Page 9 of 20
OG35.18 | IUD Procedural Skill — SDL Guide
Learning Objectives
- Demonstrate the correct technique to insert a copper IUCD (CuT 380A) in a simulated or supervised environment (OG35.18)
- Demonstrate the correct technique to remove an IUCD in a simulated or supervised environment (OG35.18)
- Apply the WHO Medical Eligibility Criteria to select appropriate candidates for IUCD insertion
- Recognise and manage common post-insertion complications including expulsion, infection, and missing threads
- Describe the principles and technique of PPIUCD insertion within the Indian national programme context
INSTRUCTIONS
The intrauterine contraceptive device (IUCD) is one of the most effective reversible contraceptive methods available, with failure rates below 1% per year for the copper IUCD and comparable efficacy for the levonorgestrel-releasing intrauterine system. Correct insertion technique is the single most important factor determining IUCD effectiveness — a fundally-placed device has the lowest expulsion and failure rates. India's RMNCH+A programme includes PPIUCD insertion as a priority service at delivery points. This module builds your understanding of IUCD device types, patient selection, insertion and removal technique, and complication recognition for simulated and supervised practice.
References
- DC Dutta's Textbook of Gynecology, 8th ed. Ch. 28 — Contraception (textbook)
- Shaw's Textbook of Gynaecology, 17th ed. Ch. 27 — Family Planning (textbook)
- WHO Medical Eligibility Criteria for Contraceptive Use, 5th ed. 2015 (guideline)
- Ministry of Health and Family Welfare India — PPIUCD Training Manual, 2014 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 28-year-old woman, gravida 2 para 2, presents to the family planning clinic requesting long-acting reversible contraception. She delivered her second child 8 weeks ago by normal vaginal delivery and is breastfeeding. She has no vaginal discharge, no pelvic pain, and her last menstrual period has not yet returned. She wants spacing contraception for 3-5 years. As you counsel her, she mentions that a friend told her that 'the coil causes infections and often falls out.' You must explain the actual risks clearly, obtain a clinical history to rule out contraindications, and perform a successful IUCD insertion. What are the two most important items in the WHO MEC checklist before you begin? And if her threads cannot be seen at her 6-week follow-up, what is your first step?
WHY THIS MATTERS
Unintended pregnancy remains one of the most common causes of preventable maternal morbidity and mortality in India, accounting for approximately 50% of pregnancies in the country (NFHS-5 2021). Long-acting reversible contraceptives (LARCs) — including IUCD and implants — have failure rates below 1% per year, dramatically outperforming short-acting methods (pill, condoms) whose real-world efficacy drops to 70-80% with typical use. The Indian national RMNCH+A programme specifically targets PPIUCD insertion as a high-yield intervention: inserting the IUCD immediately after delivery captures a moment when the woman is highly motivated and has healthcare contact, and postpartum IUCD use has been shown to significantly increase LARC uptake at 6 months compared to delayed insertion. As a future clinician working at primary or secondary health care level, IUCD counselling and insertion will be among your most impactful family planning skills.
RECALL
Before proceeding, review these foundations. The uterus in a non-pregnant woman measures approximately 7-8 cm in length (longer in multiparous women), with a cavity depth of 6-8 cm on uterine sounding. The internal os is the narrow junction between the cervical canal and uterine cavity — it may require graduated cervical dilatation (Hegar dilators) when it is stenosed (postmenopausal, nulliparous). The WHO Medical Eligibility Criteria (MEC) for contraceptive use categorises conditions from Category 1 (no restriction) to Category 4 (absolute contraindication); IUCD is Category 4 in current pregnancy, puerperal sepsis within 3 months, unexplained vaginal bleeding, and known or suspected uterine cavity distortion. The failure rate of the CuT 380A is approximately 0.8% per year (typical and perfect use are similar because it is operator-placed and user-independent). The copper IUCD mechanism of action is primarily spermicidal (copper ions impair sperm motility and fertilisation) and secondarily creates a foreign-body endometrial inflammatory response hostile to implantation.
Indications, Contraindications and Patient Counselling
The IUCD is suitable for the vast majority of women seeking long-acting contraception, and the WHO Medical Eligibility Criteria provides a systematic, evidence-based framework for identifying the small proportion of women in whom insertion is contraindicated or requires caution. Understanding both the selection criteria and the counselling content is essential: poor counselling leads to premature discontinuation — up to 20% of IUCD users discontinue within the first year, most commonly because of inadequate preparation for expected changes in bleeding pattern or unfounded fears about pelvic infection or infertility. As a clinician, your role in IUCD provision is not merely technical; it is informational and counselling-based — a woman who understands what to expect and what symptoms require urgent review is far more likely to continue and benefit from her contraception than one who was given only the procedure.
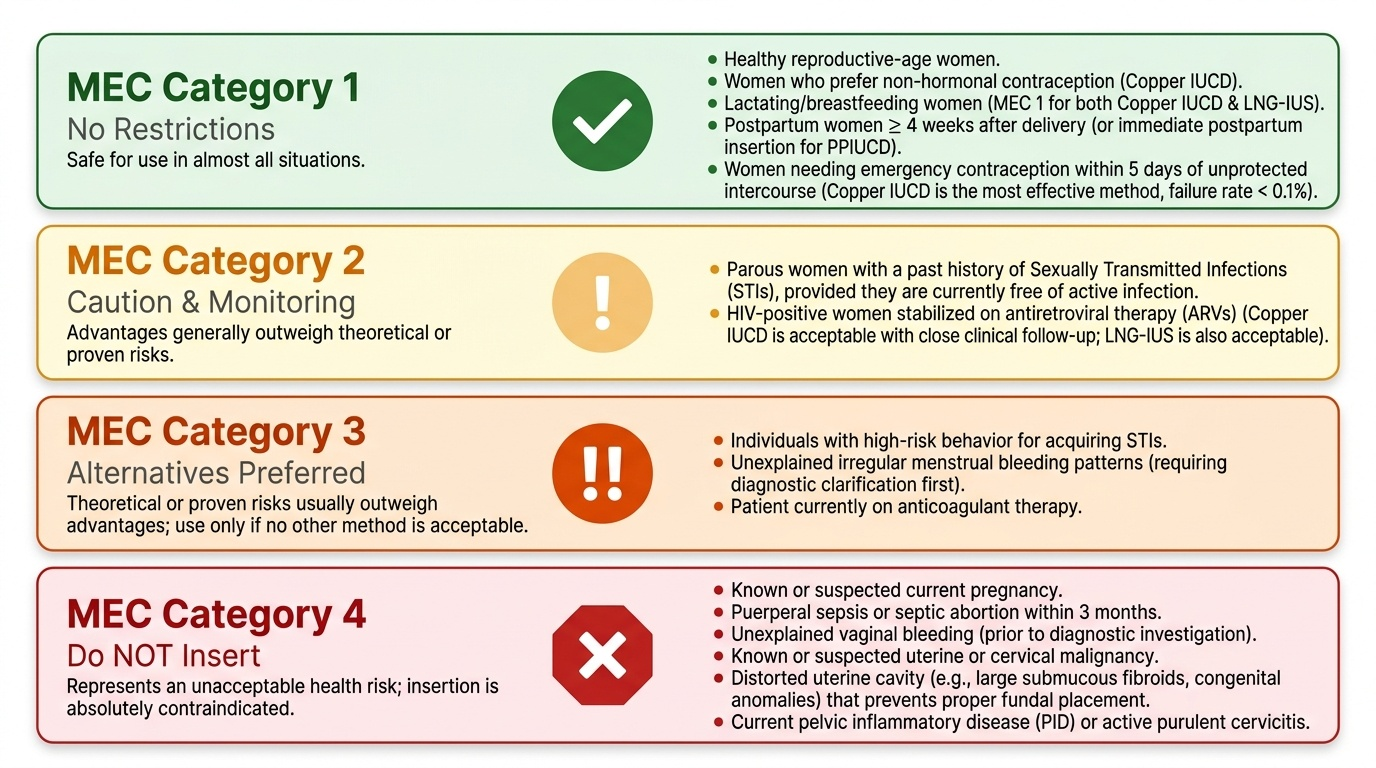
Who is an ideal IUCD candidate (WHO MEC Category 1 — no restrictions):
Most healthy reproductive-age women are eligible. The copper IUCD is particularly suitable for: women who prefer non-hormonal contraception; women during lactation (WHO MEC 1 for both copper and LNG-IUS); postpartum women 4 weeks or more after delivery (or at the time of delivery for PPIUCD); women needing emergency contraception within 5 days of unprotected intercourse (the copper IUCD is the most effective emergency contraceptive, with a failure rate below 0.1%).
Conditions where IUCD may be used with caution (WHO MEC Category 2-3):
Category 2 (advantages outweigh risks): parous women with past history of STI (if currently free of infection), HIV-positive women on antiretrovirals (copper IUCD acceptable with close follow-up; LNG-IUS also acceptable). Category 3 (theoretical risks outweigh advantages — alternatives preferred): high-risk behaviour for STI; irregular menstrual bleeding patterns requiring clarification first; anticoagulant therapy.
Absolute contraindications (WHO MEC Category 4 — do NOT insert):
- Current pregnancy (known or suspected)
- Puerperal sepsis or septic abortion within 3 months
- Unexplained vaginal bleeding (before investigation)
- Known or suspected uterine or cervical malignancy
- Distorted uterine cavity (large submucous fibroids, congenital anomalies) preventing fundal placement
- Current pelvic inflammatory disease (PID)
- Known or suspected allergy to device components (copper allergy for CuT 380A)
Counselling content (mandatory before insertion):
Effectiveness (over 99%) and duration (CuT 380A up to 10 years; LNG-IUS up to 5 years); mechanism of action; expected changes in bleeding (copper IUCD often increases menstrual flow and dysmenorrhoea, especially in first 3-6 months; LNG-IUS reduces menstrual flow); how to check the threads monthly; when to return immediately (severe pelvic pain, heavy bleeding, partner feels threads, threads not felt by user); complete reversibility.
Provided image
Uterine Anatomy and IUCD Device Types
A working knowledge of uterine cavity dimensions and the design of each IUCD type is essential for selecting the correct device and placing it correctly. The two device types in common use differ substantially in their mechanism, dimensions, and clinical effects, and the choice between them depends on the patient's clinical circumstances and preferences after counselling. Mastering the relationship between device geometry and uterine cavity dimensions prevents two critical errors: attempting insertion into a cavity too small for the device (increasing expulsion and perforation risk) and failing to achieve fundal placement (reducing contraceptive efficacy).
The uterine cavity is triangular in cross-section, wider at the fundus (approximately 4 cm wide) and narrowing to the internal os (approximately 5 mm). The ideal position for any intrauterine device is at the fundus — because fundal placement is associated with the lowest expulsion rates and highest contraceptive efficacy. A device placed too low (lower uterine segment or cervical canal) is at high risk of expulsion and may not be adequately contraceptive. The position is confirmed by uterine sounding before insertion: the measured sound depth guides the depth setting on the insertion device.
CuT 380A (copper IUCD): T-shaped polyethylene frame with copper wire wound around the vertical stem (380 mm² copper surface area) and copper collars on each horizontal arm; total dimensions approximately 36 mm (length) by 32 mm (width) when expanded. The high copper surface area accounts for its excellent spermicidal efficacy and 10-year effective life. Threads (two monofilament strings) are attached to the stem base and should protrude 2-3 cm through the external os after insertion. The inserter tube is 4 mm outer diameter — this usually passes through the internal os without dilatation in multiparous women, but nulliparous or postmenopausal women may require Hegar dilatation to 4-5 mm first.
LNG-IUS (levonorgestrel intrauterine system, Mirena 52 mg): T-shaped frame with a hormone-releasing cylindrical reservoir on the vertical stem containing 52 mg levonorgestrel released at 20 µg/day; total dimensions 32 mm by 32 mm; inserter diameter 4.8 mm. The local hormonal effect causes endometrial atrophy and thickened cervical mucus, resulting in significantly reduced menstrual flow (amenorrhoea in 20% of users); it is the first-line treatment for heavy menstrual bleeding requiring concurrent contraception.
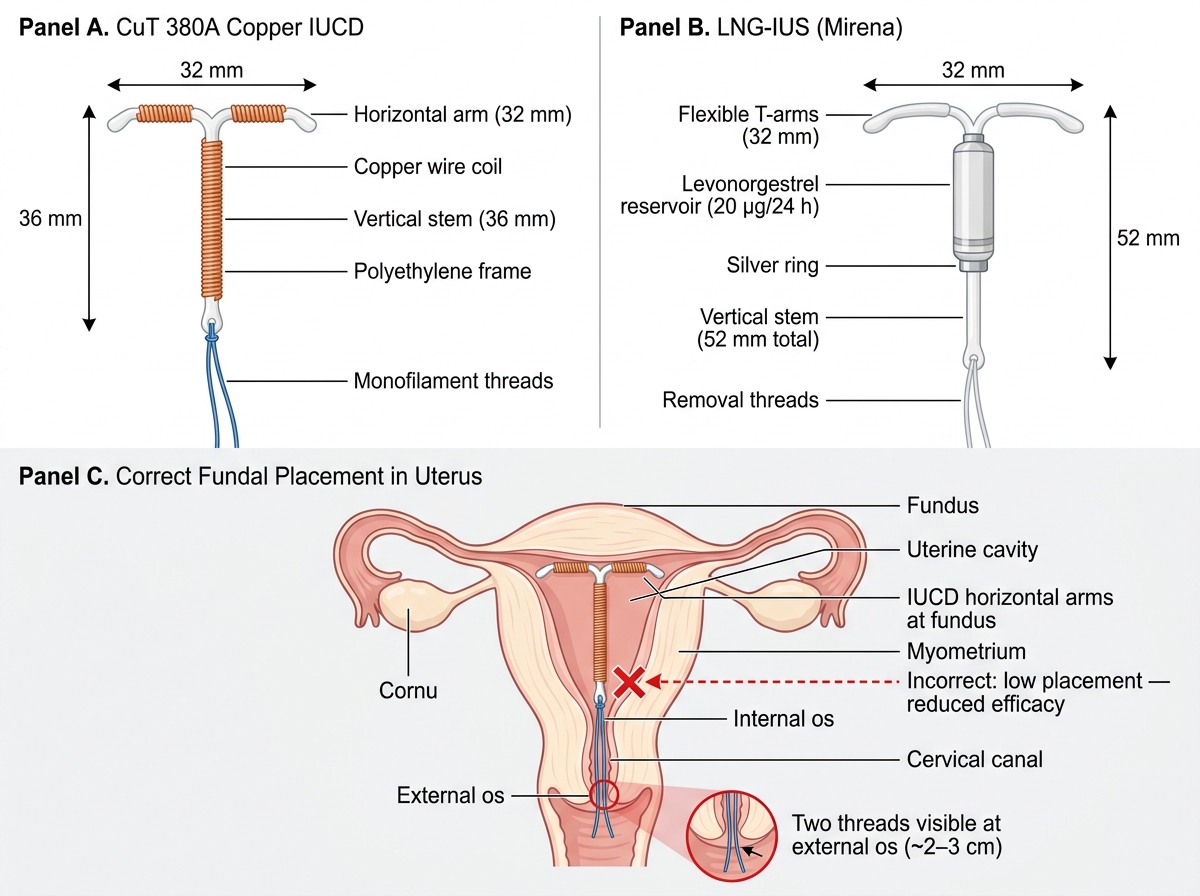
CuT 380A vs LNG-IUS Device Comparison and Correct Fundal Placement
IUCD Insertion Technique: Step-by-Step
IUCD insertion is a minor invasive procedure requiring meticulous aseptic technique and precise instrument control to achieve fundal placement, avoid uterine perforation, and preserve the sterile uterine environment. The procedure takes approximately 5-10 minutes in experienced hands. The critical technical principle that must be understood before the procedure begins is the withdrawal technique: at the moment of deployment, the outer insertion tube is withdrawn while the central rod is held completely stationary — this allows the device arms to open at the fundus. The intuitive movement of advancing the rod will push the device downward rather than deploying it at the fundus, wasting the sounding measurement and reducing efficacy. All steps must be performed using no-touch aseptic technique because introducing pathogens to the uterine cavity at insertion is the primary mechanism of IUCD-associated pelvic infection in the first 20 days after insertion.
Equipment:
- Cusco speculum
- Sponge-holding forceps and gauze swabs
- Antiseptic solution (povidone iodine or chlorhexidine)
- Uterine sound (calibrated)
- Vulsellum or single-toothed tenaculum (for cervical traction)
- CuT 380A in sterile package with inserter
- Sterile gloves and drapes
- Good light source
Step-by-step insertion (CuT 380A):
1. Position: dorsal lithotomy; perform bimanual pelvic examination before insertion to determine uterine size, position (anteverted/retroverted), and confirm no adnexal masses
2. Insert Cusco speculum; visualise cervix; clean cervix and vaginal vault with antiseptic swabs using no-touch technique
3. Apply a vulsellum (single-tooth tenaculum) to the anterior lip of the cervix at 12 o'clock; this straightens the uterine axis and provides counter-traction — use gentle steady traction
4. Sound the uterus: introduce the calibrated uterine sound slowly in the axis of the uterus until the fundus is felt (soft resistance); note the depth in centimetres (normal 6-8 cm); if less than 6 cm, the uterus may be too small for standard CuT 380A
5. Remove the sound; load the CuT 380A into the inserter tube (horizontal arms folded); set the depth indicator to the measured uterine depth
6. Introduce the loaded inserter through the cervical os to the fundus (indicator at os level = correct depth); do NOT push against resistance
7. Withdrawal technique: hold the insertion rod completely stationary while withdrawing the outer inserter tube — this releases the arms at the fundus; the rod is NOT advanced
8. Withdraw the inserter rod; cut the threads to 2-3 cm from the external os
9. Remove vulsellum; remove speculum; note any tenaculum-site bleeding
10. Inform the patient: how to check threads monthly; return in 6 weeks for thread check; return immediately if severe pain, heavy bleeding, or missing threads
PPIUCD insertion (within 48 hours of vaginal delivery): insert the IUCD manually (without sounding) immediately after placental delivery using ring forceps to guide the device to the fundus; threads should be cut longer (10-12 cm) to account for subsequent uterine involution. At caesarean section: place the device directly through the uterotomy incision by hand, then pass threads through the cervix with long forceps before closing the uterotomy.
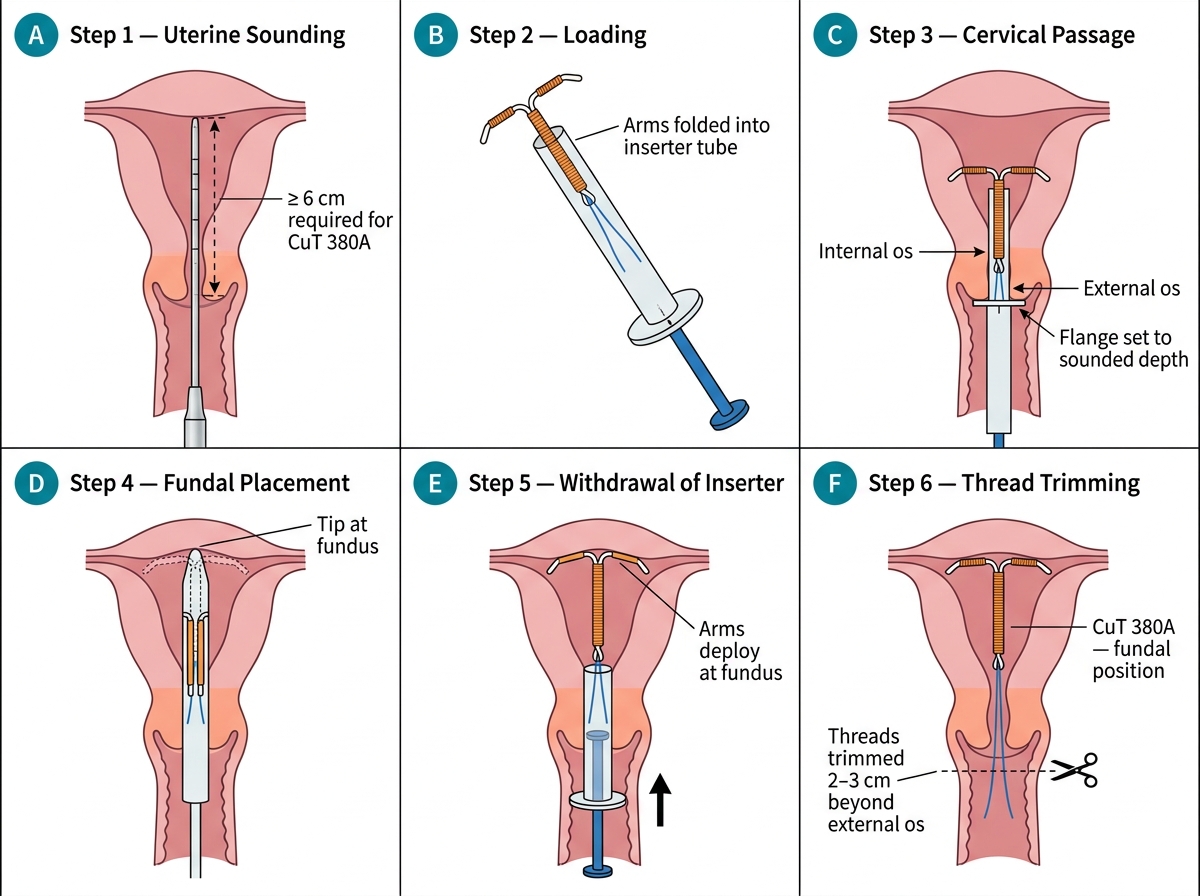
CuT 380A Insertion: Step-by-Step Procedural Sequence
SELF-CHECK
During CuT 380A insertion, the uterine sound measures 5 cm depth. How should you proceed?
A. Insert the IUCD using the standard technique — 5 cm is within normal range
B. Defer insertion; the uterine cavity is too small for a standard CuT 380A
C. Force the sound further until 7 cm is reached to ensure a standard cavity depth
D. Insert the IUCD without sounding since the depth result is unreliable in multiparous women
Reveal Answer
Answer: B. Defer insertion; the uterine cavity is too small for a standard CuT 380A
A uterine sound depth of less than 6 cm indicates a cavity that may not accommodate a standard CuT 380A (frame width 32 mm, stem length 36 mm). Inserting a device that is too large for the cavity risks mal-positioning, higher expulsion rate, and increased pain. The correct action is to defer insertion and offer an alternative contraceptive method or refer for specialist assessment. Forcing the sound (option C) risks uterine perforation. Skipping the sound (option D) removes a critical safety measurement regardless of parity.