Page 14 of 20
OG19.3 | Tubal Ligation Observation — SDL Guide (Part 2)
What the Observer Monitors: Anaesthesia, Complications and Decision Points
During your theatre observation, your role extends beyond watching the surgical steps — you are also expected to understand the anaesthetic approach, recognise the signs of intraoperative complications, and appreciate the decision points at which the operating team must modify their plan. This observational awareness is what transforms passive theatre attendance into active procedural learning, and it is the competency level that OG19.3 requires.
Anaesthetic approach: Postpartum mini-laparotomy is most commonly performed under spinal anaesthesia (already in place or given after delivery); the subarachnoid block is usually L3-4 with hyperbaric bupivacaine 0.5%, providing anaesthesia to the T6 level. Interval mini-laparotomy may use spinal or local anaesthesia (the incision is small and the procedure brief). Laparoscopic sterilisation requires general anaesthesia in most centres (pneumoperitoneum and Trendelenburg position are poorly tolerated under regional anaesthesia). The observer notes: patient positioning for spinal (sitting or lateral flexed), the time-to-block-onset before incision begins, patient blood pressure monitoring (spinal hypotension is common — IV fluid preloading and vasopressors as needed).
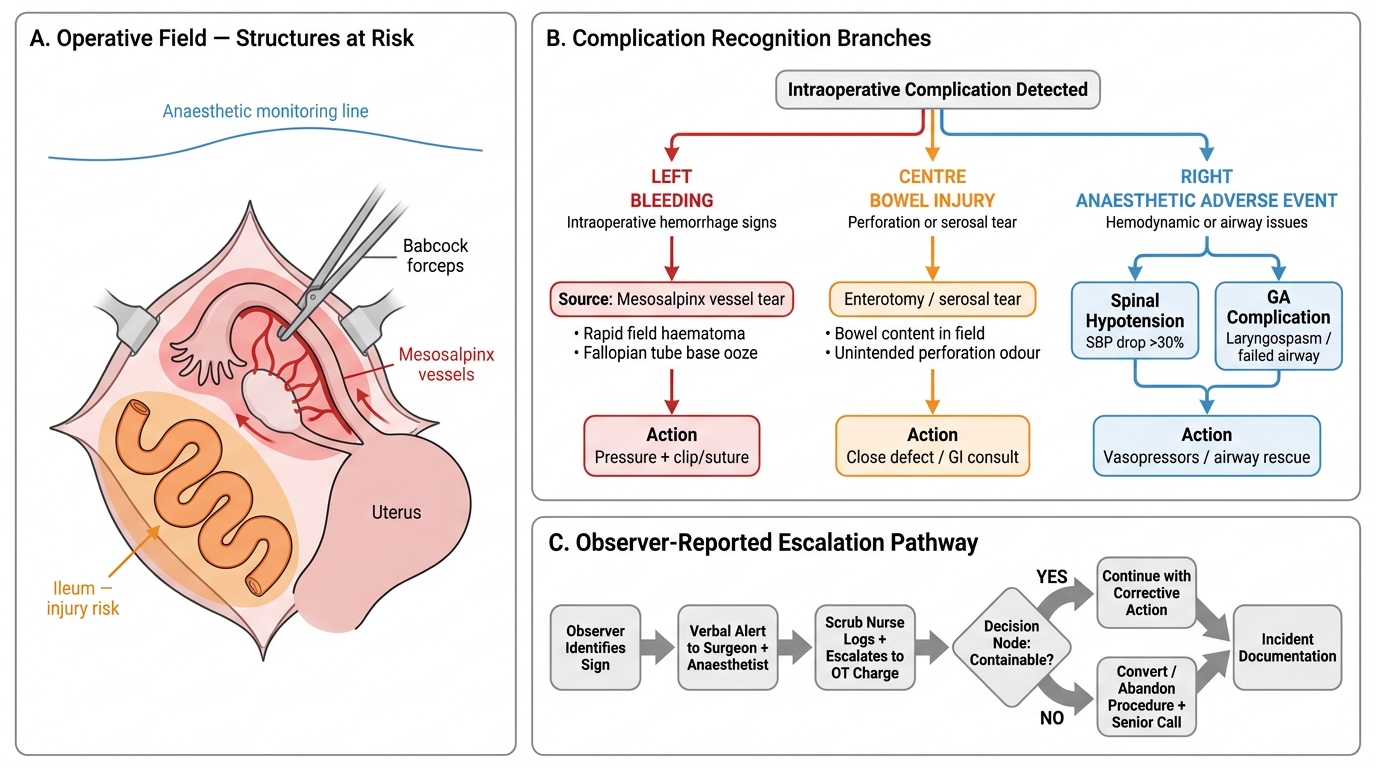
Intraoperative complications the observer recognises:
- Mesosalpinx bleeding: the most common complication; caused by inadequate haemostasis at the tubal excision site; manifested as persistent bleeding from the broad ligament; managed with a further ligature, haemostatic clip, or bipolar diathermy
- Failure to identify the tube: tubes not visible due to adhesions, large uterus, or obese patient; decision point — convert to laparoscopy, extend incision, or defer procedure
- Visceral injury (bowel or bladder): rare in mini-laparotomy; more common with laparoscopic Veress needle or trocar entry; manifested as unexpected peritoneal contents or discolouration; requires immediate escalation
- Anaesthetic complication: spinal hypotension (BP drop >30% — treat with IV fluids, vasopressor), high block (respiratory distress, nausea), or general anaesthesia complications in laparoscopic cases
Post-procedure assessment (what the observer notes):
On completion, the surgeon confirms haemostasis, closes the peritoneum and fascia in layers, and closes the skin. The observer notes the operation duration, any complications documented, blood loss estimate, and the post-operative instructions. The patient's consent form, operative note, and complications must all be congruent and complete before the patient leaves theatre.
Intraoperative Complication Recognition and Escalation — Tubal Ligation
SELF-CHECK
During a postpartum mini-laparotomy for tubal ligation, the surgeon is unable to identify the fallopian tube due to dense adhesions from a prior appendicectomy. What is the most appropriate surgical decision?
A. Proceed with ligation of the most visible tubular structure in the field — it is likely the tube
B. Convert to laparoscopy, extend the incision for better access, or defer the procedure — confirm the correct structure before ligating
C. Perform a total abdominal hysterectomy as an alternative to achieve permanent sterilisation
D. Discharge the patient without sterilisation and document that the procedure was refused
Reveal Answer
Answer: B. Convert to laparoscopy, extend the incision for better access, or defer the procedure — confirm the correct structure before ligating
The cardinal rule of tubal ligation is that the correct structure must be positively identified before ligation — because ligating the round ligament instead of the fallopian tube leaves the patient unprotected and may lead to an unintended pregnancy. When the anatomy is obscured, the correct options are: convert to laparoscopy (better visualisation), extend the mini-laparotomy incision for improved access, or defer the procedure to an interval list when adhesiolysis can be properly planned. Option A (ligate what seems likely) risks a wrong-structure ligation. Option C (hysterectomy) is disproportionate and not appropriate for sterilisation. Option D should be documented only if the patient truly changed her mind — not for a surgical difficulty.
Supervised Observation in Practice: Learning Objectives and Documentation
The OG19.3 competency is explicitly set at the observe/assist level (KH — knowledge and history-taking skills), and this deliberate placement reflects a pedagogical and safety decision: tubal ligation is a permanent, irreversible, surgical procedure with medico-legal consequences that requires supervised operative experience beyond MBBS level before independent performance is appropriate. Your role in the theatre is therefore not to perform the procedure, but to maximise the learning value of your observation by watching actively, understanding the surgeon's decisions, and contributing to patient safety in the ways that are within your scope. The three observable performance domains that NMC expects at this level are: (1) understanding of surgical anatomy and technique, (2) recognition of the counselling and consent requirements, and (3) awareness of intraoperative safety practices and complication patterns. Your theatre log entry after each observation should document all three domains, not merely note that you "attended" the procedure.
What to actively observe and document during theatre exposure:
1. Identify the route of access (mini-laparotomy — postpartum subumbilical or interval suprapubic; or laparoscopic) and understand why that route was chosen for this patient
2. Observe how the surgeon identifies the fallopian tube — trace it from the cornu to the fimbriae before any occlusion begins
3. Identify the technique being used (Pomeroy, fimbriectomy, clip, ring, etc.) and the tubal segment being occluded
4. Note the anaesthetic approach and observe the anaesthetist's monitoring: pulse, BP, SpO2, end-tidal CO2 (laparoscopic)
5. Observe haemostasis at the excision site; note whether the surgeon sends a histological specimen and whether it is labelled
6. Listen to the operation note being dictated or written: indication, consent, technique, specimen, haemostasis, complications, estimated blood loss
Operation note structure you should be able to write (from observation):
Date, patient ID, surgeon and assistant names, anaesthetic type, position and preparation, incision and access, findings (tube identified, adhesions if any, other pelvic pathology), technique used (e.g., modified Pomeroy bilateral), specimen details, haemostasis, closure in layers, post-operative plan.
Legal and ethical context: Under the Indian MTP Act 2021, sterilisation that is concurrent with an MTP follows MTP documentation rules. Standalone sterilisation requires separate written informed consent under the national family planning programme guidelines. The observer should be aware that written consent forms in a language the patient understands, signed before any premedication, are required — consent obtained after sedation or anaesthesia induction is not valid. If the observer believes the consent process was inadequate or the patient changed her mind at any point, this must be raised immediately with the supervising surgeon or team lead.
CLINICAL PEARL
The modified Pomeroy technique is the most reliable for ensuring that the correct structure was excised because the excised loop can be identified as fallopian tube on histology. The round ligament is a common wrong-structure ligation — it is white, cord-like, and in the same operative field. The key distinction intraoperatively is that the fallopian tube has a recognisable lumen on cross-section (visible when the loop is cut), while the round ligament has a solid fibromuscular core. When in doubt, the surgeon traces the structure from the uterine cornu to its lateral end — the fallopian tube ends at the ovarian fimbriae, and the round ligament ends in the inguinal canal. Never ligate without positive identification.
Self-Assessment
At the observe/assist level (OG19.3), your self-assessment focuses on the knowledge and clinical reasoning competencies that determine whether you are prepared to enter a theatre session as an informed, contributing observer — and to manage post-procedure situations such as sterilisation failure or patient regret. The questions below are pitched at the level of understanding expected of a final-year MBBS student who has read this module and completed at least one supervised theatre observation. They are not aimed at independent operative competency, which is a post-internship and residency-level objective. Use these questions to identify the knowledge gaps you need to address before your next theatre session.
Using these questions as a structured debrief after each theatre session deepens the encoding of observed procedural knowledge into retrievable clinical memory, and creates a written record that can support reflective portfolio entries or OSCE preparation.
Knowledge questions:
1. Name the four anatomical segments of the fallopian tube in order from the uterus to the ovary.
2. Which tubal segment is occluded in the modified Pomeroy technique, and why is histological confirmation of the specimen important?
3. Name two factors that significantly increase a woman's risk of post-sterilisation regret.
4. What is the cumulative 10-year failure rate of tubal ligation (modified Pomeroy) per the CREST study, and what is the implication for ectopic pregnancy risk if the procedure fails?
5. What is the correct anaesthetic approach for postpartum mini-laparotomy sterilisation, and what is the most common intraoperative anaesthetic complication?
Reflective questions (observe/assist level):
- After observing a tubal ligation, can you describe each step in sequence without referring to notes?
- Could you write a complete, accurate operation note from your theatre observation?
- If a patient told you immediately post-operatively that she felt she had been pressured into sterilisation, what would you do?
SELF-CHECK
A 29-year-old woman underwent postpartum bilateral tubal ligation by modified Pomeroy technique 2 years ago. She now presents with a 6-week amenorrhoea and a positive urine pregnancy test. She has mild right iliac fossa pain. What is the most important immediate step?
A. Reassure her that intrauterine pregnancy after tubal ligation is common and arrange an antenatal booking
B. Obtain an urgent transvaginal ultrasound to confirm intrauterine location and exclude ectopic pregnancy
C. Administer methotrexate empirically for presumed ectopic pregnancy
D. Arrange interval salpingectomy to prevent recurrence of sterilisation failure
Reveal Answer
Answer: B. Obtain an urgent transvaginal ultrasound to confirm intrauterine location and exclude ectopic pregnancy
After tubal ligation failure, the proportion of resulting pregnancies that are ectopic is disproportionately elevated — estimated at approximately 7 times the baseline rate per the CREST study, because the residual tubal segment may allow fertilisation but prevent normal transport of the embryo to the uterus. A positive pregnancy test in a sterilised woman with pelvic pain must be treated as an ectopic pregnancy until proven otherwise by urgent transvaginal ultrasound. Option A (reassure as intrauterine) is dangerous — most pregnancies after sterilisation failure are ectopic. Option C (empirical methotrexate) should not be given before confirming ectopic location (an intrauterine pregnancy would be harmed). Option D is a future consideration, not the immediate step.