Page 14 of 29
OG35.4-6 | Focused Gynaecological Case Approach — SDL Guide (Part 2)
Case 2 — Vaginal Discharge: Examination, Differential, and Management
Vaginal discharge is one of the most common presenting complaints in gynaecology OPD. The structured approach must first distinguish physiological discharge — clear or white, non-offensive, non-itchy, mid-cycle or premenstrual, related to ovulation or sexual arousal — from pathological discharge, which is characterised by a change in colour, odour, consistency, or the presence of associated symptoms (itching, burning, dyspareunia, pelvic pain, post-coital bleeding).
The history for vaginal discharge must specifically cover: duration and onset; colour (white-grey, yellow-green, thick white/curdy); odour (fishy/amine-like in BV; no specific odour in candidiasis); consistency (homogeneous in BV; frothy in trichomonas; curdy/cottage-cheese in candidiasis); associated symptoms (vulval itching = candidiasis; dysuria = trichomoniasis; pelvic pain = PID); recent antibiotic use (precipitates candidiasis); sexual history and partner symptoms; pregnancy status; and previous STI.
On speculum examination, the vaginal walls reveal the discharge type: grey-white homogeneous coating adherent to walls in bacterial vaginosis (BV); frothy yellow-green pooling in the posterior fornix with 'strawberry cervix' (colpitis macularis) in Trichomonas vaginalis; thick white curdy plaques on the vaginal walls with surrounding erythema in Candida albicans; mucopurulent cervical discharge from the os in cervicitis (Chlamydia, Gonorrhoea).
The bedside investigations for vaginal discharge include:
- Vaginal pH (normal ≤4.5): elevated >4.5 in BV and trichomonas; normal in candidiasis
- Whiff test (amine test): add 10% KOH to discharge — a fishy amine odour is positive in BV and trichomonas
- Wet mount microscopy: saline wet mount — clue cells (squamous epithelial cells studded with coccobacilli, >20% = BV by Amsel criteria); motile trichomonads (pear-shaped flagellate protozoa, larger than WBCs); KOH preparation — pseudohyphae and budding yeast cells = Candida
- Culture and sensitivity: for suspected gonorrhoea (Thayer-Martin medium), chlamydia (NAAT/PCR preferred)
Management is pathogen-specific:
- BV: metronidazole 400 mg orally twice daily for 7 days, or metronidazole 0.75% vaginal gel for 5 days
- Candidiasis: topical clotrimazole pessary 500 mg single dose, or oral fluconazole 150 mg single dose
- Trichomoniasis: metronidazole 2 g oral single dose (both partners must be treated)
- Cervicitis (Chlamydia): azithromycin 1 g single dose, or doxycycline 100 mg twice daily for 7 days
- Cervicitis (Gonorrhoea): ceftriaxone 500 mg IM single dose per WHO 2021 guidelines
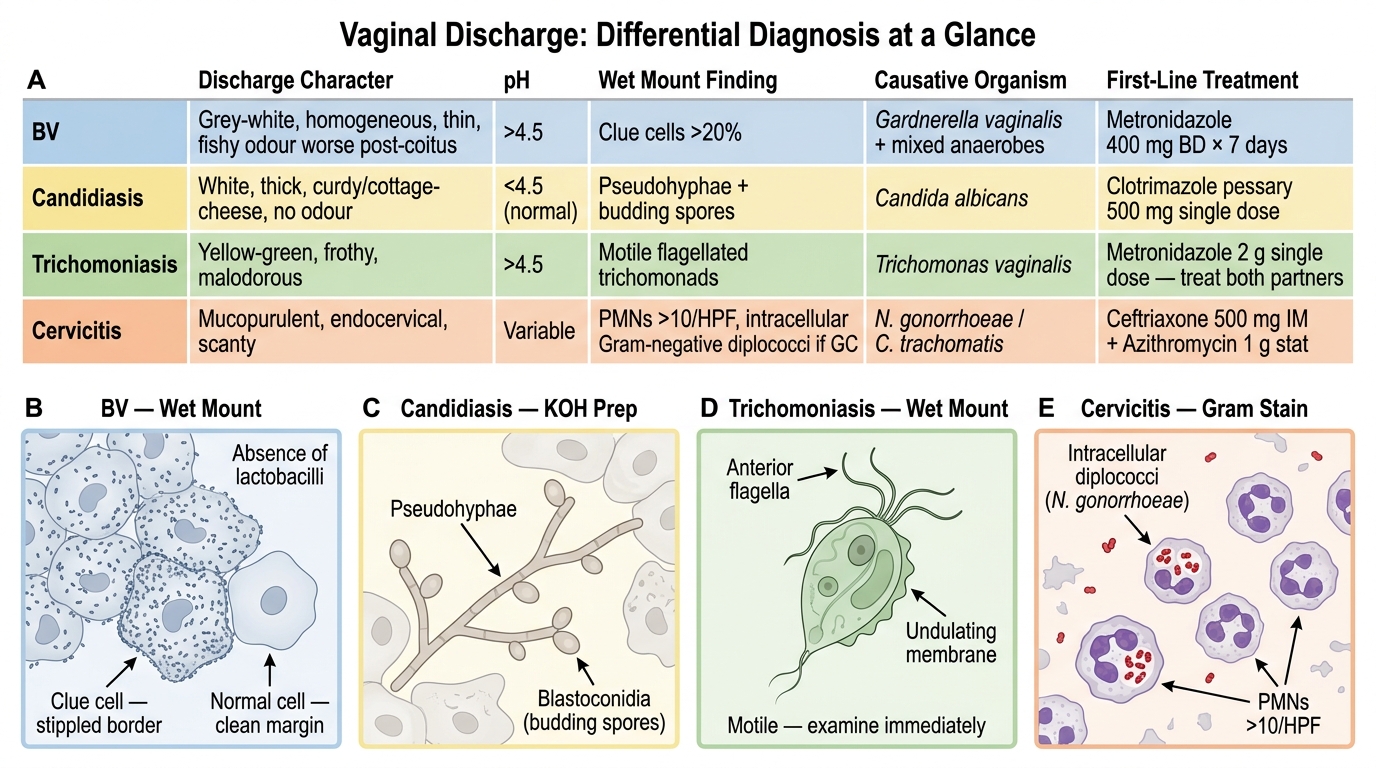
Vaginal Discharge: Differential Diagnosis and Microscopy Correlation
SELF-CHECK
A 24-year-old woman presents with 2 weeks of grey-white vaginal discharge with a strong fishy odour, worsened after sexual intercourse. On speculum the discharge is homogeneous and coats the vaginal walls. Vaginal pH is 5.2. Wet mount shows >20% clue cells. What is the diagnosis and the correct first-line treatment?
A. Candidiasis; clotrimazole pessary 500 mg
B. Trichomonas vaginalis; metronidazole 2 g single dose to both partners
C. Bacterial vaginosis; metronidazole 400 mg twice daily for 7 days
D. Chlamydial cervicitis; azithromycin 1 g single dose
Reveal Answer
Answer: C. Bacterial vaginosis; metronidazole 400 mg twice daily for 7 days
The presentation — grey-white homogeneous discharge, fishy odour worse after intercourse, pH >4.5, and >20% clue cells on wet mount — meets all four Amsel criteria for bacterial vaginosis. The causative organism is Gardnerella vaginalis and mixed anaerobes. First-line treatment is metronidazole 400 mg orally twice daily for 7 days. Unlike trichomoniasis, partner treatment is not routinely recommended for BV. Candidiasis has normal pH and curdy discharge without clue cells.
Case 3 — Genital Ulcers: Examination, Differential, and Management
Genital ulcers in a woman presenting to the gynaecology OPD require a structured approach that characterises the ulcer precisely, constructs a focused differential based on clinical features, and selects investigations that confirm the aetiology — or applies syndromic management when laboratory confirmation is not available.
The history for genital ulcers must cover: duration; single versus multiple ulcers; pain (a key discriminating feature — syphilitic chancres are classically painless, herpetic ulcers are markedly painful, chancroid ulcers are very painful, LGV primary lesions are painless); systemic symptoms (fever, malaise, rash — suggests HSV or secondary syphilis); lymphadenopathy (painful tender lymphadenopathy = chancroid; painless rubbery lymphadenopathy = syphilis; painful fluctuant inguinal buboes = LGV); sexual history (number of partners, recent partner change, condom use); and HIV status.
On examination, characterise the ulcer using these features:
- Number: single (primary syphilis, chancroid) vs multiple (herpes, secondary syphilis)
- Pain: painless = syphilis, LGV primary lesion, granuloma inguinale; painful = herpes, chancroid
- Base: clean granulomatous base (syphilis); necrotic/dirty base (chancroid); raised beefy-red base (donovanosis)
- Edge: indurated, rolled edge (syphilis); undermined, ragged edge (chancroid); rolled/raised edge (donovanosis)
- Associated features: grouped vesicles progressing to shallow ulcers = herpes; satellite ulcers = chancroid; Donovan bodies on smear = granuloma inguinale
The differential diagnosis of genital ulcers:
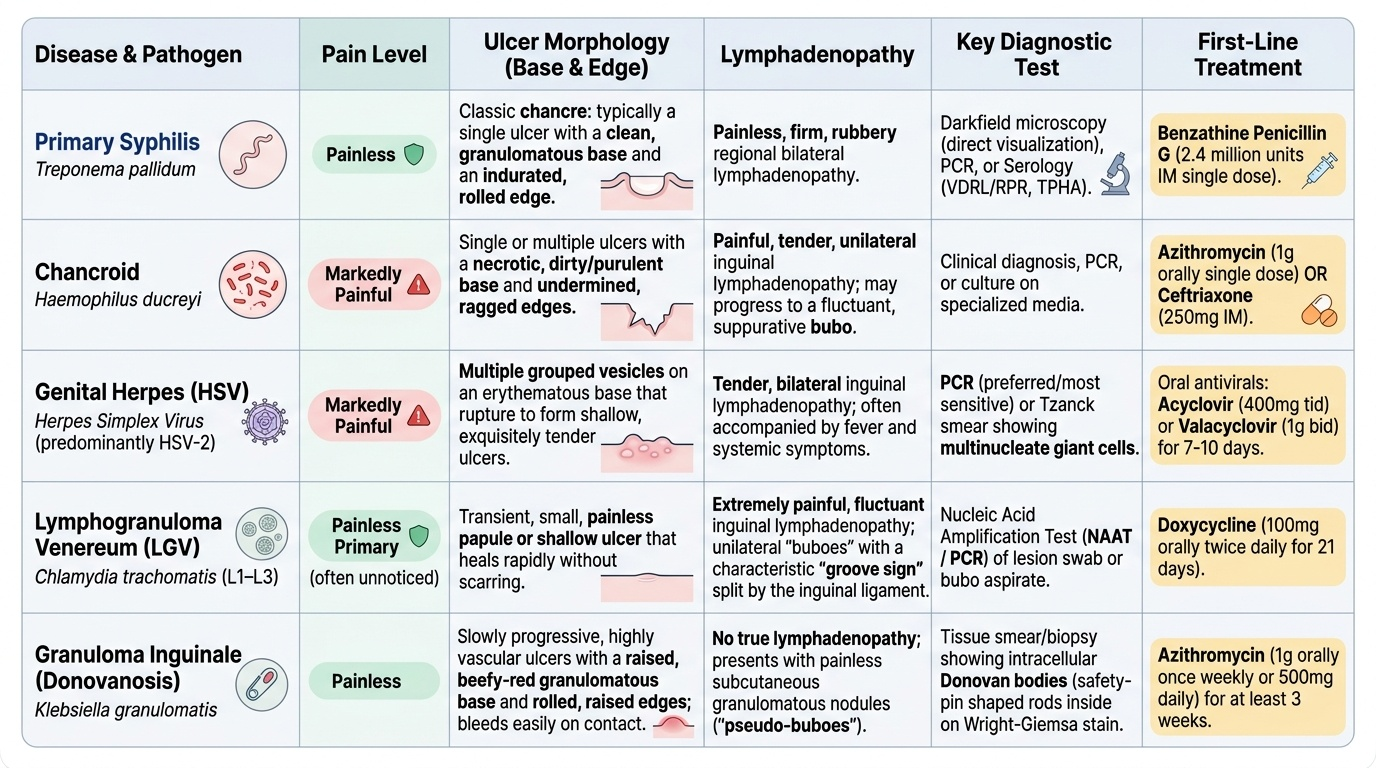
- Primary syphilis (Treponema pallidum): single, painless, indurated chancre with firm rolled edge; painless regional lymphadenopathy; VDRL may be negative in the first 4–6 weeks, TPHA positive earlier
- Chancroid (Haemophilus ducreyi): single or multiple, very painful, soft ulcer with undermined edges; unilateral tender inguinal lymphadenopathy (may suppurate)
- Genital herpes (HSV-2 predominantly): multiple grouped vesicles progressing to shallow painful ulcers; may be bilateral; tender inguinal lymphadenopathy; Tzanck smear shows multinucleate giant cells
- Lymphogranuloma venereum (Chlamydia trachomatis L1–L3 serovars): transient painless papule or ulcer at the primary site (often missed); followed by painful inguinal buboes — the 'groove sign' (a groove between nodes above and below the inguinal ligament) is characteristic
- Granuloma inguinale / Donovanosis (Klebsiella granulomatis): painless, progressive, beefy-red ulcer with rolled edges; no lymphadenopathy; Donovan bodies (Giemsa or silver stain of tissue smear) are pathognomonic
Investigations: dark-field microscopy for Treponema pallidum (fresh ulcer exudate, requires motile organisms); VDRL + TPHA for syphilis serology; HSV PCR or viral culture; Tzanck smear (HSV — quick bedside test, low sensitivity); Giemsa-stained smear for Donovan bodies.
Management:
- Syphilis: benzathine penicillin G 2.4 million IU IM single dose (primary/secondary); treat partner
- Chancroid: azithromycin 1 g single dose or ceftriaxone 250 mg IM single dose
- Herpes: acyclovir 400 mg three times daily for 7–10 days (primary episode)
- LGV: doxycycline 100 mg twice daily for 21 days
- Granuloma inguinale: azithromycin 1 g weekly (or 500 mg daily) for ≥3 weeks until lesion heals
- Syndromic management (when laboratory unavailable): treat for both syphilis AND chancroid simultaneously
Provided image
Interpreting Clinical Findings: Pattern Recognition and Differential Refinement
Clinical pattern recognition in gynaecology is the skill of integrating history, examination, and investigation findings into a coherent diagnostic impression — and knowing when to revise that impression. This requires not just knowledge of individual disease features, but an understanding of how features combine and how common findings interact with uncommon ones.
For pelvic masses, the key interpretive step is distinguishing benign from potentially malignant. Features that increase the likelihood of malignancy in an adnexal mass include: post-menopausal age; bilateral masses; irregular solid or mixed (solid-cystic) ultrasound appearance; associated ascites; elevated CA-125 in the post-menopausal context; constitutional symptoms (weight loss, anorexia); fixed, non-mobile mass on bimanual examination. None of these features is individually diagnostic, but their combination generates a risk profile. The IOTA M-rules (malignancy rules) provide a validated ultrasound framework: ascites, at least four papillary projections, irregular solid tumour, and solid component in multilocular-solid tumour >10 cm each constitute an M-rule; presence of any M-rule without B-rule = refer for specialist surgical oncology assessment.
For vaginal discharge, the important interpretive challenge is not missing a concurrent cervical pathology. When Amsel criteria confirm BV or when candidiasis is evident on wet mount, the clinician should still inspect the cervix for post-coital bleeding, friability, or suspicious lesions — because a coincidental cervical carcinoma can be masked by the symptomatic discharge. Similarly, in trichomoniasis, the classic strawberry cervix (colpitis macularis) is visible to the naked eye in fewer than 10% of cases despite being pathognomonic when seen — so the absence of a strawberry cervix does not exclude trichomonas.
For genital ulcers, the critical interpretive principle is that co-infection is common. A patient with a painful ulcer may have both herpes and secondary syphilis. In endemic areas (sub-Saharan Africa and parts of India), any genital ulcer should prompt HIV testing because genital ulcer disease is a recognised facilitator of HIV transmission and acquisition. When the ulcer does not fit a classic pattern, consider Behcet's disease (painful oral and genital ulcers, uveitis, skin lesions) and fixed drug eruption as non-infectious causes.
Red flags requiring urgent referral: a pelvic mass with ascites and constitutional symptoms in a post-menopausal woman; a friable bleeding cervical mass; a non-healing ulcer that has been treated appropriately without response (may indicate squamous cell carcinoma of the vulva masquerading as a chronic ulcer).
CLINICAL PEARL
Three bedside rules that sharpen the gynaecological differential without investigations: (1) Always catheterise before diagnosing a pelvic mass — a full bladder is the most common 'pelvic mass' seen in a busy OPD. (2) In vaginal discharge, pH and a wet mount together give a diagnosis in more than 70% of cases — do not wait for culture results to start treatment. (3) For genital ulcers, painful = herpes or chancroid; painless = syphilis or LGV primary lesion — this single parameter narrows the differential to one or two diagnoses before serology returns.