Page 31 of 37
OG34.5 | Major Operative Gynaecology — SDL Guide (Part 4)
Self-Assessment
Test your understanding with the following self-assessment scenarios. Work through each independently before reading the explanation.
Scenario 1 — Indication and approach selection: A 38-year-old nulliparous woman has a 10 cm intramural fibroid causing menorrhagia and requesting fertility preservation. She has failed medical management. What is the most appropriate surgical approach and why? Answer: Abdominal myomectomy is preferred for a 10 cm intramural fibroid in a fertility-seeking woman — large fibroids of this size are generally too large for laparoscopic approach without highly specialised equipment. Hysterectomy is not appropriate (fertility desired). Hysteroscopic myomectomy is not appropriate (intramural, not submucosal). She must be counselled that: (a) there is a 5–10% risk of intraoperative haemorrhage requiring conversion to hysterectomy (and this must be included in the consent); (b) future delivery will likely need caesarean section.
Scenario 2 — Complication recognition: A 52-year-old woman underwent TAH+BSO 8 days ago for a large fibroid uterus. She is readmitted with fever (38.8°C), constant watery vaginal discharge beginning 4 days ago, and right flank pain. Serum creatinine is 145 µmol/L (previously normal). What complication has occurred and what is the investigation and management? Answer: The combination of watery vaginal discharge + right flank pain + raised creatinine suggests a right ureterovaginal fistula — urine leaking from an injured right ureter into the vaginal vault. Investigation: CT urogram (shows right hydronephrosis and extravasation at the ureterovaginal junction); flexible cystoscopy + retrograde uretero-pyelogram. Management: urological referral; attempt endoscopic ureteric stenting; if unsuccessful, surgical repair (ureteroneocystostomy) after 6–12 weeks.
Scenario 3 — Consent counselling point: A patient asks what the risk of bladder injury is during her hysterectomy and how it would be managed. Answer: Cystotomy (inadvertent bladder entry) occurs in approximately 0.5–1% of hysterectomies. If recognised intraoperatively, it is repaired immediately in two layers with absorbable sutures; catheter remains for 7–14 days and recovery is complete. If unrecognised intraoperatively, it presents as vesicovaginal fistula 7–14 days post-operatively (constant urinary dribbling from the vagina) and requires delayed surgical repair 6–12 weeks after the injury.
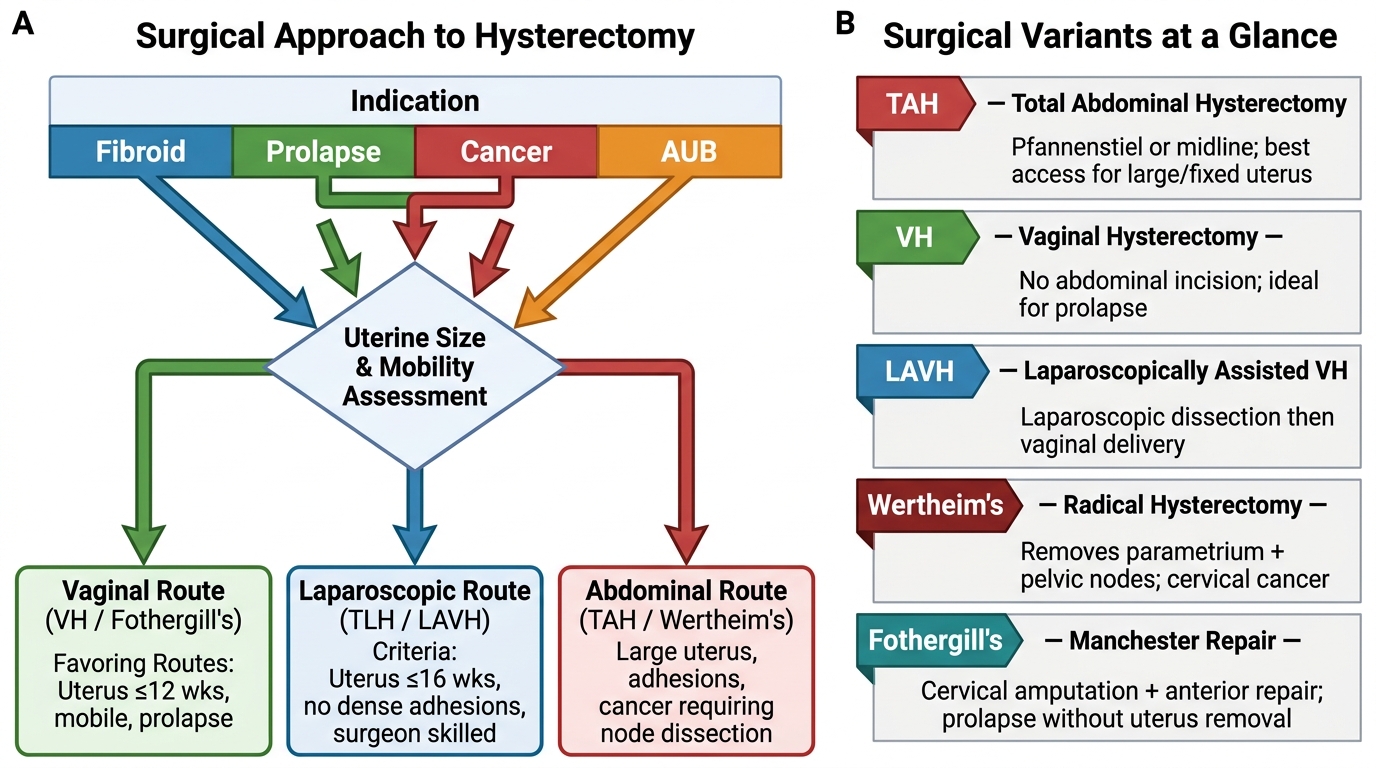
Decision Algorithm for Surgical Approach to Hysterectomy
SELF-CHECK
A woman undergoes laparoscopic salpingectomy for a right ectopic pregnancy. The Veress needle is inserted at the umbilicus and CO₂ insufflation begins. The insufflation pressure immediately reads 25 mmHg (normal <12 mmHg during initial filling). What does this indicate and what is the correct response?
A. Normal — the pressure always starts high and will fall as the cavity fills
B. The needle tip is in the preperitoneal space or against omentum/bowel, not free in the peritoneal cavity — stop insufflation, re-check needle position
C. Proceed — the high pressure will convert to normal once the gas distributes
D. Switch immediately to open (Hasson) entry without further checks
Reveal Answer
Answer: B. The needle tip is in the preperitoneal space or against omentum/bowel, not free in the peritoneal cavity — stop insufflation, re-check needle position
Initial insufflation pressure with a correctly placed Veress needle should be low (<8 mmHg) as CO₂ enters the free peritoneal cavity. A starting pressure of 25 mmHg indicates the needle tip is NOT in the free peritoneal space — it is likely in the preperitoneal space (subcutaneous fat), against omentum, or against bowel. Continuing insufflation in this position risks subcutaneous emphysema, bowel insufflation (potentially catastrophic), or gas embolism. The correct response is to stop, withdraw the needle, check the drop test, and re-position. Open Hasson entry is an alternative if multiple Veress attempts fail or are unsafe — but it is not mandatory after a single failed attempt.