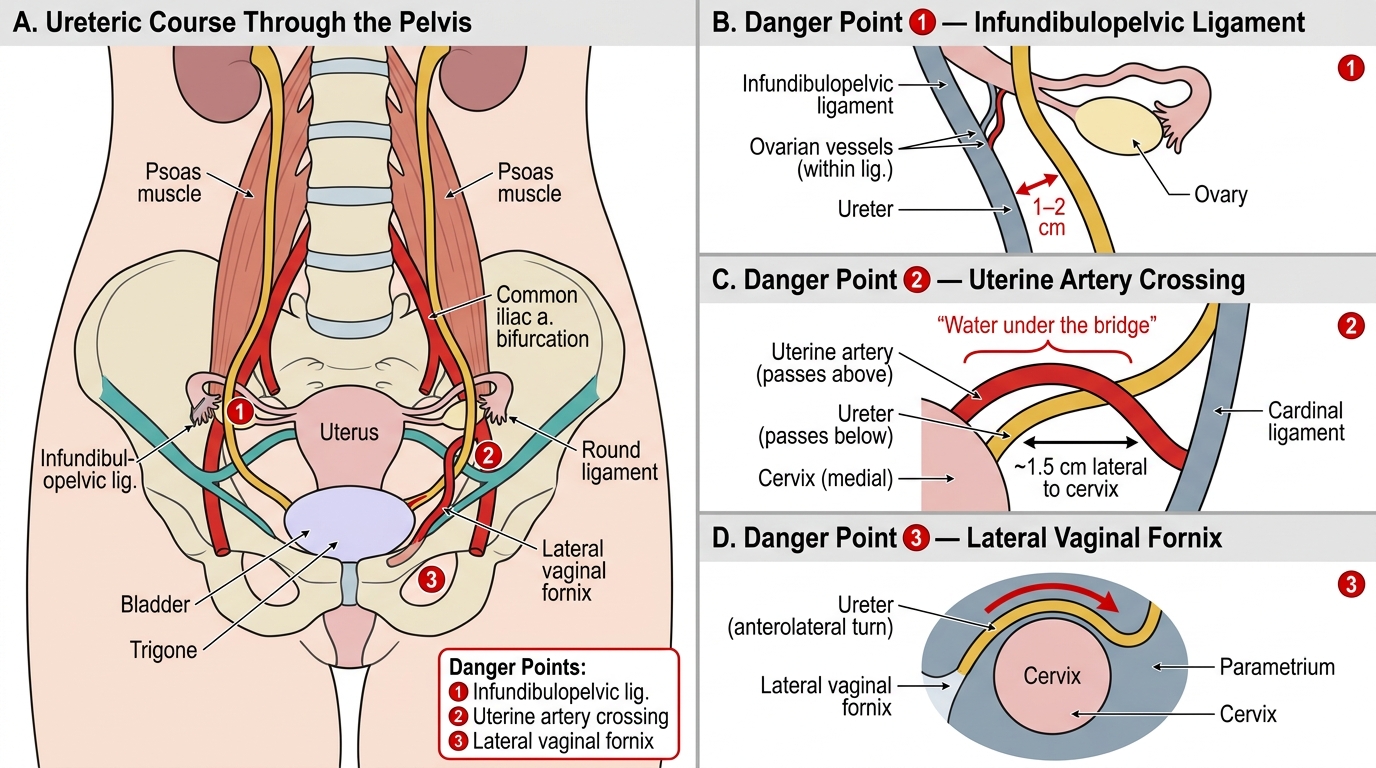
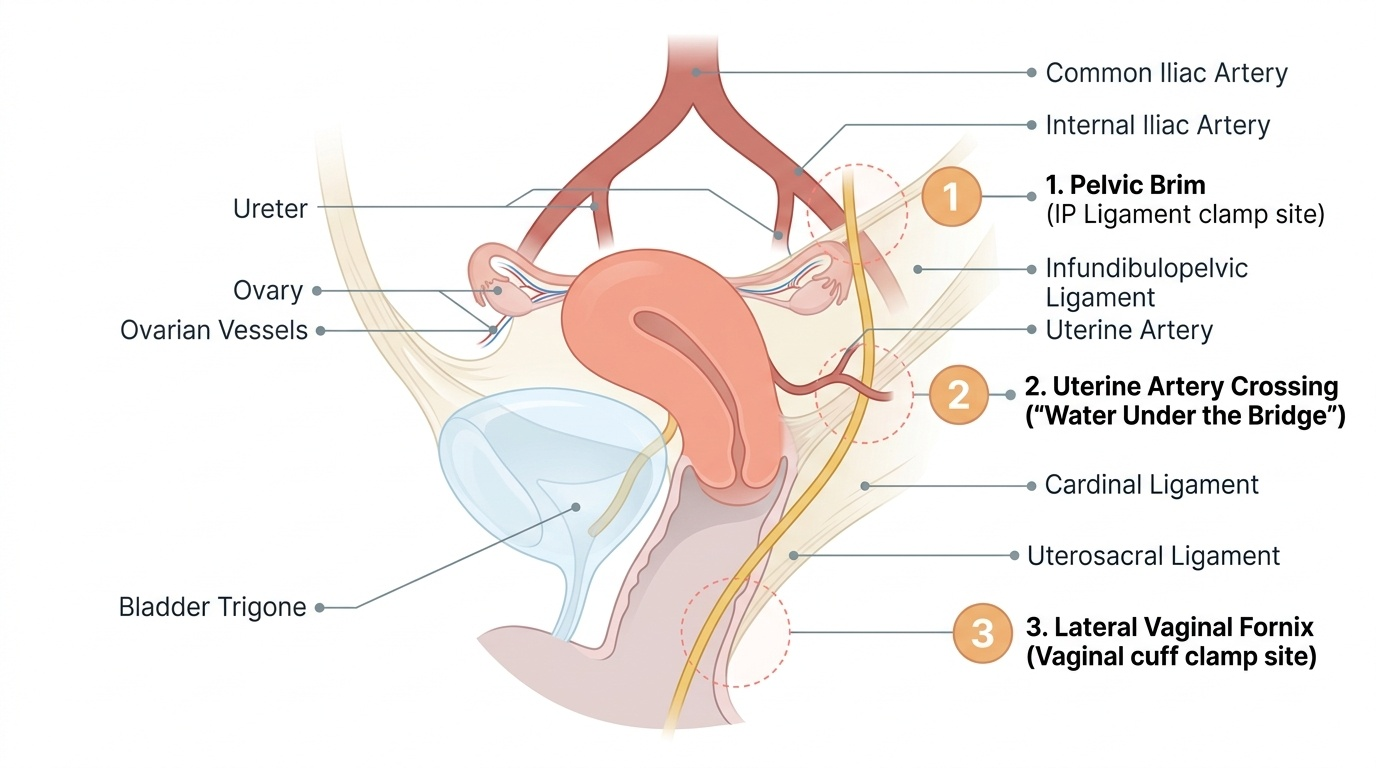
The pelvic surgeon's foremost anatomical concern is the ureter — a structure intimately related to the uterus and its supporting ligaments, invisible at the start of most hysterectomies, and capable of causing catastrophic morbidity if inadvertently ligated, kinked, or transected. The ureter is a retroperitoneal structure approximately 25–30 cm in length that descends from the renal pelvis along the psoas muscle, crosses the pelvic brim at the bifurcation of the common iliac artery, and travels along the lateral pelvic wall before ultimately entering the bladder at the trigone. Throughout this pelvic course the ureter lies in close proximity to the uterus and its ligamentous supports — proximity that makes it uniquely vulnerable during gynaecological dissection. The incidence of ureteric injury during hysterectomy is approximately 0.5–1% and accounts for the majority of serious medicolegal claims in gynaecological surgery. Recognising the three anatomical sites at which the ureter is most vulnerable — and understanding the surgical reason for vulnerability at each site — is the foundation of safe pelvic surgery; it is knowledge that must be automatic before you stand at any operating table for a hysterectomy.
The three danger points of the ureter in gynaecological surgery are:
1. At the pelvic brim — where the ureter crosses the bifurcation of the common iliac artery and enters the pelvis, lying beneath the infundibulopelvic ligament (containing the ovarian vessels). When the infundibulopelvic ligament is clamped for oophorectomy, the ureter may be included in the clamp if it has not been identified and lateralised first.
2. Where the uterine artery crosses the ureter — approximately 1.5 cm lateral to the cervix, the uterine artery passes over the ureter ('water passes under the bridge'). This is the most common site of ureteric injury — when the uterine artery pedicle is clamped close to the cervix, the ureter may be inadvertently clamped, tied, or cut along with it.
3. Near the lateral vaginal fornix — the ureter enters the bladder approximately 1–2 cm lateral to the vaginal angle; when the upper vagina is clamped for the vaginal cuff pedicle, the ureter is vulnerable here.
The bladder is the other major structure requiring constant attention during hysterectomy. The bladder must be mobilised downward off the anterior surface of the lower uterine segment and cervix (bladder reflection, or 'opening the vesicouterine space') before the cervicovaginal junction can be safely approached. Inadequate mobilisation is the commonest cause of inadvertent cystotomy.
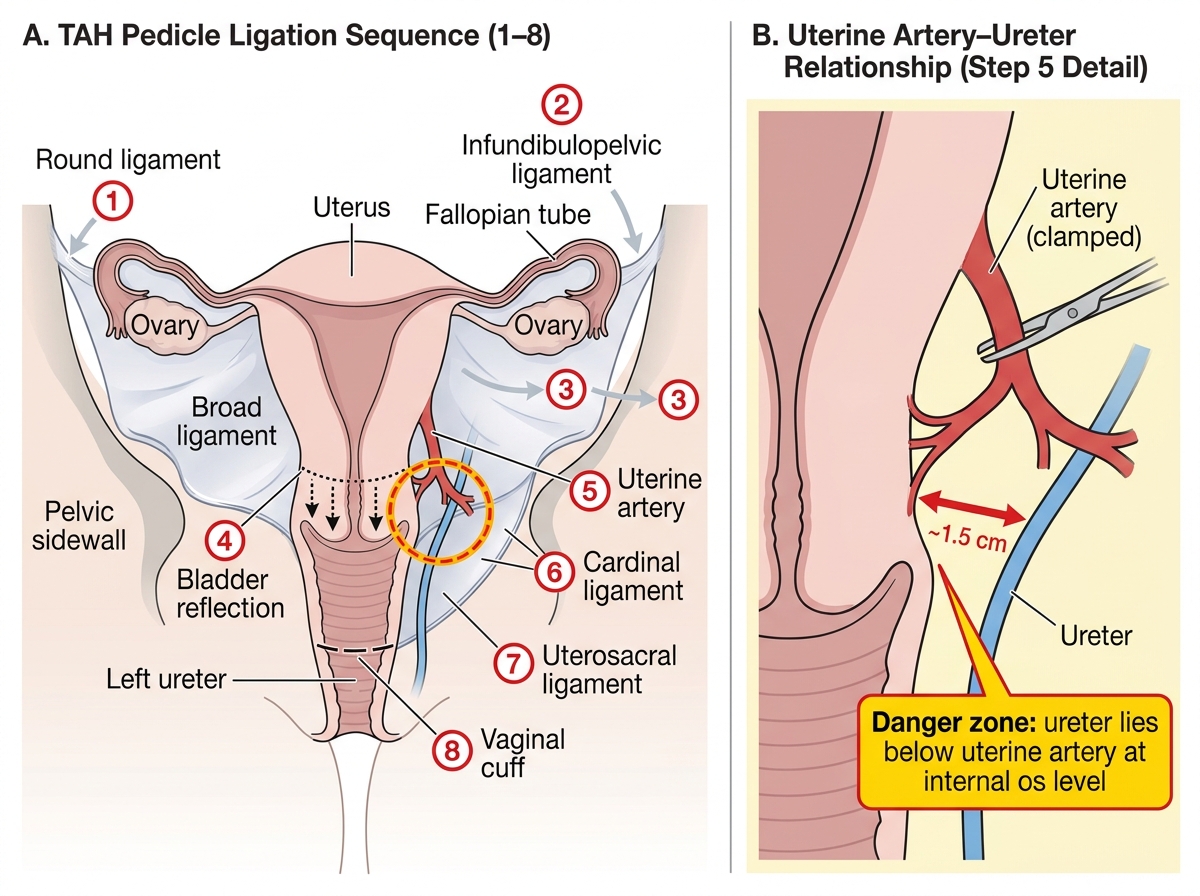
The ligamentous anatomy governs the sequence of pedicle ligation in hysterectomy. Proceeding systematically from lateral to medial and superior to inferior ensures each vascular pedicle is secured before the adjacent structures are divided. The sequence: round ligament → infundibulopelvic ligament (if ovaries removed) or utero-ovarian ligament (if ovaries retained) → broad ligament → bladder reflection → uterine artery → cardinal ligament → uterosacral ligament → vaginal cuff.
The principles of haemostasis in pelvic surgery are: identify each structure before clamping; apply clamps close to the uterus (not close to the pelvic wall) to keep lateral structures — ureter, iliac vessels — out of the pedicle; ligate each pedicle with two ties (transfixion suture + free tie) before dividing; inspect pedicles before closure for bleeding.
Provided image
Abdominal Hysterectomy — Technique and Variants
Total abdominal hysterectomy (TAH) is the most common major gynaecological operation and the foundational pelvic surgical procedure that every final-year student must understand in systematic detail. It is performed via a transverse (Pfannenstiel) or midline vertical incision — the choice of incision is itself a clinical decision: midline is used for large fibroids, ovarian masses, staging laparotomy, and when access to the upper abdomen is required; Pfannenstiel is used for benign conditions with a normal-to-moderately enlarged uterus, offering a cosmetically superior scar and fewer wound complications, though it provides limited access for large or complex masses. Regardless of incision type, the operative logic of TAH follows a consistent anatomical sequence — lateral to medial, superior to inferior — in which each pedicle is secured before the adjacent structure is approached. Understanding this sequence as a logical principle (not a memorised list) allows you to follow any surgeon's technique and to predict the next operative step throughout the procedure.
The operative sequence of TAH, step by step:
1. Peritoneal entry and examination of pelvis and upper abdomen for unexpected pathology
2. Pack bowel cephalad; Trendelenburg position improves pelvic exposure
3. Round ligament ligation and division bilaterally — provides entry to the broad ligament and identifies the infundibulopelvic ligament
4. Broad ligament opening — creates the retroperitoneal space through which the ureter can be identified
5. Infundibulopelvic ligament (for TAH + BSO): identify the ureter before clamping; clamp, divide, and doubly ligate. Alternatively, the utero-ovarian ligament + fallopian tube are ligated for ovarian conservation (TAH without BSO)
6. Bladder reflection — the vesicouterine peritoneum is opened and the bladder is dissected off the lower uterine segment with careful blunt/sharp dissection to expose the cervicovaginal junction
7. Uterine artery ligation — the uterine artery is identified at the level of the internal os, clamped close to the uterus (medial to the ureter), divided, and doubly ligated; this is the most critical haemostatic step
8. Cardinal and uterosacral ligament division — progressing downward to the cervicovaginal junction
9. Vaginal cuff incision — circumferential incision through the vaginal vault, removing the uterus and cervix en bloc
10. Vaginal cuff closure — suture of the vaginal angles (incorporating the uterosacral ligaments for vault support), central closure with or without a drain
11. Pedicle check and peritoneal closure
Variants: Subtotal (sub-cervical) hysterectomy — cervix is retained; faster, less risk of ureteric/bladder injury, but cervical smear surveillance must continue. Radical (Wertheim's) hysterectomy — performed for cervical carcinoma (Stages IB1/IB2); adds removal of the parametrium (cardinal and uterosacral ligaments widely), upper 2 cm of vagina, and pelvic lymph node dissection; much higher risk of ureteric devascularisation, bladder denervation (neurogenic bladder), and lymphocoele. TAH with BSO is performed when ovarian pathology co-exists, or at the patient's request after appropriate counselling regarding surgical menopause.
TAH Pedicle Ligation Sequence and Uterine Artery–Ureter Anatomy
SELF-CHECK
During TAH for large fibroids, the surgeon clamps the right uterine artery pedicle. Post-operatively on day 3, the patient has fever, right loin pain, and anuria. Cystoscopy shows no ureteral jets on the right. What is the most likely intraoperative event and what investigation confirms it?
A. Bladder cystotomy — confirmed by cystoscopy showing a defect in the bladder wall
B. Right ureteric ligation — confirmed by CT urogram showing right hydronephrosis and lack of ureteric opacification below the ligature
C. Pelvic haematoma compressing the ureter — confirmed by ultrasound pelvis
D. Post-operative UTI causing ureteric spasm — confirmed by urine culture
Reveal Answer
Answer: B. Right ureteric ligation — confirmed by CT urogram showing right hydronephrosis and lack of ureteric opacification below the ligature
Anuria on one side (no ureteral jet on the right on cystoscopy) with ipsilateral loin pain and fever on day 3 post-hysterectomy is classic for right ureteric ligation or kinking — the most common serious complication of hysterectomy, occurring most often at the level of the uterine artery pedicle. CT urogram (intravenous urography) will show proximal right hydronephrosis, delayed nephrogram, and absence of distal ureteric opacification. Management: ureteric stenting (if possible) or ureterotomy/reimplantation by a urologist.