Page 3 of 27
OG37.1 | Caesarean Section Observation — SDL Guide (Part 3)
Immediate Postoperative Care and What to Document
The observer's responsibility does not end when the skin is closed. Understanding what happens in the recovery room consolidates the overall picture of caesarean section as a peri-operative episode of care, not merely an intraoperative procedure.
In the immediate postoperative period (first 1–2 hours), the most important monitoring parameters are uterine tone (assessed by palpating the fundus through the abdominal wall — it should be firm and contracted, at or below the umbilicus), lochia (the amount and character of vaginal bleeding), maternal vital signs (particularly blood pressure if spinal anaesthesia was used and if there was intraoperative haemorrhage), urine output via indwelling catheter (a minimum of 30 mL/h signals adequate renal perfusion), and oxygen saturation. The oxytocin infusion (typically 20–40 IU in 500 mL Ringer's lactate) is continued for at least 4 hours postoperatively to maintain uterine contraction.
Pain management after CS typically involves a multi-modal approach: intrathecal morphine (if spinal was used), regular paracetamol, NSAIDs (if not contraindicated), and supplemental oral opioids for breakthrough pain. Observe whether the anaesthesiologist mentions the intrathecal opioid — this provides excellent analgesia for 12–24 hours but carries a small risk of delayed respiratory depression requiring monitoring.
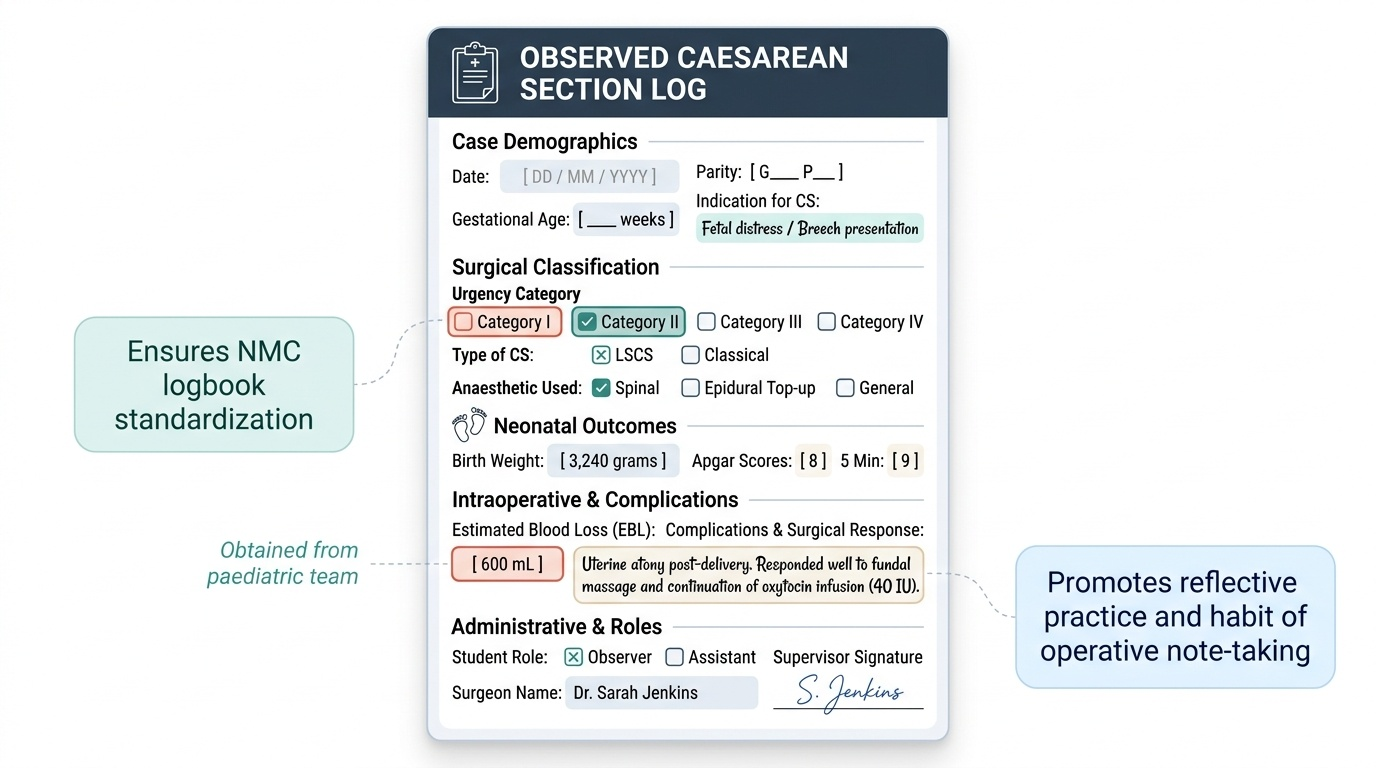
Logbook documentation for an observed CS should include:
- Date, parity, gestational age, and indication for CS
- Urgency category (I/II/III/IV)
- Type of CS (LSCS vs classical)
- Anaesthetic technique used (spinal / epidural top-up / general)
- Fetal birth weight and Apgar scores (obtained from the paediatric team)
- Estimated blood loss
- Any complications observed and the surgical response
- Your role (observer/assistant) and the supervising surgeon's name
This documentation serves multiple purposes: it fulfils the NMC logbook requirement, trains the habit of operative note-keeping, and provides a reflective record of learning.
Provided image
SELF-CHECK
After a caesarean section under spinal anaesthesia, a patient in the recovery room has uterine fundus that is soft and boggy at 20 minutes postoperatively. Estimated intraoperative blood loss was 800 mL. She is currently receiving oxytocin 20 IU in 500 mL at 125 mL/h. What is the most important immediate action?
A. Increase the oxytocin infusion rate and perform uterine massage
B. Administer carboprost 250 µg IM — it is the first-line response
C. Organise an urgent return to theatre for re-exploration
D. Transfuse 2 units of packed red cells immediately
Reveal Answer
Answer: A. Increase the oxytocin infusion rate and perform uterine massage
A boggy uterus in the recovery room with an ongoing slow bleed requires immediate bimanual uterine massage plus an increase in the oxytocin rate as first steps. Carboprost is a second-line uterotonic (contraindicated in asthma). Re-exploration and blood transfusion are indicated if initial measures fail — escalate stepwise.
Self-Assessment — Consolidating Your CS Observation
Use the following questions to test your readiness before theatre and to consolidate your learning after your observed caesarean section. These questions mirror the kinds of problems posed in structured viva examinations and clinical scenario OSCEs, and they directly reflect the competency level required by NMC (OG37.1, SH level — observe and assist). Working through them carefully will help you shift from passive recall of isolated facts toward active clinical reasoning about the procedure. For each question, construct a complete answer in your own words before consulting any reference — this deliberate retrieval practice is one of the most evidence-supported strategies for converting short-term recall into durable long-term understanding. After each theatre session, revisit whichever questions you found difficult and look them up in Dutta's Obstetrics or Williams Obstetrics before your next posting. The objective is not to memorise a checklist, but to be able to reason aloud in front of an examiner or senior clinician — demonstrating that you understand not just the steps of the procedure, but the physiological, anatomical, and clinical rationale behind each decision the surgeon makes. This kind of reflective, reasoning-based review after theatre is what separates students who simply watch operations from students who genuinely learn from them.
Think through each question carefully before reviewing the answers:
- What are the five absolute indications for caesarean section that the examiner is most likely to ask about?
- Describe the Pfannenstiel incision: site, direction, and how the underlying layers are entered.
- What is the Joel-Cohen technique, and what is its evidence-based advantage over Pfannenstiel?
- Why is the lower uterine segment preferred for the uterine incision rather than the upper segment?
- A surgeon performing LSCS notices the bladder is unusually high and adherent. What does this suggest, and what does the surgeon do next?
- Name three signs of uterine atony that the recovery room nurse should watch for after CS.
- A woman with previous classical CS is now pregnant again. What is the key management difference compared to a woman with a previous LSCS scar?
- What is the maximum dose of carboprost given at CS for atony, and in which patient is it absolutely contraindicated?
- Which anaesthetic technique is preferred for elective LSCS, and why?
- List five items that must appear in a complete logbook entry for an observed CS.
CLINICAL PEARL
The most dangerous moment in an LSCS on a patient with a previous uterine scar is not the skin incision — it is the bladder flap. In women with adherent bladders from previous surgery, hurried sharp dissection at this step causes the majority of bladder injuries at CS. Watch how experienced surgeons slow down at this step, palpate gently, and use scissors with small bites rather than sweeping cuts. The second highest-risk moment is lateral extension of the uterine incision when the fetal head is deeply impacted: the surgeon should not pull the head through a small incision but rather extend it first or use a disimpacting manoeuvre from below. Understanding these two high-risk moments will make you a far more attentive and useful assistant.
SELF-CHECK
Which of the following statements about the classical caesarean section is CORRECT?
A. The uterine incision is placed in the lower uterine segment at an angle
B. It is preferred in cases of anterior placenta praevia at term because the LUS is thin
C. The scar rupture rate in subsequent pregnancy is approximately 4–9%, much higher than LSCS
D. It can safely allow a trial of labour in subsequent pregnancies in most cases
Reveal Answer
Answer: C. The scar rupture rate in subsequent pregnancy is approximately 4–9%, much higher than LSCS
Classical CS involves a vertical incision through the upper uterine segment. The scar rupture rate in subsequent pregnancy is approximately 4–9% — substantially higher than the <1% risk of LSCS scar rupture. This is why trial of labour after classical CS (TOLACC) is not recommended in standard practice. Anterior placenta praevia at term is an indication for classical CS, but not because the LUS is thin — rather, the LUS in this situation is occupied by placenta and an incision there would cause massive haemorrhage.