Page 5 of 20
OG35.{16-17,20} | ARM, Episiotomy Suturing and Urinary Catheterisation — SDL Guide
Learning Objectives
- Demonstrate the correct technique to perform artificial rupture of membranes (ARM/amniotomy) in a simulated or supervised environment (OG35.16)
- Demonstrate the correct technique to perform and suture episiotomies in a simulated or supervised environment (OG35.17)
- Demonstrate the correct technique of urinary catheterisation in a simulated or supervised environment (OG35.20)
- Recognise the indications and contraindications for each procedure and select the appropriate technique
- Identify and manage immediate complications of each procedure, including cord prolapse after ARM and perineal haematoma after episiotomy repair
INSTRUCTIONS
Three fundamental intrapartum and peripartum procedures — artificial rupture of membranes, episiotomy suturing, and urinary catheterisation — are among the most commonly performed obstetric skills in any labour ward. Each requires precise anatomical knowledge, a clear understanding of indications and contraindications, and a disciplined aseptic technique. Errors in any one of these procedures can have serious consequences: cord prolapse after ARM, perineal haematoma from inadequate suturing, and catheter-associated urinary tract infection from poor asepsis. This module builds your procedural knowledge and simulation-ready technique for all three skills.
References
- DC Dutta's Textbook of Obstetrics, 10th ed. Ch. 11 — Normal Labour; Ch. 13 — Management of Normal Labour (textbook)
- Williams Obstetrics, 26th ed. Ch. 22 — Normal Labour; Ch. 27 — Episiotomy (textbook)
- WHO Recommendations: Intrapartum Care for a Positive Childbirth Experience, 2018 (guideline)
- Cochrane Review: Episiotomy for vaginal birth — Carroli G, Mignini L, 2008 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A primigravida at 40 weeks of gestation has been in active labour for 8 hours. The cervix is 8 cm dilated with intact membranes and the fetal head at station 0. The partograph shows that progress has slowed over the last 2 hours without crossing the action line. The registrar asks you to perform an ARM. As you prepare, you notice the fetal head is not fully engaged on the last examination. Before you proceed, you should ask yourself: is the head well-applied to the cervix, or is there a risk of cord prolapse? Could the liquor be meconium-stained, and what would that mean for the plan? Two minutes later, the baby's heart rate drops to 80 bpm immediately after you perform the ARM. Cord prolapse is the emergency you must now manage — it began with a decision to proceed despite an incompletely engaged head.
WHY THIS MATTERS
Artificial rupture of membranes, episiotomy suturing, and urinary catheterisation are not merely technical skills — they are clinical decisions wrapped in procedural steps. ARM can accelerate labour but risks cord prolapse; an episiotomy protects the perineum from ragged tearing in selected situations but is not routine; urinary catheterisation is essential for intraoperative monitoring and postpartum retention, but each unnecessary catheterisation risks a catheter-associated urinary tract infection (CAUTI), the most common healthcare-associated infection. As a final-year student rotating through the labour ward, you will assist with or perform these procedures under supervision. Understanding when, how, and how not to perform each of them distinguishes competent care from potentially harmful care.
RECALL
Recall these anatomical and physiological foundations before proceeding. The fetal membranes consist of an outer chorion (derived from trophoblast) and inner amnion (derived from epiblast), together forming the amniochorionic membrane that contains amniotic fluid. At term, the membranes are typically continuous with the cervical margin; they may bulge through the os when intact. Normal liquor is clear or straw-coloured; meconium-stained liquor indicates fetal distress. The perineum refers to the diamond-shaped region between the pubic symphysis and coccyx; the perineal body is the central fibromuscular mass where multiple perineal muscles converge. The female urethra is approximately 3-4 cm long, opening anteriorly at the urethral meatus between the clitoris and vaginal opening. The external anal sphincter (EAS) lies posteriorly to the vaginal introitus; damage to it constitutes a third-degree perineal tear, which must be identified and repaired by a senior clinician.
Clinical Indications and Decision-Making for Each Procedure
Each of these three procedures has specific indications that must be satisfied before proceeding, and each has important contraindications or prerequisites that must be confirmed. The decision to perform any of them in the labour ward requires clinical judgment, not just mechanical capability.
Artificial Rupture of Membranes (ARM): The primary indications for ARM are: augmentation of slow or arrested labour in active phase (cervix ≥3 cm, head engaged or at station 0 or below, no contraindication); induction of labour (as an adjunct to oxytocin); assessment of liquor colour (to detect meconium staining indicative of fetal distress); application of a fetal scalp electrode for continuous CTG monitoring. The absolute contraindications to ARM include: unengaged fetal head (the head must be firmly applied to the lower uterine segment, preventing cord slip); known vasa praevia (risk of fatal fetal haemorrhage); placenta praevia; umbilical cord presentation (on examination); active genital herpes infection. The key safety prerequisite is that the fetal head must be well engaged and firmly applied to the cervix to prevent the cord from slipping past the head into the lower birth canal after fluid drains.
Episiotomy: The WHO (2018) and Cochrane evidence (Carroli 2008) strongly support selective rather than routine episiotomy. Selective indications include: imminent severe perineal tear (perineum taut, tissue thinning and blanching, head advancing rapidly in a primigravida with tight perineum); instrumental delivery (forceps or ventouse, where additional space reduces the risk of sphincter damage); shoulder dystocia (to facilitate additional obstetric manoeuvres); preterm delivery (to shorten the second stage and protect the preterm head); and fetal distress requiring rapid delivery. Episiotomy is not indicated as a routine preventive measure and does not prevent incontinence. It is a deliberate incision and must be repaired correctly.
Urinary catheterisation in obstetrics: Indications include: continuous intraoperative bladder drainage during caesarean section or perineal/vaginal repair; epidural analgesia (inability to void voluntarily); postpartum urinary retention (inability to void spontaneously for ≥6 hours after vaginal delivery, or ≥4 hours after catheter removal post-LSCS); monitoring of urine output in severe pre-eclampsia, PPH, or any shocked patient (requires an indwelling Foley catheter for accurate hourly output). Catheterisation is not without risk — CAUTI is the most common healthcare-associated infection in hospitalised patients; each day of unnecessary catheterisation increases infection risk, and catheters must be removed at the earliest clinically appropriate time.
Relevant Anatomy: Perineum and Lower Urinary Tract
Precise anatomical knowledge of the perineum and lower urinary tract directly determines the safety and effectiveness of episiotomy and catheterisation. The perineum is bounded anteriorly by the pubic symphysis, posteriorly by the coccyx, and laterally by the ischial tuberosities; it is divided into the urogenital triangle anteriorly and the anal triangle posteriorly. The perineal body — the central fibromuscular landmark — receives the insertions of the bulbospongiosus (bulbocavernosus), superficial and deep transverse perinei, external anal sphincter, and pubococcygeus; damage to the perineal body during delivery weakens pelvic floor support and risks both anal and urinary incontinence.
The episiotomy incision is made through specific tissue layers. From superficial to deep, the layers of the posterior perineum are: (1) skin and subcutaneous fat; (2) bulbospongiosus (bulbocavernosus) muscle; (3) superficial transverse perineal muscle; (4) deep transverse perineal muscle (part of the urogenital diaphragm); (5) fascia and connective tissue. The external anal sphincter (EAS) lies between the posterior fourchette and anus — a mediolateral incision at 45-60° from the midline deliberately avoids it. A midline episiotomy, while easier to repair, places the EAS at direct risk; in India, the mediolateral technique is standard. A third-degree tear involves partial or complete disruption of the EAS; a fourth-degree tear involves the EAS plus the rectal mucosa — both require specialist repair.
For urinary catheterisation, the key anatomical points are: the female urethra is 3-4 cm long (much shorter than the male urethra), making catheterisation generally straightforward; the urethral meatus lies in the midline between the clitoris anteriorly and the vaginal opening posteriorly; in postpartum women, oedema, haematoma, and perineal pain may distort local anatomy, making identification of the meatus challenging. The urinary bladder lies immediately posterior to the pubic symphysis; a full bladder elevates the uterine fundus and can impede uterine contraction, contributing to postpartum haemorrhage.
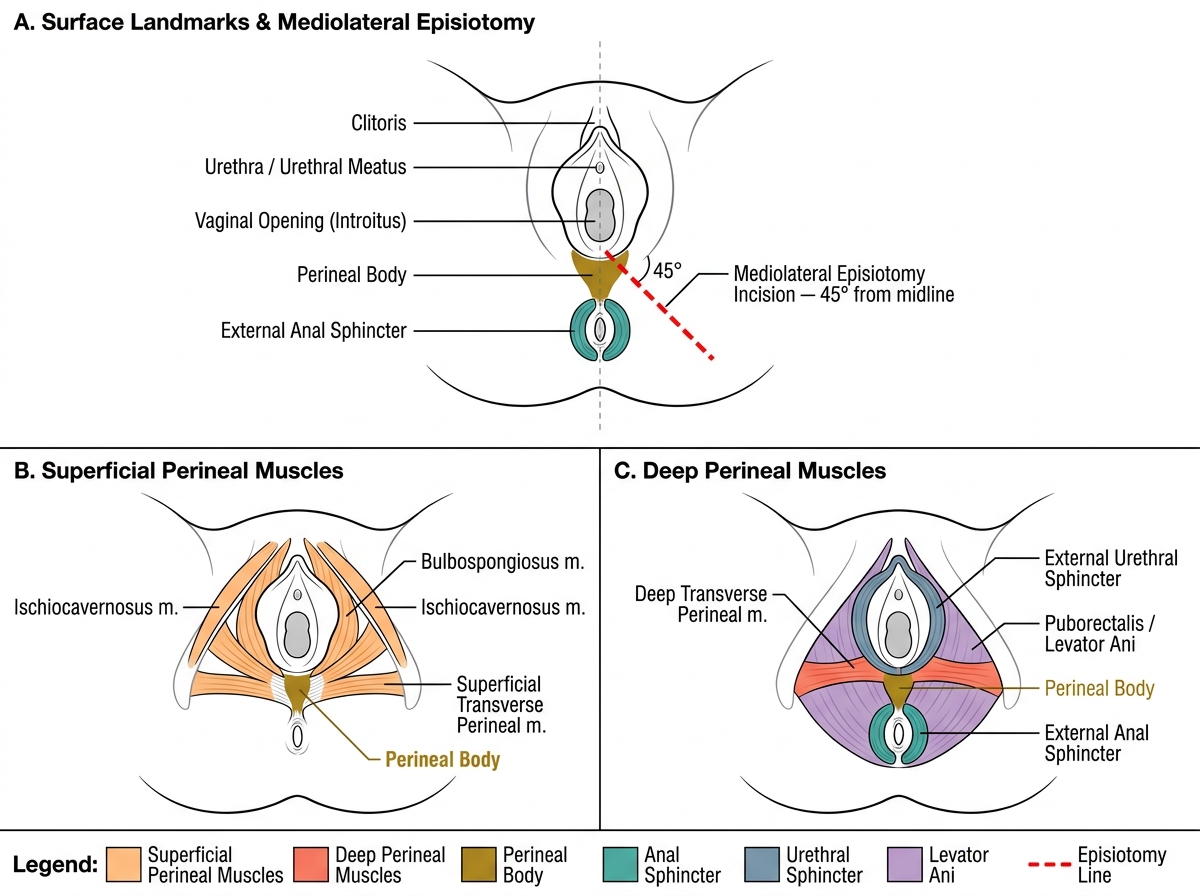
Female Perineal Anatomy and Mediolateral Episiotomy
Artificial Rupture of Membranes (ARM): Technique
ARM is a deliberate, irreversible procedure that permanently removes the protective barrier of the amniotic membranes from the fetus, and this irreversibility is what makes it categorically different from most other diagnostic manoeuvres performed in labour. Once the membranes are ruptured, the sterile amniotic environment is lost, the fetus is exposed to the potentially colonised birth canal, and delivery must be completed within a time frame that prevents chorioamnionitis. Every hour of ruptured membranes without delivery increases the risk of ascending infection, particularly if repeated vaginal examinations are performed. The decision to perform ARM therefore commits the entire obstetric team to active labour surveillance, appropriate fetal monitoring, and timely delivery planning. The technique must be executed with meticulous attention to two safety principles: the fetal head must be engaged before rupture to prevent cord prolapse, and the amnihook must be guided alongside the examining fingers rather than introduced blindly to prevent inadvertent injury to fetal scalp vessels or the cord.
Prerequisites before ARM:
- Fully explained procedure to the patient; verbal consent obtained
- Confirm engagement of fetal head (at or below the level of the ischial spines on vaginal examination; should be ≥2/5 palpable abdominally — i.e. mostly below the pelvic brim)
- Confirm absence of cord or vessel presentation (pulsatile structure on VE before rupture is a contraindication)
- Confirm fetal heart rate is normal immediately before the procedure
- Have a plan for fetal heart rate monitoring immediately after ARM
Equipment:
- Amnihook (long plastic hook with a small notched tip) — standard in most units, OR
- Kocher's forceps (older technique — pointed closed blades used to nick the membrane)
- Sterile gloves, lubricant
- Amniscope or standard VE tray
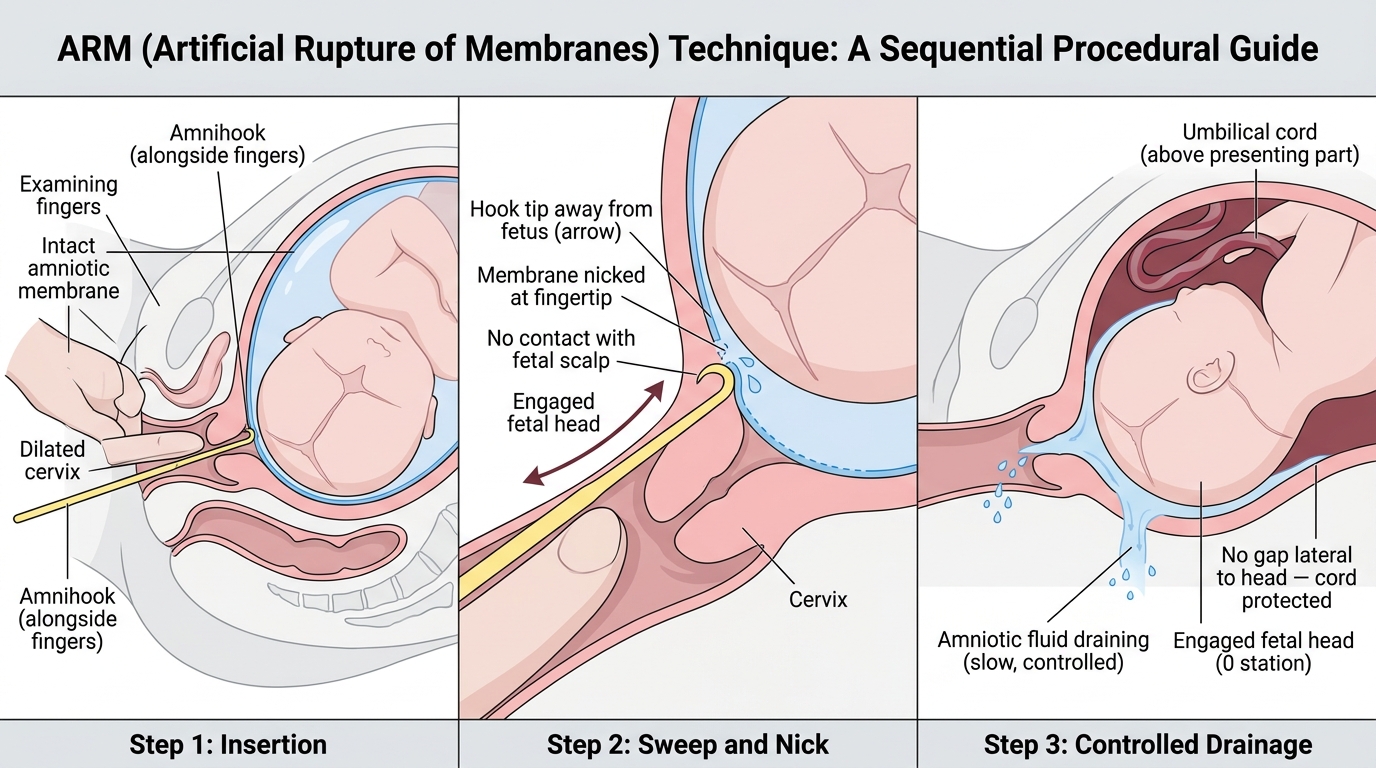
Step-by-step technique:
1. Position: patient in dorsal lithotomy or semi-recumbent position
2. Perform a sterile vaginal examination with two fingers; confirm head engagement, station, and cervical dilatation; note any pulsatile cord
3. While keeping your examining fingers in the vagina to guard the cord and direct the instrument, introduce the amnihook alongside your fingers (NOT blindly)
4. Direct the hook to the bulging membrane at the level of the external os; ensure the hook tip is pointing away from the fetal head and is not in contact with scalp
5. Apply gentle lateral traction to nick the membrane — a small controlled rent is sufficient; do not slash widely
6. Allow fluid to drain slowly between your fingers; note the colour (clear/straw = normal; green = meconium; blood-stained = possible abruption or vasa praevia tear)
7. Immediately after membrane rupture: check for cord by sweeping the vaginal vault with your examining fingers; auscultate or check the CTG for fetal heart rate immediately
8. Document: time, cervical dilatation at ARM, colour and volume of liquor, fetal heart rate before and after
Cord prolapse emergency: if FHR decelerates after ARM, immediately check for cord at the os. If cord is felt or visible, displace the head upward manually with fingers in the vagina to relieve cord compression, place the patient in knee-chest or Trendelenburg position, call for urgent senior help, and prepare for immediate emergency delivery (LSCS or operative vaginal delivery if fully dilated).
Artificial Rupture of Membranes (ARM): Step-by-Step Technique
SELF-CHECK
Before performing ARM, you check the fetal head engagement. You find the head is 4/5 palpable above the pelvic brim on abdominal examination and is felt at station -2 on vaginal examination. What should you do?
A. Proceed with ARM immediately since the cervix is well dilated
B. Defer ARM until the head is more engaged to reduce the risk of cord prolapse
C. Perform ARM and immediately apply a fetal scalp electrode to monitor the heart rate
D. Perform ARM and ensure the patient is in the lithotomy position to prevent cord prolapse
Reveal Answer
Answer: B. Defer ARM until the head is more engaged to reduce the risk of cord prolapse
A head that is 4/5 palpable abdominally (i.e., mostly above the pelvic brim) or at station -2 is unengaged. Performing ARM in this situation creates a gap between the leading part and the lower uterine segment through which the umbilical cord can prolapse as liquor rushes out. Cord prolapse is a life-threatening emergency. ARM should be deferred until the head descends and engages (ideally 2/5 or less palpable abdominally, or 0 station or below). Fetal scalp electrode application (option C) does not mitigate cord prolapse risk. Position (option D) does not prevent cord prolapse.