Page 9 of 29
OG35.{7,9-10,14} | Communication, Ethics, Consent and Universal Precautions — SDL Guide
Learning Objectives
- Demonstrate effective interpersonal and communication skills when discussing illness, investigations, diagnosis, and outcomes with patients and their families in an OG context
- Apply the four principles of medical ethics and AETCOM competencies to clinical decision-making in obstetrics and gynaecology
- Obtain valid informed consent for any OG examination or procedure, including special-situation consent (sterilisation, MTP, minor, unconscious patient, emergency)
- Correctly select and use appropriate universal precautions and personal protective equipment in OG settings, and manage needle-stick or sharps injuries using the NACO PEP protocol
INSTRUCTIONS
Professional skills — communication, ethics, consent, and infection prevention — are the invisible infrastructure of every clinical encounter in obstetrics and gynaecology. A technically perfect caesarean section followed by poor communication about the indication can destroy the patient's trust and generate a complaint. An examination conducted without valid consent is legally an assault, regardless of clinical intent. A needle-stick injury mismanaged in the first hour can result in preventable HIV seroconversion. This module builds these four professional competencies systematically, from governing principles to supervised practice.
References
- Dutta DC. Textbook of Obstetrics. 10th ed. New Central Book Agency; 2023 (textbook)
- Shaw RW et al. Shaw's Textbook of Gynaecology. 17th ed. Elsevier; 2019 (textbook)
- NMC AETCOM Competencies for MBBS Programme. 2019 (guideline)
- NACO. Post Exposure Prophylaxis Guidelines. 2014 (guideline)
- WHO. Standard Precautions in Health Care. 2007 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Dr Priya, a senior resident, is about to perform an emergency caesarean section on Mrs Leela, a 26-year-old primigravida with fetal distress. She briefly says 'Sign here, we need to operate now' and hands over the consent form. Mrs Leela, frightened and in pain, signs without understanding what she has agreed to. Six hours later, her husband arrives and is furious: 'Nobody told us there would be a scar, a bladder risk, or that she might need ICU care.' The surgery was technically flawless. The clinical outcome was excellent. And yet the case became a formal complaint — because consent was a signature, not a conversation. In obstetrics and gynaecology, professional skills are not soft extras. They are the legal and ethical foundation on which every clinical act rests.
WHY THIS MATTERS
Obstetrics and gynaecology involves some of the most intimate and emotionally charged clinical encounters in medicine — pregnancy loss, infertility, sexual health, cancer, and the death of mothers and newborns. Communication failures in OG are disproportionately represented in medicolegal complaints: in India and globally, inadequate communication and deficient consent are the two most common grounds for complaints against obstetricians and gynaecologists. AETCOM competencies (OG35.7, OG35.9, OG35.10) and universal precautions (OG35.14) are assessed in OSCE, clinical assessment, viva voce, and skill assessment in your final examinations — and more importantly, they protect your patients and yourself every day in practice.
RECALL
Bring to mind what you already know from your AETCOM sessions and earlier clinical postings. What are the four classical principles of medical ethics as articulated by Beauchamp and Childress? What elements must be present for a consent to be legally valid — recall from your surgery and medicine postings. In community medicine you learned about standard precautions and the NACO PEP protocol. What does the chain of PPE donning look like? And from your communication training: what is SPIKES, and in what clinical context was it introduced? Hold these anchors as we build OG-specific applications on them.
Why Professional Skills Are the Bedrock of Safe OG Practice
Clinical competence in obstetrics and gynaecology rests on two inseparable pillars: technical skill and professional skill. Technical skill — the ability to perform a forceps delivery, diagnose placenta praevia on ultrasound, or manage postpartum haemorrhage — is visible, measurable, and taught intensively. Professional skill — the ability to communicate a devastating diagnosis, obtain genuine informed consent, act ethically in reproductive decision-making, and protect oneself and colleagues from blood-borne infection — is equally important but far less systematically taught. The consequences of professional-skill failure in OG are severe and often irreversible.
Communication failure in OG manifests in multiple ways: a patient who does not understand her diagnosis cannot participate in management decisions; a family excluded from a difficult conversation about a sick neonate becomes adversarial rather than supportive; a patient who never received her results fails to return for follow-up. In a country like India, where OG care spans an enormous range of literacy, language, and cultural contexts, communication skill is not a luxury — it is a competency gap with documented outcomes in maternal mortality.
Consent failure in OG is both a legal and an ethical problem. The Supreme Court of India has ruled clearly that medical examination or treatment without valid consent constitutes battery, even when clinically indicated. In reproductive health specifically — sterilisation, MTP, hysterectomy — the courts have imposed additional scrutiny on consent processes because these procedures permanently alter reproductive capacity.
Ethical failures in OG are among the most publicly visible in medicine. Forced sterilisation, sex-selective practices violating PCPNDT, and confidentiality breaches in HIV-positive pregnancies have all generated landmark legal and regulatory responses in India. The NMC AETCOM curriculum reflects the recognition that ethical behaviour must be taught, modelled, and assessed — not assumed.
Universal precautions exist because every patient must be treated as if they could be carrying a blood-borne pathogen. In OG, the exposure risk is high: deliveries, manual removal of placenta, sharp instruments, blood and amniotic fluid — all represent potential transmission vectors. A single needle-stick injury from an HIV-positive patient carries a transmission risk of approximately 0.3%. Without PEP initiated within 72 hours, that risk is unchangeable. With correct precautions, it is preventable.
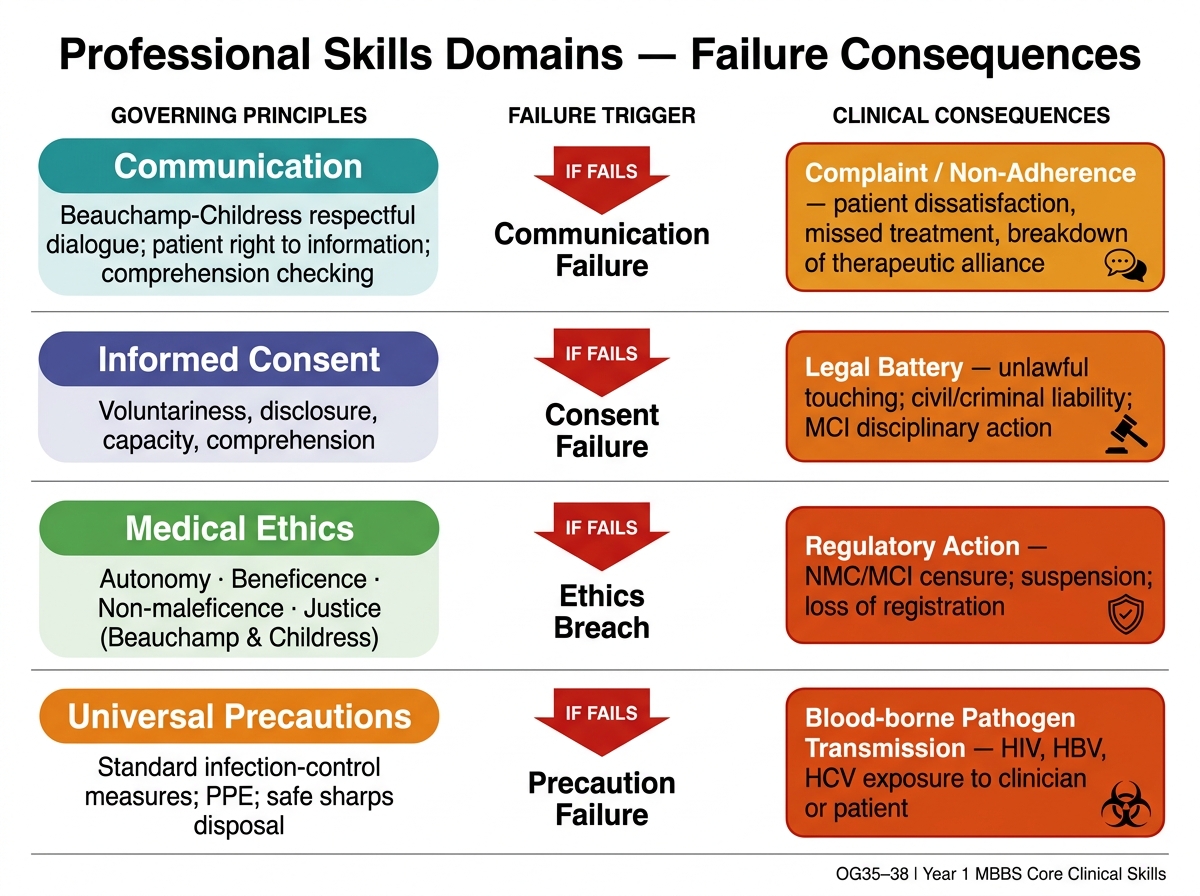
Professional Skills Domains and Consequences of Failure
Principles Governing Communication, Ethics, Consent and Precautions
Each of the four professional skills domains is governed by a distinct but overlapping set of principles. Understanding these principles before practising the techniques ensures that the techniques are applied with reasoning rather than rote.
Communication principles in clinical medicine draw on the Beauchamp-Childress model of respectful dialogue — acknowledging the patient's right to information, responding to emotional cues before providing information, checking comprehension, and ensuring that the content of the communication serves the patient's understanding rather than the clinician's convenience. In OG specifically, language barriers, health literacy, and the emotional weight of reproductive events demand a pace and register that differs from other clinical specialties.
Medical ethics in OG is governed by the four classical principles of Beauchamp and Childress:
| Principle | Meaning | OG Application |
|---|---|---|
| Autonomy | Respect the patient's right to decide for herself | Reproductive choices including contraception, MTP, sterilisation |
| Beneficence | Act in the patient's best interest | Recommending evidence-based treatment even when inconvenient |
| Non-maleficence | Do no harm | Avoiding unnecessary interventions; correct medication doses |
| Justice | Equitable treatment regardless of background | Equal care to BPL patients, migrant workers, sex workers |
Beyond these four pillars, the NMC AETCOM curriculum adds fidelity (keeping promises, maintaining trust), veracity (truthfulness even when difficult), and professional boundaries (avoiding dual relationships, maintaining appropriate limits of care).
Informed consent is governed by the principle that a patient has the right to determine what happens to her body (autonomy), which requires that she receive sufficient information to make a genuinely free and informed decision. The legal elements of valid consent in India are: (a) capacity — the patient is an adult (≥18 years) with decision-making ability; (b) disclosure — the clinician has explained the diagnosis, proposed procedure, risks, benefits, alternatives, and consequences of refusal in language the patient understands; (c) understanding — the patient has actually comprehended the information (not merely received it); (d) voluntariness — the decision is free from coercion or undue influence; (e) decision — the patient has actively consented or refused.
Standard precautions (the WHO 2007 revision of universal precautions) are a set of minimum infection-prevention measures applied to all patients regardless of their known infection status. They include: hand hygiene (the single most effective intervention), appropriate use of PPE (gloves, gown, mask, eye protection — selected based on anticipated exposure), safe sharps handling (never recap needles by hand; use a single-hand scoop technique or a sharps container), respiratory hygiene, and segregation of clinical waste.
SELF-CHECK
A 17-year-old unmarried girl presents for a termination of pregnancy at 10 weeks. She is alert, oriented, and clearly understands the procedure. Her parents are in the waiting area. Regarding consent, which statement is correct?
A. She cannot consent because she is a minor — her parents must sign
B. She can consent for herself under the MTP Act because she is the patient, but guardian consent is additionally required for minors
C. She can consent independently if she demonstrates capacity, but under Indian law guardian consent should also be obtained for minors in non-emergency situations
D. No consent is needed as termination up to 12 weeks is automatic
Reveal Answer
Answer: C. She can consent independently if she demonstrates capacity, but under Indian law guardian consent should also be obtained for minors in non-emergency situations
Under Indian law the legal age for independent consent is 18 years. Minors require guardian/parental consent alongside the patient's own assent where the patient is capable of understanding. The MTP Act 2021 specifically includes minors as a category eligible for termination up to 24 weeks, but does not override the guardian consent requirement for those under 18. Option C correctly reflects the need for both. Option A is an overstatement (the minor's own capacity and assent matter). Option D is incorrect — consent is always required.
Therapeutic Communication in Obstetrics and Gynaecology
Therapeutic communication in OG requires skills that go beyond the transmission of information. The goal is not merely to inform but to facilitate understanding, reduce anxiety, build trust, and enable the patient to participate actively in decisions about her care. This is particularly challenging in OG because many consultations involve emotionally loaded content — an abnormal scan result, a cancer diagnosis, a stillbirth, or a conversation about options following a complicated delivery. Research on communication in healthcare consistently shows that patients who understand their diagnosis and treatment plan are more adherent to follow-up, more likely to disclose symptoms early, and more likely to return to care — all of which translate into better clinical outcomes. Conversely, patients who feel dismissed or poorly informed after a difficult consultation are more likely to experience psychological harm, delayed decision-making, and disengagement from the healthcare system. In OG, where decisions about reproduction, fertility, and life-threatening conditions frequently intersect, the quality of communication is inseparable from the quality of care itself.
The SPIKES protocol, originally developed for oncology but now widely applied in OG, provides a structured framework for breaking bad news and conducting difficult conversations:
- S — Setting: Choose a private, quiet space. Ensure the right people are present (the patient decides who). Sit at eye level. Turn off interruptions.
- P — Perception: Before giving information, ask what the patient already knows or suspects. 'What have you been told so far about your ultrasound results?' This prevents information overload and reveals the patient's baseline.
- I — Invitation: Ask how much information the patient wants and how she would like to receive it. 'Would you like me to explain the findings in detail, or would you prefer I give you the key summary first?'
- K — Knowledge: Deliver information in small steps, using plain language. Avoid jargon. Pause frequently to check understanding. 'I'm going to tell you something difficult. Your scan shows that...' Deliver the headline, then pause.
- E — Empathy: Acknowledge and name the emotion you observe. 'I can see this is very distressing for you. It's completely understandable to feel this way.' Do not move on until the emotional response has been acknowledged.
- S — Strategy and Summary: Provide a clear plan. Summarise what has been decided. Offer a follow-up appointment. Give written information where available. 'What we'll do next is...'
In OG-specific contexts, the following communication challenges require additional skill:
Perinatal loss: a miscarriage, stillbirth, or neonatal death requires the clinician to acknowledge the baby by name if one has been given, offer to see the baby together with the parents if they wish, and avoid phrases like 'at least you can try again' (which minimise the loss).
Genetic or congenital abnormality: a diagnosis of fetal anomaly on morphology scan requires careful explanation of the finding, what it means for the baby's health, the available management options (including continuation and termination within legal limits), and time for the parents to process before being asked to make decisions.
Communication with the family: in many Indian cultural contexts, families (especially husbands and in-laws) expect to be involved in medical decisions about a woman's care. The clinician must respect this cultural norm while also ensuring that the patient's own voice and autonomy are protected. The patient's preferences about what is shared with whom must be established first, in a private consultation.
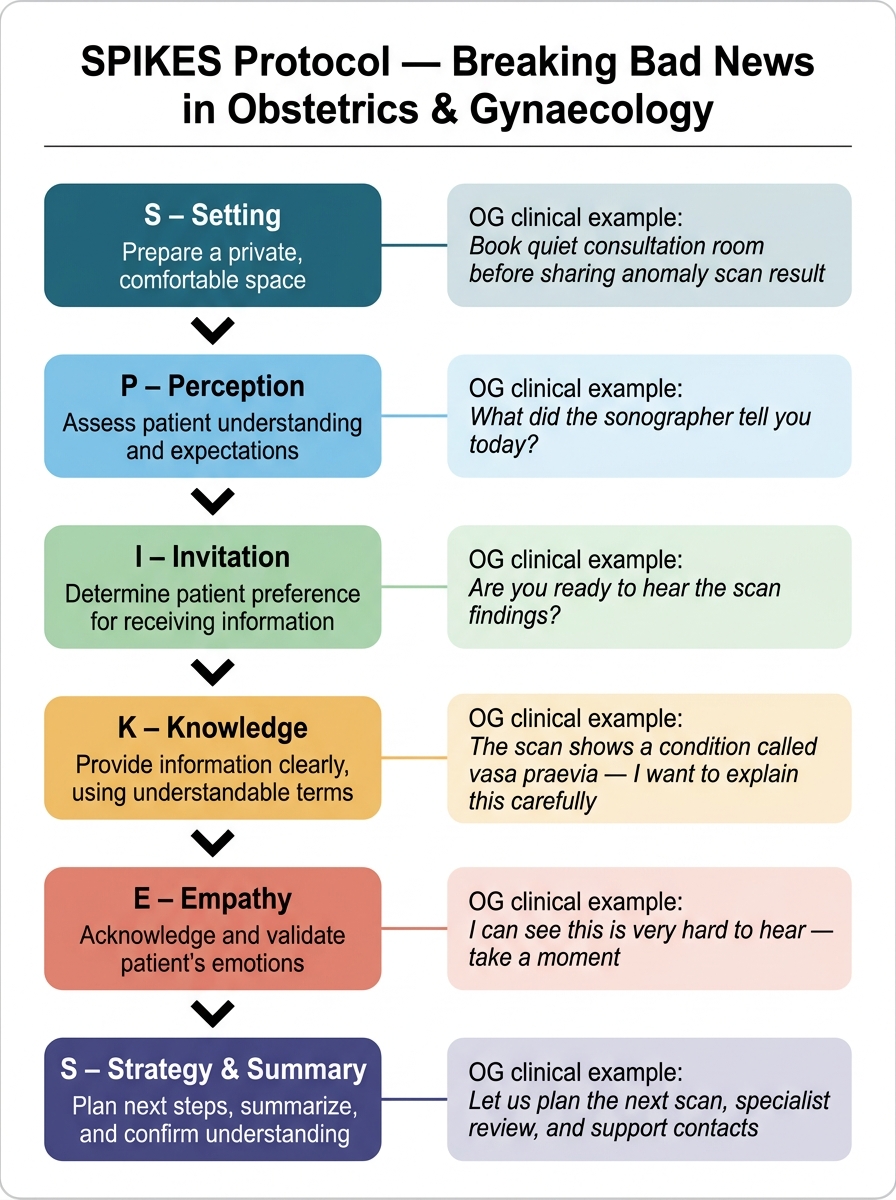
SPIKES Protocol for Breaking Bad News — Obstetrics & Gynaecology Examples