Page 6 of 29
OG35.12-13,OG38.4 | Discharge, Referral and Medical Certification — SDL Guide (Part 2)
Writing a Referral Letter: Components and Urgency Grading
A referral letter is a professional-to-professional communication that transfers clinical responsibility (partially or fully) from one provider to another — either to a specialist colleague at the same facility or to a secondary or tertiary centre. In obstetrics and gynaecology, referrals are an essential safety mechanism: the ability to recognise a case exceeding one's clinical capacity and communicate it clearly can be life-saving.
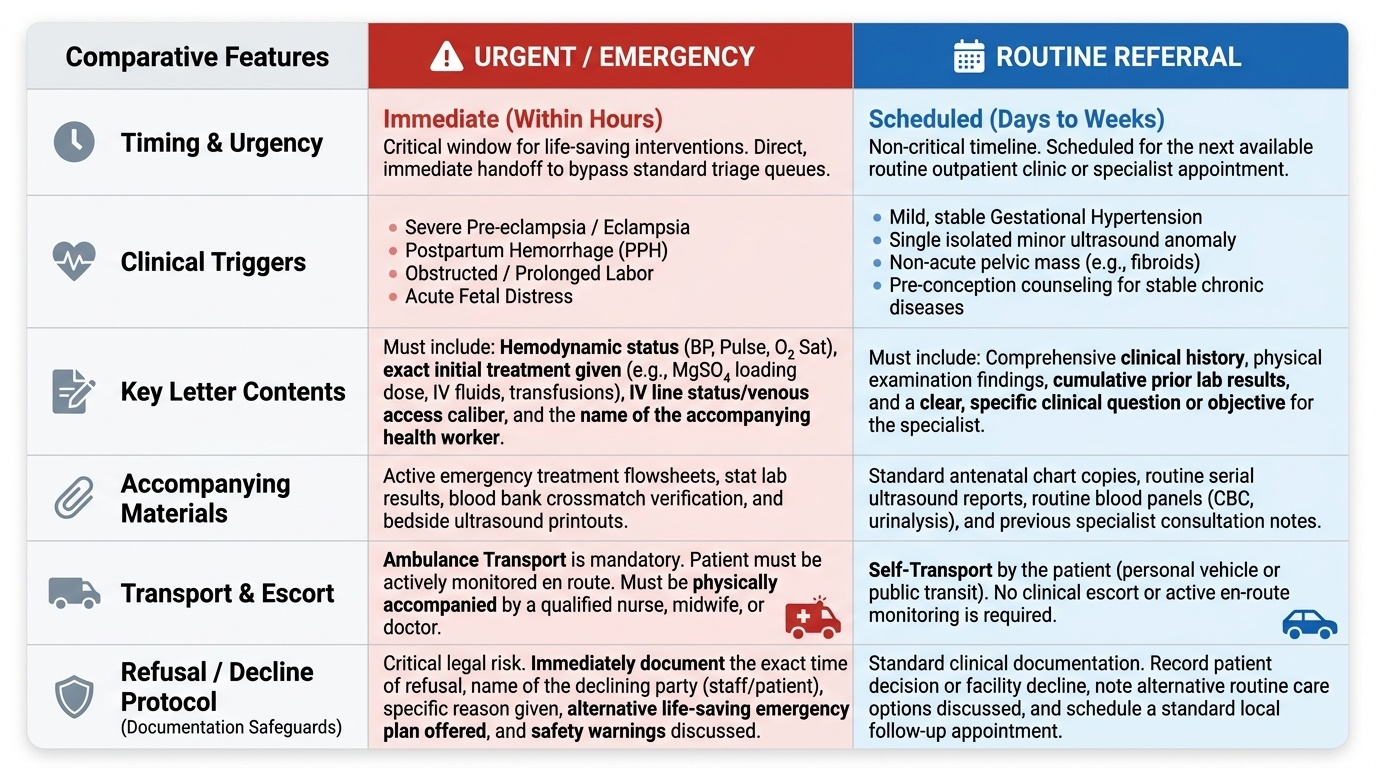
A referral letter in OG has five mandatory components. First is patient identification: full name, age, parity, gestational age (if pregnant), hospital number, and the referring doctor's name, designation, and facility. Second is the reason for referral: one or two sentences stating clearly why the patient is being referred — the clinical problem, what has been done so far, and what specific input is needed from the receiving centre. Third is the clinical summary: relevant history, examination findings, and investigation results — concise but complete. The receiving doctor must be able to make an independent assessment from the letter alone. Fourth is urgency grading: is this an emergency, urgent (within hours), semi-urgent (within 24-48 hours), or routine (can wait for a scheduled appointment)? This single piece of information determines how the receiving facility allocates resources. An eclamptic patient transferred without any urgency marking may wait in a triage queue. Fifth is accompanying materials: attach photocopies of the investigation results, ECG, ultrasound report, or blood bank crossmatch where relevant. State explicitly what documents accompany the patient.
For obstetric emergencies, the referral letter must also include: the haemodynamic status at the time of referral (blood pressure, pulse rate, oxygen saturation), what initial treatment has been given (IV fluids, MgSO₄ loading dose, blood transfusion), the IV line status and venous access, and the name of the accompanying health worker or attendant.
A separate but important situation is when referral is declined by the receiving facility or refused by the patient. Both must be documented: note the time and name of the person refusing or declining, the reason given, and the alternative plan offered. This documentation protects both the patient and the clinician.
Provided image
Medical Certificates in Obstetrics and Gynaecology Practice
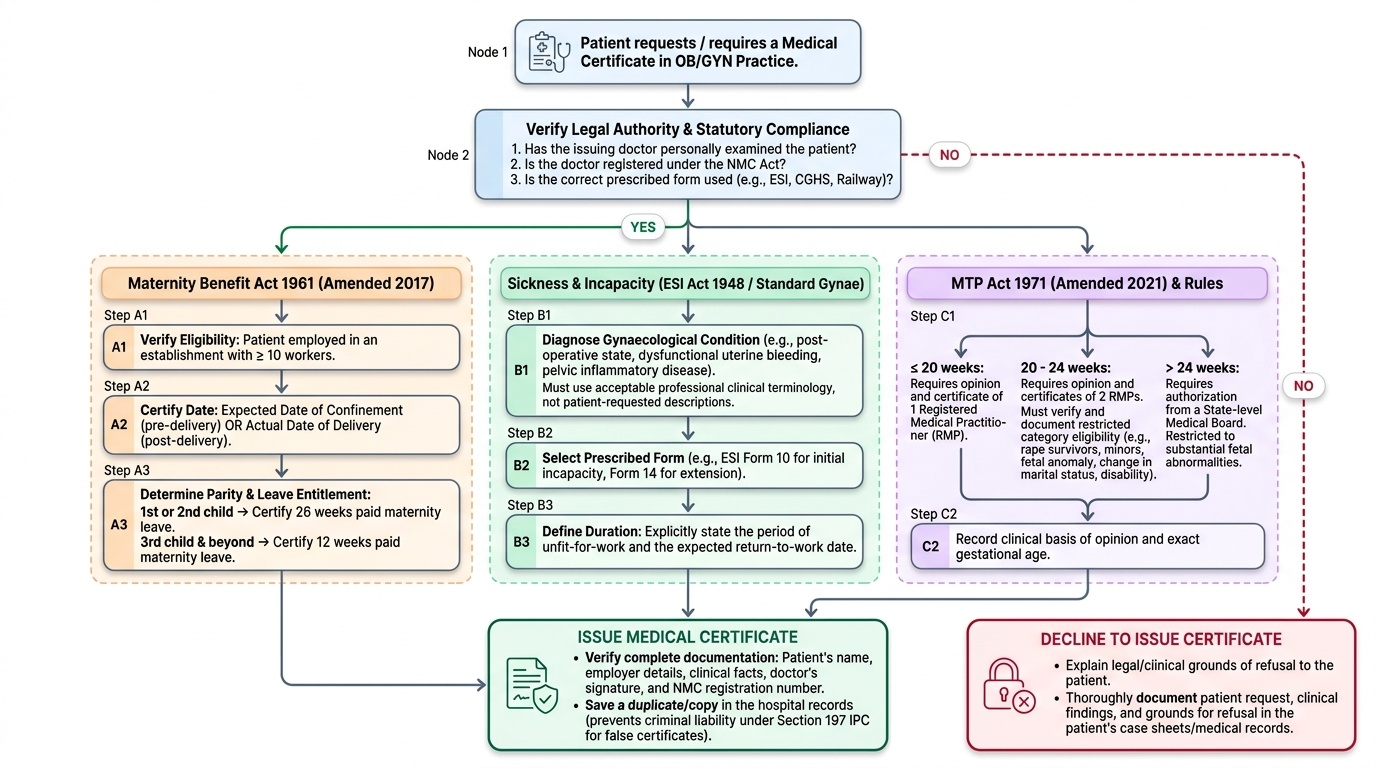
A medical certificate is a legal document signed by a registered medical practitioner that attests to a clinical fact for a defined official purpose. Unlike a discharge summary or referral letter, it has statutory requirements — the issuing doctor must have personally examined the patient, must be registered under the NMC Act, and where a prescribed form exists (ESI, CGHS, railway, insurance), that specific form must be used. Issuing a false certificate is a criminal offence under Section 197 of the Indian Penal Code and a ground for NMC disciplinary action.
In obstetrics and gynaecology practice, the following categories of medical certificates are commonly required:
Maternity certificate: issued under the Maternity Benefit Act 1961 (amended 2017). Any woman employed in an establishment with ≥10 workers is entitled to maternity benefit. The attending doctor certifies the expected date of confinement (before delivery) or the actual date of delivery (after delivery). This enables the woman to claim the 26-week paid maternity leave (for the first two surviving children; 12 weeks for the third child and beyond). The certificate must state: patient's name, employer, expected/actual date of delivery, and the examining doctor's registration number.
Sickness and incapacity certificate: certifies that the patient is unfit for work for a specified period due to a gynaecological condition (post-operative, dysfunctional uterine bleeding, pelvic inflammatory disease). Under the ESI Act 1948, this is issued on the prescribed Form 10 (initial) or Form 14 (extension). It must state diagnosis (using acceptable clinical terminology, not a label the patient has requested), duration of incapacity, and the expected return-to-work date.
MTP certification: under the MTP Act 1971 amended 2021 and MTP Rules 2021, a certificate of opinion is required from at least one registered medical practitioner for termination up to 20 weeks; from two registered medical practitioners for 20–24 weeks (restricted to specified categories: survivors of rape/incest, minors, foetal anomaly, change in marital status, physical/mental disability, emergency); and from a State-level Medical Board for substantial foetal abnormality beyond 24 weeks. The certificate must record the gestational age, the clinical basis for the opinion, the ground under which termination is authorised, and the registration number of the issuing practitioner.
Fitness certificate: certifies that a patient is fit to resume work, travel, sport, or a specific activity after an OG procedure or illness. Must be grounded in a documented examination on that date.
Birth and death certificates: a birth certificate attests to a live birth in a healthcare facility; a death certificate certifies cause of death. Both are statutory under the Registration of Births and Deaths Act 1969. Maternal and neonatal deaths have additional requirements under the facility-based maternal death review (MDR) process — a separate internal review form must be completed within 24 hours.
The overarching rule for all medical certificates: examine first, certify based only on what you find, and never backdate or antedate.
Provided image
SELF-CHECK
A second-year MBBS student is attached to the postnatal ward. A woman asks the student to sign a maternity benefit certificate for her employer so she can start her leave. The student knows the clinical facts from the notes and fills in the form accurately. Is this appropriate?
A. Yes, because the student has access to accurate clinical information
B. Yes, if a registered doctor countersigns within 24 hours
C. No, because medical certificates must be signed by a registered medical practitioner after personally examining the patient
D. No, because maternity certificates must be issued by a gynaecologist specifically
Reveal Answer
Answer: C. No, because medical certificates must be signed by a registered medical practitioner after personally examining the patient
A medical certificate is a legal document that can only be signed by a registered medical practitioner (registered under the NMC Act or its predecessor). An MBBS student is not registered and cannot issue a certificate regardless of accuracy. Only an MBBS or higher-degree holder with NMC registration may sign. Additionally, the issuing doctor must have personally examined the patient — reliance on notes alone is insufficient.
Reading and Acting on a Received Document
Interpreting incoming clinical documents is the mirror skill to writing them, and in daily OG practice you will receive discharge summaries and referral letters as often as you write them. The ability to read these documents critically — identifying gaps, red flags, and actionable information — is equally important to patient safety.
When you receive a referral letter, the first task is urgency triage: is this an emergency or a routine referral? An eclamptic patient transferred from a primary centre must bypass ordinary triage queues and go directly to the labour ward. A 'referral for elevated BP in third trimester' needs assessment in the obstetric outpatient department. The urgency grading in the referral letter should guide this, but if it is absent or ambiguous, the clinical facts in the letter must guide your decision. Do not wait for paperwork to be complete before stabilising an acutely unwell patient.
Next, identify information gaps: what investigations were done, and are the results attached? Is the gestational age clearly stated? Has the patient received any treatment, and if so, what dose and when? In obstetric emergencies, the time of the last MgSO₄ loading dose is critical before re-dosing — if this is not in the referral letter, call the sending facility immediately.
For received discharge summaries (when a patient presents to your unit with a previous discharge summary from elsewhere), extract: the final diagnosis, any ongoing medications and doses, follow-up targets, and any red-flag conditions documented during the prior admission. This prevents both duplication and dangerous omission.
Finally, document what you have done with the information: 'Referral letter received from Dr X, [facility], dated [date]. Patient assessed and admitted to labour ward on the basis of [clinical grounds]. Referral letter filed in case record.' This closes the documentation loop and creates a medicolegal record that the referral was acted upon appropriately.
CLINICAL PEARL
The three most commonly litigated documentation failures in Indian OG practice are: (1) a discharge summary that does not list medication doses — the family gives the wrong dose and the patient is readmitted; (2) a referral letter with no urgency grading — the receiving triage nurse treats an eclamptic patient as a routine referral; and (3) a medical certificate signed by a doctor who did not personally examine the patient on that date — invalid in law and a disciplinary matter. Internalize these three failure modes before you touch a pen in the ward.