Page 1 of 27
OG37.1 | Caesarean Section Observation — SDL Guide
Learning Objectives
- Identify the clinical indications for caesarean section and understand the urgency classification system
- Describe the anatomy of the lower uterine segment and the surgical planes relevant to LSCS
- Follow the sequential steps of an LSCS procedure as an informed observer at the scrub table
- Distinguish between lower-segment and classical caesarean section and recognise when each is indicated
- Identify intraoperative findings and key decision points during a caesarean section
- Recognise early signs of intraoperative complications and observe the surgical team's response
- Document an observed caesarean section accurately in the logbook
INSTRUCTIONS
Caesarean section is the most commonly performed major obstetric surgery in modern maternity care, and as a final-year student you are required to observe and assist in the procedure (NMC OG37.1). This module prepares you to make the most of that theatre experience — not merely as a passive bystander but as an informed observer who understands every step, every decision, and every potential complication as it unfolds. Read this module before your obstetric theatre posting. Use the self-check questions to test your preparedness, and complete your logbook documentation immediately after each observed case.
References
- DC Dutta's Textbook of Obstetrics, 9th edition, Chapter 37 — Caesarean Section (textbook)
- Williams Obstetrics, 26th edition, Chapter 30 — Caesarean Delivery and Peripartum Hysterectomy (textbook)
- FOGSI Good Clinical Practice Recommendation — Caesarean Section, 2019 (guideline)
- NICE Guideline NG192 — Caesarean Birth, 2021 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
You are in the labour ward at 2 AM when the midwife calls: a 28-year-old primigravida at 39 weeks with a reassuring CTG suddenly develops prolonged fetal bradycardia after a spontaneous membrane rupture. The CTG shows a sustained deceleration to 80 bpm persisting for four minutes. The registrar examines her — cervix 3 cm, fully effaced — and calls for an emergency caesarean section. Within eight minutes the patient is wheeled into theatre. As the student on call, you scrub and stand at the table. What will you see? What decisions will the surgeon make? What complications must you be ready to observe? This module gives you the understanding to answer all of those questions.
WHY THIS MATTERS
Caesarean section now accounts for approximately 17–20% of deliveries in India and rising proportions globally. As an obstetrician — or as any doctor who works near maternity services — you will encounter post-caesarean patients, counsel women about the procedure, manage post-CS complications, and in some settings be the first responder when the surgery goes wrong. The NMC CBME curriculum requires you to observe and assist at least one caesarean section (OG37.1, SH level). This module ensures that your theatre time is purposeful: you will understand every incision, every instrument, and every intraoperative decision before you see it live.
RECALL
Before proceeding, take a moment to recall the relevant anatomy and clinical foundations. The uterus at term is a muscular organ weighing approximately 1 kg with a blood flow of 500–750 mL/min — haemostasis is paramount in uterine surgery. The lower uterine segment, which forms from the isthmus during the third trimester, is thin, avascular relative to the upper segment, and anatomically distinct from the upper segment both in muscle density and in its relationship to the bladder. From your obstetrics lectures, you should also recall the broad categories of CS indications — cephalopelvic disproportion (CPD), fetal distress, placenta praevia, malpresentation, previous uterine scar — and the four-tier urgency classification (Category I = immediate threat to life, through Category IV = elective at maternal/clinician preference). Finally, recall that PPH is defined as blood loss ≥500 mL after vaginal delivery or ≥1000 mL after caesarean section.
Why Caesarean Section? Indications and the Decision for Surgery
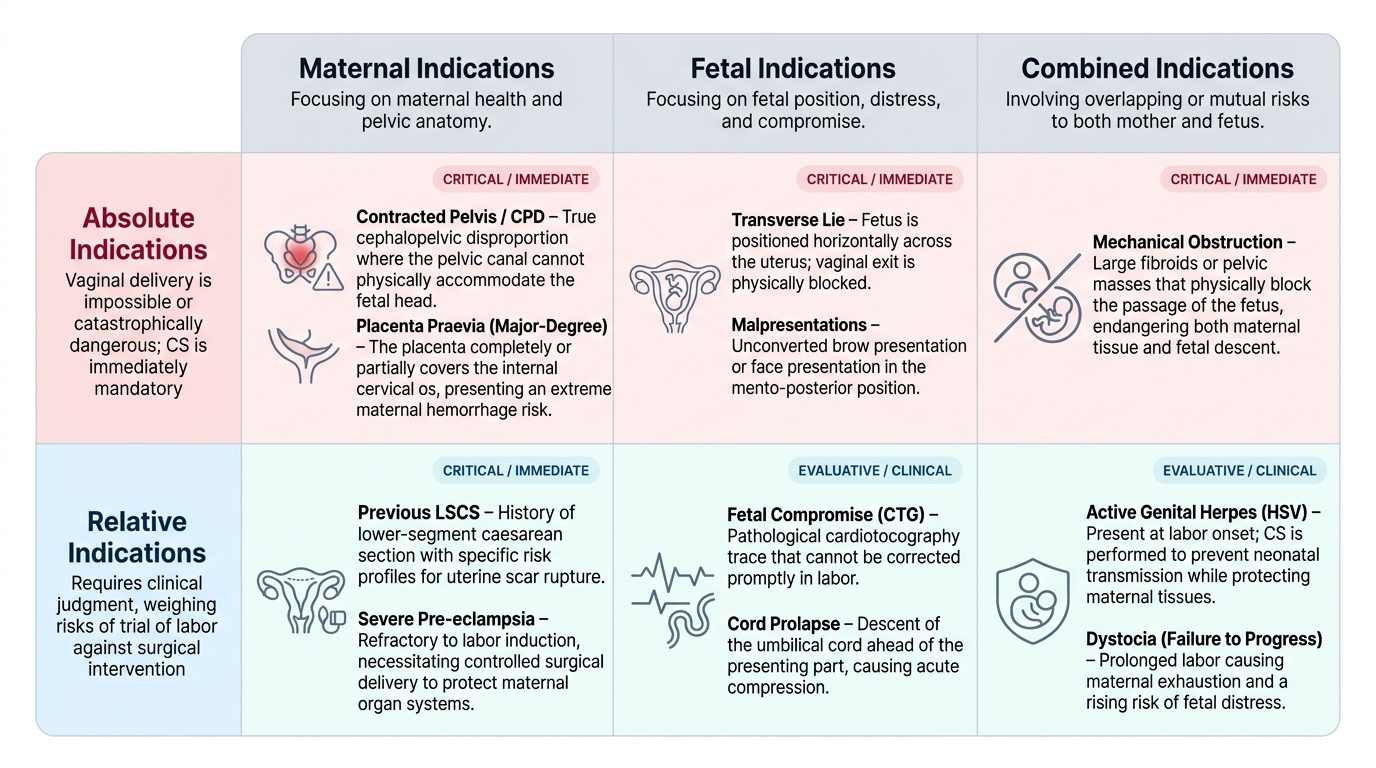
The decision to perform a caesarean section is one of the most consequential in obstetric practice, balancing maternal surgical risk against the risk of continuing with labour or vaginal delivery. Understanding the indication is the very first thing an observer at the theatre table should know before the skin incision is made, because it determines the urgency, the incision type, the approach to the uterus, and even the anaesthetic technique chosen.
Absolute indications are those where vaginal delivery is impossible or would be catastrophically dangerous: major-degree placenta praevia (where the placenta completely or partially covers the internal os), face presentation with mento-posterior position, brow presentation that fails to convert, contracted pelvis with true CPD, and transverse lie. In these situations, regardless of the fetal condition, caesarean section is unavoidable. Relative indications account for the majority of real-world cases and involve clinical judgment: previous lower-segment caesarean section (LSCS) with certain constellations of risk for scar rupture, severe pre-eclampsia refractory to labour induction, active genital herpes simplex at labour onset, cord prolapse, and fetal compromise on CTG that cannot be corrected in time to allow vaginal delivery.
The urgency classification system in wide clinical use (NICE NG192) places CS into four categories:
- Category I — Immediate threat to the life of the woman or fetus; requires delivery within 30 minutes of decision (or faster for truly acute emergencies like cord prolapse or uterine rupture).
- Category II — Maternal or fetal compromise not immediately life-threatening; target delivery within 75 minutes.
- Category III — No compromise, but early delivery needed; target within the next available operating slot.
- Category IV — Elective, at a time chosen by mother and clinician.
As an observer, the first question to ask yourself or to look up before scrubbing in is: 'What category is this case, and what is the primary indication?' This frames every subsequent step you observe.
Provided image
Anatomy of the Lower Uterine Segment and Surgical Planes
The anatomical rationale for the lower-segment caesarean section is elegant: the lower uterine segment (LUS) forms progressively from the isthmus during the second and third trimesters, reaching its maximum width and thinness at term. Because it contains fewer muscle fibres and is relatively avascular compared to the upper segment, an incision here bleeds less, heals more reliably, and is less likely to rupture in a subsequent pregnancy than an upper-segment (classical) incision.
The LUS sits within the uterovesical space, bounded anteriorly by the bladder and the vesicouterine peritoneal fold, superiorly by the uteroplacental vascular arcades, and laterally by the broad ligament containing the uterine vessels. During surgery, after entering the abdomen and the uterovesical peritoneum, the surgeon reflects the bladder downward to expose the anterior LUS — this 'bladder flap' manoeuvre is the critical step that protects the bladder from the uterine incision. The vesicouterine peritoneum is incised transversely about 1–2 cm above the bladder reflection, and the bladder is pushed down using a swab or the index finger.
Key anatomical structures the observer should watch the surgeon identify and protect:
- Bladder: reflected downward; injury recognised by a gush of clear fluid or visible bladder mucosa
- Uterine vessels: lateral on both sides; extension of the uterine incision laterally risks haemorrhage
- Ureters: travel within the broad ligament approximately 1–2 cm lateral to the uterine cervix; visible indirectly during lateral clamping for bleeding
- Round ligaments and utero-ovarian ligaments: identify the extent of the uterine fundus and adnexa
The uterine incision itself is placed transversely across the LUS, starting centrally and extended laterally by the fingers in a controlled 'stretch' motion rather than by scissors — this reduces risk of lateral extension into the uterine vessels.
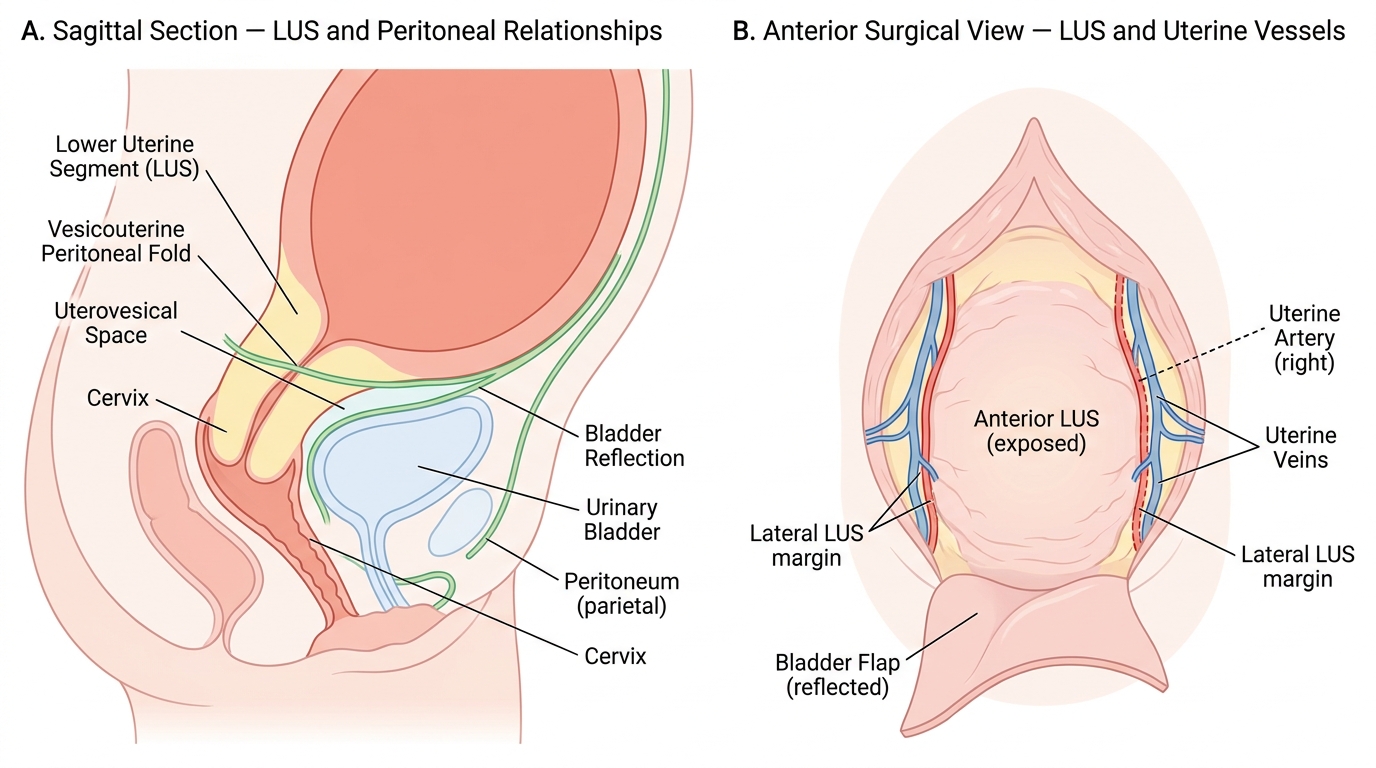
Lower Uterine Segment: Peritoneal and Vascular Anatomy
The LSCS Procedure — Step-by-Step from the Observer's Perspective
Observing an LSCS with a structured mental framework transforms a bewildering sequence of instrument exchanges into a comprehensible narrative. The procedure can be divided into seven sequential phases, and a good observer tracks which phase is underway at all times.
Phase 1 — Abdominal entry. The most commonly used incision is the Pfannenstiel incision: a curved transverse incision about 3 cm above the symphysis pubis, following the skin crease. The alternate Joel-Cohen technique uses a straight transverse incision slightly higher (about 3 cm below the anterior-superior iliac spine line), with blunt digital extension of the subcutaneous tissue and fascia rather than sharp dissection. Evidence from comparative trials shows the Joel-Cohen technique is associated with shorter operative times, less blood loss, and faster postoperative recovery, which is why it has gained wider adoption. After the skin incision, the anterior rectus sheath (linea alba) is divided transversely, and the recti muscles are separated in the midline by blunt dissection. The parietal peritoneum is opened vertically with sharp dissection, taking care to stay in the midline and away from the bladder.
Phase 2 — Bladder flap creation. The vesicouterine peritoneum is identified as a loose fold of peritoneum overlying the lower segment. It is incised transversely and the bladder reflected downward to expose the anterior LUS. The Doyen retractor (a curved blade) is placed to hold the bladder down throughout the procedure.
Phase 3 — Uterine incision. A small transverse stab incision is made centrally through the LUS with a scalpel. The surgeon then inserts two fingers into the incision and extends it laterally by traction, creating a smooth 8–10 cm transverse uterine opening. Note that the surgeon angles the incision slightly upward at the ends ('smile' incision) to avoid the uterine vessels laterally.
Phase 4 — Fetal extraction. This is often the most dramatic phase for observers. The surgeon places one hand into the uterine cavity and lifts the fetal head into the incision (or uses obstetric forceps if the head is impacted), while an assistant applies fundal pressure. The head is delivered through the incision, followed by the trunk and limbs. If the presentation is breech, the surgeon delivers by the feet (footling breech manoeuvre). Note the time of delivery — this is recorded for neonatal records.
Phase 5 — Placenta and membranes. Once the fetus is delivered and the cord clamped, the placenta is usually delivered by controlled cord traction with uterine massage. Oxytocin (typically 5 IU slow IV or 10 IU IM) is given at this stage to stimulate uterine contraction and prevent PPH.
Phase 6 — Uterine repair. The uterine incision is sutured in one or two layers using an absorbable suture (typically #1 Vicryl or chromic catgut). Single-layer and double-layer closure are both practised; the CORONIS trial found no significant difference in major outcomes between the two approaches, though debate continues. The surgeon inspects both angles of the incision carefully before completing closure.
Phase 7 — Abdominal closure. The peritoneum may or may not be closed (evidence supports non-closure of the visceral and parietal peritoneum with equivalent outcomes). The rectus sheath is closed with a continuous absorbable suture, and the skin is closed with subcuticular sutures or staples.
| Feature | Pfannenstiel Incision | Joel-Cohen Incision |
|---|---|---|
| Level | ~3 cm above symphysis, curved | ~3 cm below ASIS line, straight |
| Tissue separation | Sharp (scalpel) | Blunt (digital) |
| Operative time | Longer | Shorter |
| Blood loss | Slightly more | Less |
| Wound complications | Comparable | Comparable |
| Post-op recovery | Standard | Faster |
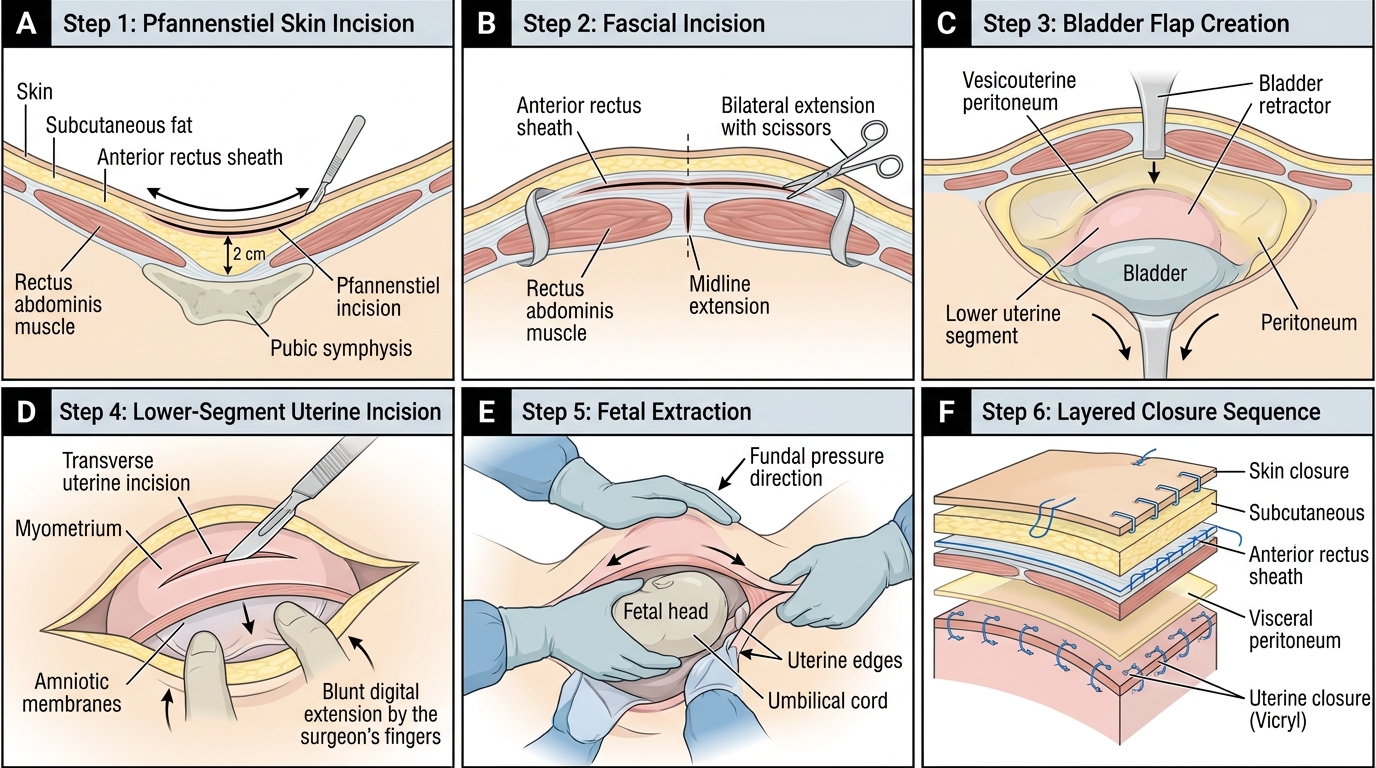
Step-by-Step LSCS Procedure: Surgical Sequence from Skin Incision to Closure