Page 9 of 27
OG37.4-5 | D and C with EA-ECC Observation — SDL Guide
Learning Objectives
- Identify the clinical indications for Dilatation and Curettage (D&C) and endometrial aspiration-endocervical curettage (EA-ECC)
- Describe the anatomy of the uterine cavity and cervical canal relevant to intrauterine instrumentation
- Follow the steps of an Examination Under Anaesthesia (EUA) preceding uterine instrumentation
- Observe the sequential steps of a D&C and describe the rationale for each step
- Describe the technique of endometrial aspiration (EA) and endocervical curettage (ECC), including fractional curettage order
- Recognise macroscopic tissue characteristics from uterine curettage and understand specimen handling
- Identify the signs of intraoperative complications — particularly uterine perforation — and observe the immediate surgical response
INSTRUCTIONS
Dilatation and Curettage (D&C) and endometrial aspiration with endocervical curettage (EA-ECC) are among the most commonly performed minor gynaecological procedures, used both for diagnosis (abnormal uterine bleeding, suspected endometrial pathology, cervical cancer staging) and treatment (evacuation of retained products of conception). This module prepares you to observe and assist in these procedures (NMC OG37.4 and OG37.5) with a clear understanding of every step and the reasoning behind it.
References
- DC Dutta's Textbook of Gynaecology, 7th edition, Chapter 18 — Diagnostic and Operative Procedures (textbook)
- Shaw's Textbook of Gynaecology, 16th edition, Chapter 21 — Minor Gynaecological Operations (textbook)
- RCOG Green-top Guideline No. 61 — Management of Endometrial Hyperplasia, 2016 (guideline)
- FOGSI Good Clinical Practice Recommendation — Endometrial Sampling, 2020 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 48-year-old woman with a 6-month history of heavy and irregular menstrual bleeding is admitted to the gynaecological ward. Ultrasound shows an endometrial thickness of 14 mm (normal postmenopausal <4 mm; premenopausal interpretation depends on cycle phase) with an irregular endometrial echo. Her gynaecologist has listed her for an Examination Under Anaesthesia (EUA) followed by Dilatation and Curettage (D&C) and endocervical curettage (ECC) to rule out endometrial carcinoma. As a student on the gynaecology posting, you are asked to attend the procedure. What will the surgeon examine first? Why must the cervical canal be sampled separately before the uterine cavity? What complications must you watch for? This module gives you the knowledge to make this a meaningful observation.
WHY THIS MATTERS
D&C and endometrial sampling remain foundational procedures in gynaecological practice. Despite advances in outpatient pipelle biopsy and hysteroscopy, D&C is still performed for evacuation of retained products of conception (ERPC), for cases where outpatient sampling is inadequate or impossible, and in conjunction with ECC for cervical cancer staging. As a doctor you will refer patients for these procedures, explain them to patients, recognise their complications, and manage post-procedural care. NMC OG37.4 and OG37.5 require you to observe and assist in D&C and EA-ECC respectively — this module prepares you for that experience.
RECALL
Before proceeding, take a moment to recall the relevant anatomy and clinical context. The uterus has an external os (at the ectocervix, accessible per speculum), an endocervical canal (lined by columnar epithelium), and an internal os (the anatomical constriction between the cervical canal and the uterine cavity). The cavity itself is triangular in shape (cornu to cornu superiorly, cervical canal inferiorly) and lined by the endometrium. The position of the uterus — anteverted (common, ~80%) or retroverted (~20%) — determines the direction of instrument insertion: anteverted uterus needs a slightly anterior direction for the sound and curette; a retroverted uterus is instrumented posteriorly. Recall also that abnormal uterine bleeding (AUB) in women over 40 (or at any age if risk factors are present) is an indication for endometrial sampling to exclude malignancy.
When Is D&C or EA-ECC Indicated? Clinical Context
The decision to perform a D&C or endometrial sampling procedure is driven by a specific clinical question, and that question determines everything that follows: the instruments chosen, the anaesthetic approach, whether a specimen is collected, and what the surgeon is looking for. Before you observe any intrauterine procedure, you should already know whether the purpose is diagnostic — to obtain tissue for histological analysis and exclude malignancy or hyperplasia — or therapeutic, such as evacuating retained products of conception, or a combination of both. Understanding the indication transforms you from a passive bystander into an observer who can anticipate each step, understand each instrument choice, and follow the surgeon's reasoning in real time. It also prepares you for the post-procedure discussion that is the most educationally valuable part of any theatre session.
Indications for D&C (diagnostic or evacuative):
- Abnormal uterine bleeding (AUB) in women over 40 or with risk factors (obesity, PCOS, nulliparity, unopposed oestrogen, tamoxifen use) — to exclude endometrial hyperplasia or carcinoma
- Postmenopausal bleeding — any bleeding after 12 months of amenorrhoea in a woman over 45 is endometrial carcinoma until proven otherwise; histology is mandatory
- Incomplete abortion / miscarriage — ERPC (Evacuation of Retained Products of Conception) to remove retained placental or fetal tissue
- Hydatidiform mole — following suction evacuation, a curette confirms clearance (though routine curettage after suction is controversial in modern practice)
- Investigation of infertility — if endometrial factors are suspected
- Prior to insertion of some IUCDs in difficult cases (rarely needed today)
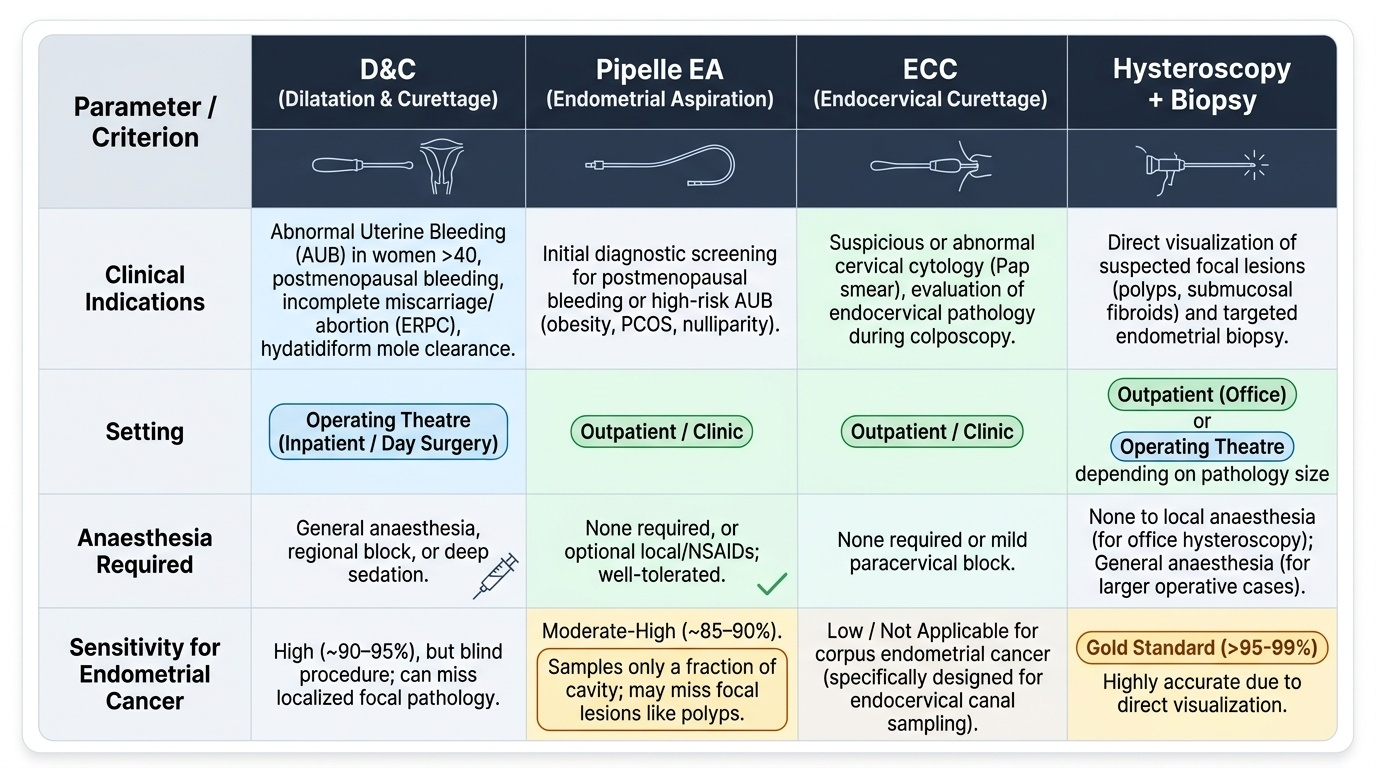
Indications for EA (Endometrial Aspiration):
Endometrial aspiration with a pipelle device or Karman cannula (a flexible plastic cannula connected to a syringe) can often sample the endometrium without full cervical dilatation, making it feasible as an outpatient or clinic procedure. It is preferred in women with an accessible os, adequate cavity depth, and no prior failed outpatient sampling. Pipelle biopsy has a sensitivity of approximately 85–90% for endometrial carcinoma. However, it samples only a fraction of the endometrial surface and may miss focal lesions (polyps, submucosal fibroids) — hence hysteroscopy with targeted biopsy is more accurate for focal pathology.
Indications for ECC (Endocervical Curettage):
ECC samples the endocervical canal and is used to detect endocervical extension of cervical or endometrial carcinoma. In cervical cancer FIGO staging, a positive ECC (endocervical glandular involvement) indicates cervical canal extension and influences staging. ECC is also performed when colposcopy reveals an unsatisfactory transformation zone (not fully visible), when there is a suspicion of endocervical adenocarcinoma, or when Pap smear shows glandular abnormality of endocervical origin.
Fractional curettage — the technique in which ECC is performed BEFORE uterine curettage — is critically important when endometrial carcinoma is suspected. If the endometrial curette is used first, blood and tissue from the uterine cavity contaminates the endocervical canal specimen, making the ECC result uninterpretable. Watch the surgeon perform ECC first in any case where endometrial or cervical malignancy is suspected.
Provided image
Anatomy of the Uterine Cavity and Cervical Canal
Safe and effective intrauterine instrumentation requires a thorough understanding of the three-dimensional anatomy of the uterus, because the instruments are inserted blindly (without direct vision) in a D&C, and the surgeon relies entirely on tactile feedback and knowledge of dimensions and direction to guide the curette. An unexpected anatomical variant — a retroverted uterus, a stenosed internal os, or a uterine anomaly — can turn a routine procedure into a perforation if the anatomy is not correctly assessed beforehand.
The uterine cervix has two apertures: the external os at the ectocervical surface (accessible per speculum examination; the transformation zone is visible here), and the internal os at the upper end of the endocervical canal (a constriction approximately 3–5 mm in diameter in a nullipara, more open in a multipara). Between them is the endocervical canal, approximately 2–3 cm long, lined by columnar epithelium with mucous glands. In premenopausal women with regular cycles, the internal os admits a 3–4 mm probe without forcible dilatation. In postmenopausal women and in nulliparae, the cervix may be atrophic and stenosed, requiring careful dilatation with small dilators before any instrument can be passed.
The uterine cavity is a potential space (the walls are normally apposed) with a triangular cross-section: the two cornua (tubal ostia) at the superior corners, and the internal os at the apex. The cavity is lined by the endometrium, which varies in thickness from 2–3 mm (early proliferative) to 10–14 mm (late secretory) in a normal cycle. The total uterine depth from external os to fundus, measured by a uterine sound, is approximately 6–8 cm in a normal adult uterus at term. In a fibroid uterus the cavity may be enlarged and distorted; in a post-menopausal atrophic uterus it may be as short as 4–5 cm.
The uterine position determines the direction of instrument insertion. In an anteverted uterus (approximately 80% of women), the fundus tilts anteriorly — the sound and curette are directed slightly anteriorly after passing the internal os. In a retroverted uterus (~20%), the fundus tilts posteriorly — the surgeon must direct the instrument posteriorly and may need to straighten the uterus with a tenaculum before sounding. Failure to recognise a retroverted position before forcible insertion is one of the most common causes of uterine perforation.
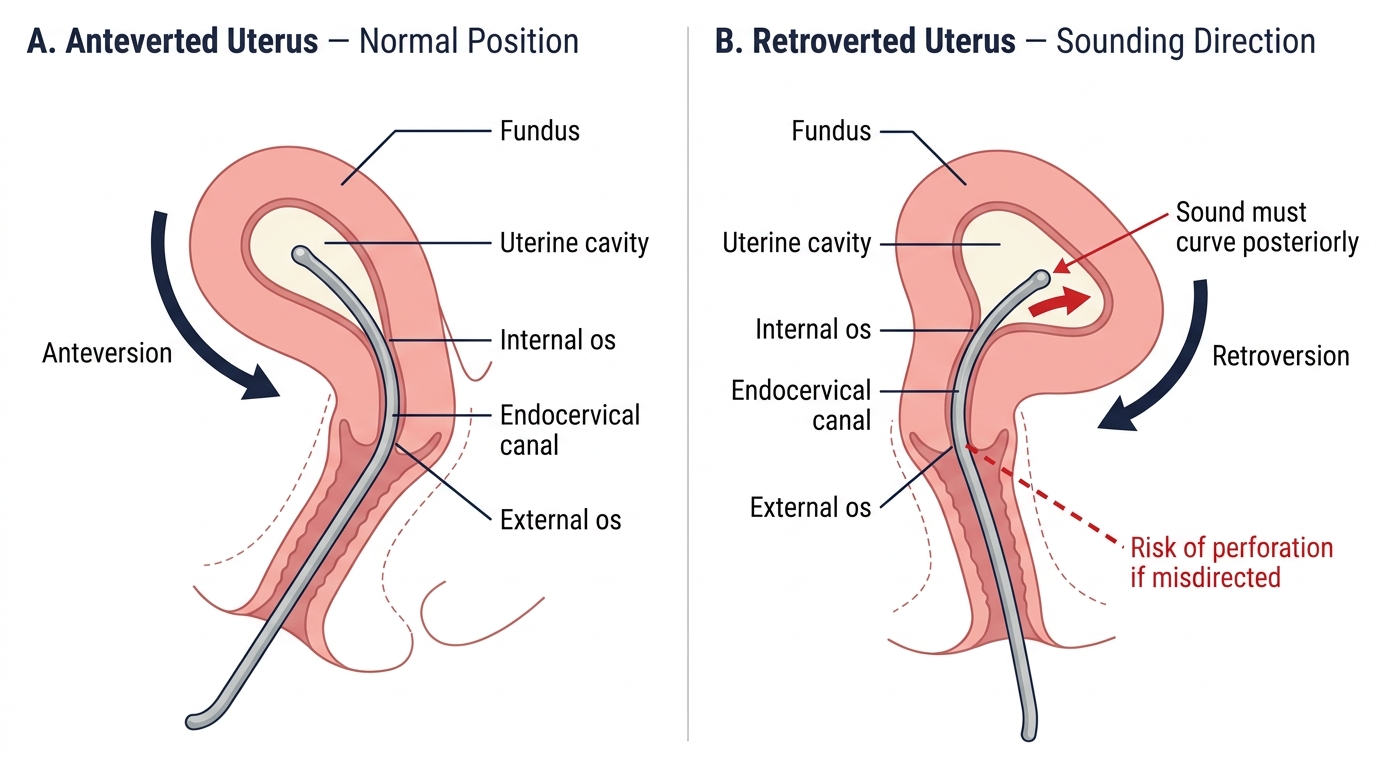
Sagittal Cross-Section of the Uterus: Anteverted vs Retroverted Position and Uterine Sounding Direction
SELF-CHECK
A 52-year-old postmenopausal woman is listed for EUA + D&C + ECC for postmenopausal bleeding. On EUA, the uterus is found to be 8 weeks size with a retroverted, slightly immobile position. When inserting the uterine sound, in which direction should the instrument be angled after passing the external os, and why?
A. Anteriorly, because all uteri are anteverted
B. Posteriorly, because the uterus is retroverted and the fundus tilts posteriorly
C. Laterally toward the right, because the uterus is tilted to the right
D. Straight up vertically, because the retroverted position does not affect the sounding direction
Reveal Answer
Answer: B. Posteriorly, because the uterus is retroverted and the fundus tilts posteriorly
In a retroverted uterus the fundus tilts posteriorly, meaning the uterine cavity curves backward. After passing the external os, the sound must be directed posteriorly to follow the uterine cavity to the fundus. Directing it anteriorly (as you would for an anteverted uterus) will push against the anterior uterine wall and risk perforation anteriorly. Assessing uterine position on EUA before sounding is precisely why EUA precedes instrumentation.
Examination Under Anaesthesia (EUA) — What the Observer Watches
The Examination Under Anaesthesia is not a separate procedure but a critical prelude to any intrauterine instrumentation performed under general or regional anaesthesia. Under anaesthesia, the patient's pelvic floor muscles are relaxed, allowing a far more accurate bimanual assessment of uterine size, position, and mobility than is possible in an outpatient clinic. This examination provides the surgeon with the anatomical information needed to sound and instrumet the uterus safely.
The patient is placed in the lithotomy position (hips flexed and abducted, feet in stirrups) and the perineum is cleaned and draped. The procedure begins with a systematic examination:
Step 1 — Bimanual examination. The surgeon inserts two gloved fingers into the vagina and places the other hand on the lower abdomen. This allows assessment of: uterine size (in weeks of gestation equivalent), uterine position (anteverted or retroverted), uterine consistency (firm = normal; soft = pregnancy), uterine mobility (fixed = adhesions or malignancy; mobile = benign), and any adnexal masses on either side.
Step 2 — Speculum insertion. A bivalved or Sim's speculum (or Cusco's speculum) is inserted to visualise the cervix. The observer watches the surgeon inspect the cervix for erosion, polyps, contact bleeding, or suspicious lesions. The cervical os is identified. If the procedure is a colposcopy-guided ECC, the cervix will also have colposcopic assessment at this point.
Step 3 — Cervical preparation. The anterior lip of the cervix is grasped with a single-tooth vulsellum or tenaculum to stabilise it and provide traction. This straightens the uterocervical axis, particularly important in anteverted or retroverted uteri. Watch how the surgeon notes whether the cervix bleeds easily on contact (a sign of cervical pathology) or is firm and pale.
Findings from EUA are documented: uterine size, position, mobility, os patency, and any unexpected findings. These findings directly determine the next steps: a stenosed os requires careful dilatation; a fixed uterus demands careful sounding to avoid perforation; an unexpected mass may change the operative plan entirely.
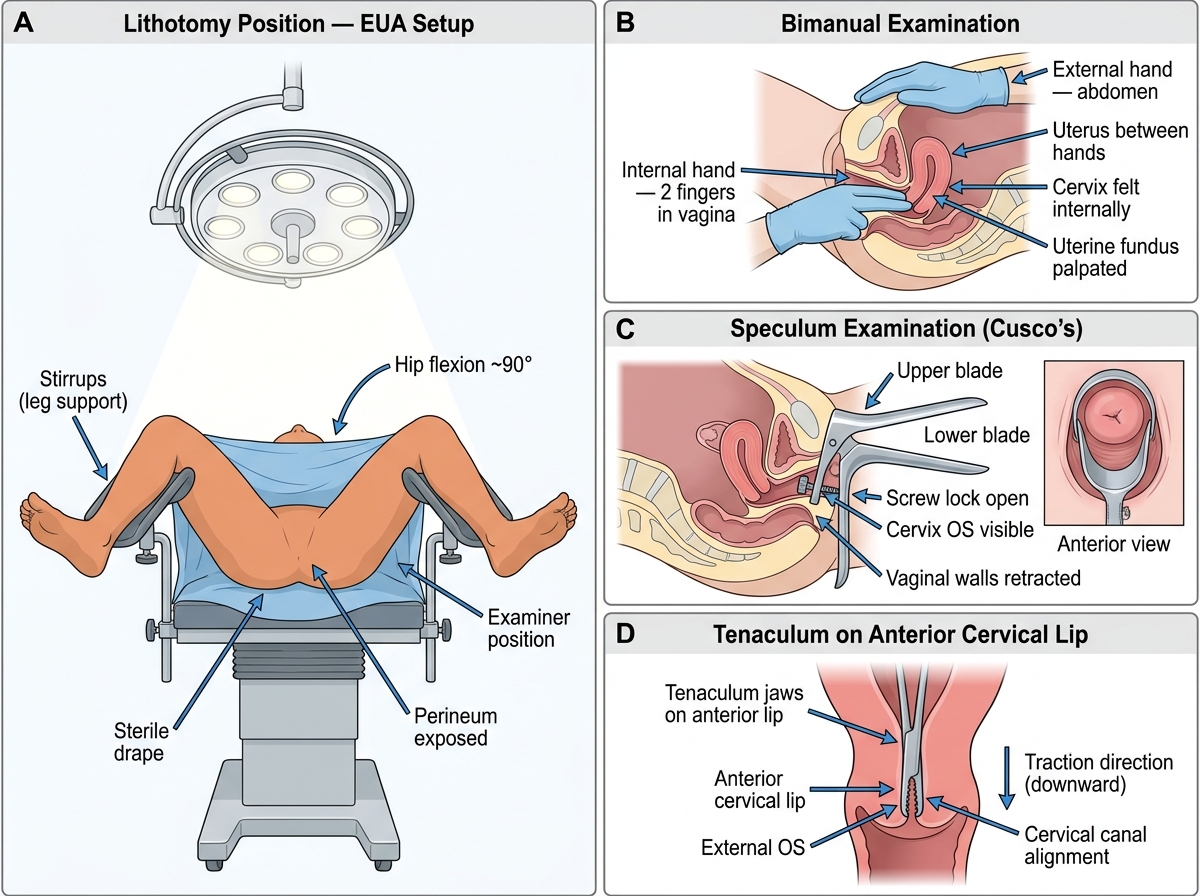
EUA Setup: Lithotomy Position, Bimanual Examination, Speculum, and Tenaculum Placement