Page 11 of 27
OG37.4-5 | D and C with EA-ECC Observation — SDL Guide (Part 3)
Observing Complications — Perforation, Haemorrhage, Cervical Injury
Although D&C is considered a minor gynaecological procedure, its complications — while uncommon — are clinically important and must be recognised immediately to prevent serious morbidity. Observing how experienced surgeons recognise and respond to these complications is a key learning outcome of theatre attendance at these procedures.
Uterine perforation is the most serious intraoperative complication, occurring in approximately 0.1–0.3% of diagnostic D&Cs and at higher rates in post-abortal or post-menopausal atrophic uteri. The classic sign is that the instrument (sound, dilator, or curette) advances beyond the previously determined uterine depth without any resistance — it simply passes into the peritoneal cavity. There is no 'fundal bounce-back' sensation. The observer will notice the surgeon pause abruptly and immediately withdraw the instrument. Additional signs include the sudden absence of the gritty endometrial sensation, a 'sinking' of the instrument through what should be a firm wall, or the appearance of omentum or bowel at the os. The procedure is immediately halted. A perforation with a sound or small dilator (an 'unrecognised perforation') is usually managed conservatively with antibiotics, analgesia, and observation. A perforation with a suction curette — where the curette was actively rotating with suction — may have caused bowel injury and requires urgent laparoscopy to assess the damage.
Cervical laceration occurs when the tenaculum or dilator tears the cervical tissue, either at the tenaculum site on the anterior lip or by forcible over-dilatation creating a radial tear in the cervix. The observer will see fresh bleeding from the cervical lip beyond what is expected. Small lacerations are sutured with absorbable sutures; large tears may extend to the parametrium.
Haemorrhage during or after D&C is uncommon for diagnostic curettage but relevant for ERPC where the placental bed may ooze significantly. If haemorrhage occurs post-ERPC, the surgeon will verify completeness of evacuation (incomplete evacuation is the most common cause of post-procedure bleeding), use intrauterine balloon tamponade, or administer uterotonics (oxytocin infusion, misoprostol).
Late complication — Asherman syndrome: Not an intraoperative complication but important to know: aggressive curettage, especially in post-abortal or post-infective settings, can damage the basal endometrium and cause intrauterine adhesions (Asherman's or Fritsch's syndrome), presenting later with amenorrhoea, hypomenorrhoea, or infertility. This is why a D&C should be as conservative as possible, particularly in women who wish to preserve fertility.
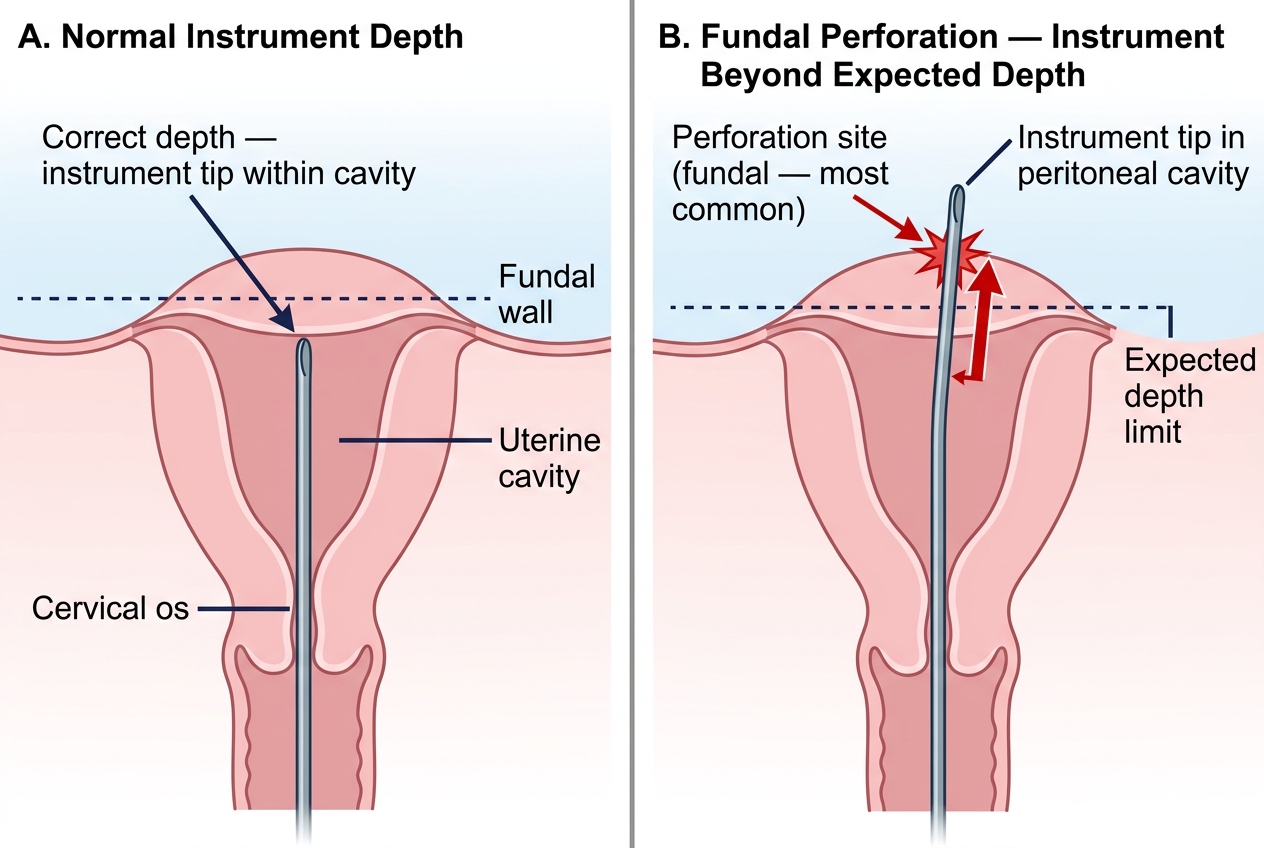
Uterine Perforation: Fundal Perforation vs Correct Instrument Depth
Self-Assessment — D&C and EA-ECC Observation
Use the following questions to consolidate your learning after observing a D&C or EA-ECC. These questions mirror the content and reasoning expected at the SH competency level (observe and assist) and are framed to test understanding rather than rote recall. Work through each question by constructing a reasoned answer before reading the reference material. The value of this deliberate retrieval practice is well established in educational research: the effort of attempting an answer — even imperfectly — strengthens the memory trace far more than passive re-reading. After your theatre session, bring these questions to your post-theatre discussion with your registrar or consultant to verify your answers against clinical practice. You may also compare your answers with a fellow student who observed the same procedure — explaining your reasoning aloud is one of the most effective consolidation strategies available.
Think through each question before reviewing the answers:
- Name three indications for performing ECC rather than endometrial curettage alone.
- Why must ECC be performed before endometrial curettage in cases of suspected malignancy?
- A postmenopausal woman has a stenosed cervical os that will not accept a Hegar 3 dilator. What options does the surgeon have?
- You notice the surgeon's uterine sound has passed to 11 cm without resistance in a woman whose uterus was assessed as 8 weeks size on bimanual. What has happened and what should the surgeon do?
- What macroscopic finding distinguishes chorionic villi (products of conception) from normal endometrium on a gauze specimen?
- Name two late complications of D&C and the patient population at highest risk for each.
- How does a pipelle biopsy differ from a formal D&C in terms of anaesthetic requirement, dilatation needed, and sensitivity for endometrial cancer?
- In a patient with FIGO stage IB2 cervical carcinoma, how does the ECC result alter the staging?
- What is the significance of a 'gritty' sensation versus no resistance felt during curettage?
- What items must appear in the histology request form accompanying uterine curettage specimens?
CLINICAL PEARL
The most preventable complication in intrauterine instrumentation is uterine perforation from failure to assess uterine position before sounding. The single clinical habit that prevents most perforations is this: before inserting any instrument into the uterus, always confirm the position (anteverted or retroverted) on EUA bimanual examination, adjust the instrument direction accordingly, and never advance the sound beyond the first point of fundal resistance. A sound that passes to 9 cm in a uterus bimanually assessed as 7 cm size should stop the procedure until the discrepancy is explained — never advance further. This habit costs 10 seconds; perforation costs an emergency laparoscopy.
SELF-CHECK
After a D&C for AUB, the pathology report returns showing 'proliferative endometrium with no atypia'. What does this mean, and what is the appropriate management?
A. Malignancy confirmed; urgent oncology referral
B. Normal histology for the proliferative phase of the cycle; reassuring if the patient's bleeding settles with hormone management
C. Endometrial hyperplasia without atypia; requires progestin therapy and repeat biopsy
D. Endometrial polyp; surgical resection by hysteroscopy required
Reveal Answer
Answer: B. Normal histology for the proliferative phase of the cycle; reassuring if the patient's bleeding settles with hormone management
Proliferative endometrium without atypia is a normal histological finding in the first half of the menstrual cycle. If AUB was the indication, this result is reassuring (no malignancy or hyperplasia) and suggests that the bleeding may be managed with hormonal therapy directed at the underlying cause of AUB. Endometrial hyperplasia without atypia would require progestin therapy and surveillance biopsy. Malignancy is characterised by cytological atypia and architectural complexity on the histology report.