Page 17 of 27
OG37.7 | First Trimester MTP and Evacuation Observation — SDL Guide
Learning Objectives
- Describe the legal framework under the MTP Act 1971 (amended 2021) for first-trimester MTP and evacuation of incomplete abortion
- Identify the anatomical principles that govern safe uterine evacuation in the first trimester
- Outline the step-by-step technique of manual vacuum aspiration (MVA) and electric vacuum aspiration (EVA)
- Describe how to examine products of conception to confirm completeness of evacuation
- Identify the decision points, signs of complications, and escalation criteria observed during a supervised evacuation procedure
INSTRUCTIONS
Unsafe abortion remains a preventable cause of maternal mortality in India. As a final-year student, you will observe first-trimester MTP and evacuation procedures in the operation theatre. This module prepares you to understand the legal context, anatomical basis, technique, and complication recognition you need to observe meaningfully and assist safely. This is an OBSERVE-AND-ASSIST competency — your role at this stage is structured observation, not independent performance.
References
- DC Dutta's Textbook of Obstetrics, 9th ed., Ch 28 (Abortion) + Ch 29 (MTP) (textbook)
- Shaw's Textbook of Gynaecology, 16th ed., Ch 15 (Abortion) + Ch 22 (Endoscopic and Minimal Access Surgery) (textbook)
- WHO Comprehensive Abortion Care: Clinical Practice Handbook, 2nd ed., 2022 (guideline)
- Medical Termination of Pregnancy Act 1971 (Amendment Act 2021) and MTP Rules 2021 (legislation)
- FOGSI Good Clinical Practice Recommendations on Medical Methods of Abortion, 2022 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 22-year-old woman, six weeks pregnant, is brought to the gynaecology OT for a manual vacuum aspiration under the MTP Act. As you scrub in to observe, the surgeon asks you: 'What position is her uterus in — and why does it matter before I insert the cannula?' A moment later, after the evacuation, she slides the aspirated material into a bowl and turns to you: 'Tell me what you see and whether this is complete.' Your ability to answer these questions — anatomy, legal context, technique, and complication recognition — depends on the structured observation you make today.
WHY THIS MATTERS
Unsafe abortion contributes significantly to India's maternal mortality. The MTP Act 1971 (amended 2021) was enacted to make safe abortion services accessible and to reduce maternal deaths from clandestine procedures. First-trimester suction evacuation — particularly manual vacuum aspiration (MVA) — is the WHO-recommended gold standard for surgical management of early pregnancy failure and induced abortion up to 12–14 weeks. Evacuation of incomplete abortion (partial expulsion of products of conception) is a time-sensitive gynaecological emergency that prevents haemorrhage and sepsis. As a future clinician, you will encounter both situations at district hospitals, primary health centres, and referral facilities. Understanding the procedure from the observer's standpoint equips you to recognise complications early, assist effectively, and counsel patients with accuracy.
RECALL
Before entering the OT, refresh these foundations: (1) The uterus is typically anteverted and anteflexed at the cervico-uterine junction — but significant retroversion or lateral flexion occurs in a subset of women and changes instrument direction. (2) The internal os is the narrow junction between the cervical canal and uterine cavity; it must be gently dilated before any instrumentation. (3) Products of conception (POC) in the first trimester consist of chorionic villi (feathery, white), decidua (membranous), and — after 8 weeks — recognisable embryonic parts. (4) Gestational age determines expected uterine size: at 8 weeks the uterus is approximately plum-sized, at 12 weeks it reaches the symphysis pubis. Confirming gestational age by dates plus uterine size is the starting point of every procedure.
Legal Framework and Indications for MTP
The Medical Termination of Pregnancy Act 1971, substantially amended in 2021, is the statute that governs lawful abortion in India. Understanding this framework is not merely a legal obligation — it determines who can perform the procedure, where, at what gestational age, and for whom. Every practitioner who participates in MTP, even as an observer, must know the law precisely because violations constitute a criminal offence.
Under the MTP Act 2021 and MTP Rules 2021, the key gestational thresholds are as follows. Termination of pregnancy up to 20 weeks may be performed on the opinion of a single Registered Medical Practitioner (RMP) when continuation of the pregnancy would involve risk to the woman's life or health (physical or mental), or where there is a substantial risk of a serious physical or mental abnormality in the child. The 2021 amendment liberalised the upper limit for specific categories of women — 20 to 24 weeks is now permissible on the written opinion of two RMPs, but only for specified categories: survivors of rape or sexual assault, minors (below 18 years), change of marital status (widowhood, divorce), women with physical disabilities (≥40% disability), women in humanitarian settings, and cases of foetal anomaly diagnosed after 20 weeks. Beyond 24 weeks, termination is only permitted where there is a substantial foetal abnormality diagnosed by a State Medical Board constituted under the Act. No gestational limit is set for this route — the Board's approval is the gate.
The Act also protects the woman's confidentiality — no registered medical practitioner is required to disclose the name and identity of the woman whose pregnancy is terminated. The PCPNDT Act 1994 runs in parallel: no ultrasound or investigation may be performed for sex determination at any point, and foetal sex is not disclosed to anyone.
From a clinical standpoint, MTP in the first trimester (up to 12–14 weeks) encompasses two contexts: (a) induced abortion — a conscious choice by the woman within legal provisions — and (b) evacuation of incomplete abortion — where the pregnancy has partially expelled and retained products of conception create haemorrhage and infection risk. The MTP Act applies to the former; evacuation of incomplete abortion may also occur in the context of spontaneous pregnancy loss and constitutes a medical indication regardless of gestational age thresholds for induced MTP.
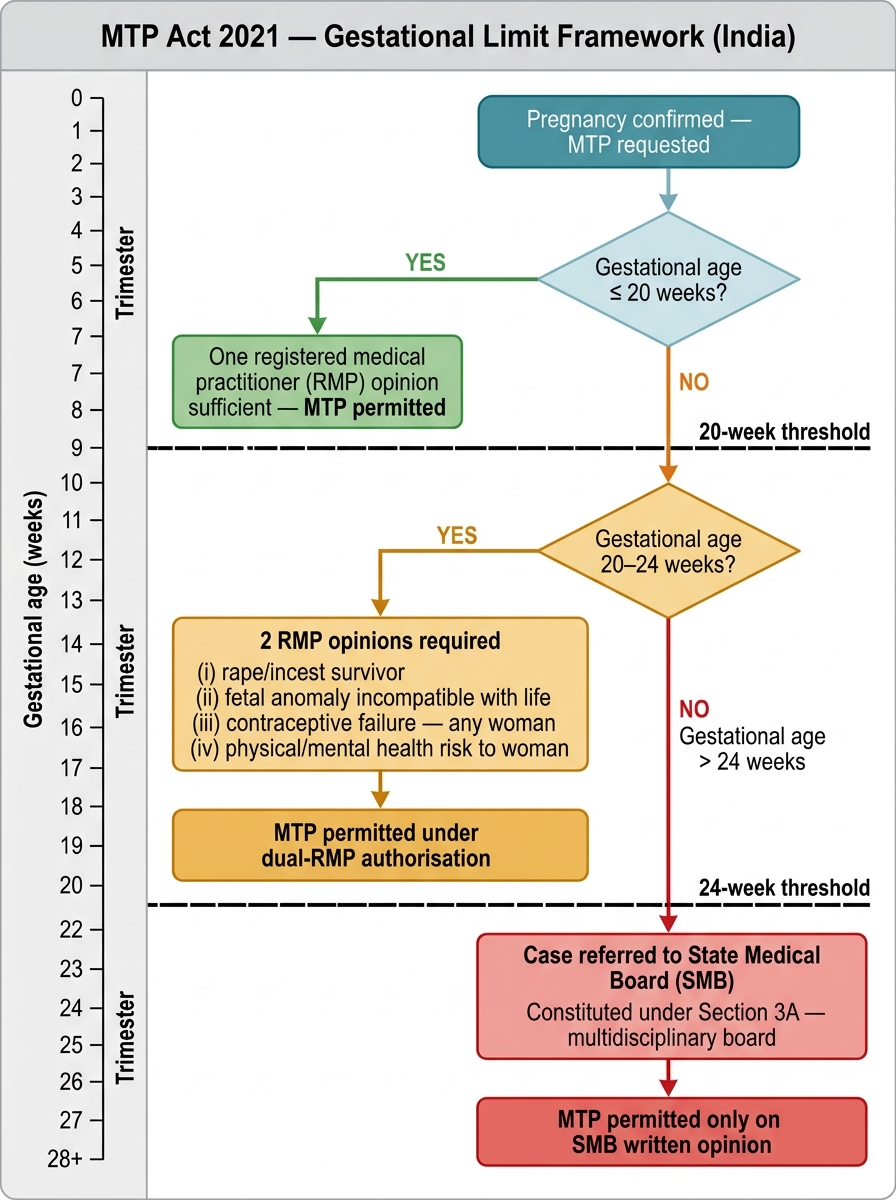
MTP Act 2021 — Gestational Limit Decision Framework
Uterine Anatomy and Anatomical Principles Governing Safe Evacuation
Safe evacuation depends on a thorough understanding of uterine anatomy and orientation. Before any instrument is introduced, the surgeon determines the uterine axis through bimanual examination — a step that is not a formality but a safety check that directly governs instrument direction and the risk of perforation.
The uterus consists of the fundus, corpus (body), isthmus, and cervix. The cervix opens at the external os (visible at speculum examination) and communicates with the uterine cavity through the internal os, separated by the narrow cervical canal. In the reproductive-age woman the cervix is firm with a distinct canal; after misoprostol priming or after a previous vaginal delivery it becomes softer and more easily dilated.
In the classic anteverted-anteflexed uterus, the corpus tilts anteriorly relative to the cervix: instruments introduced through the external os must be directed slightly posteriorly to enter the cervical canal and then anteriorly to follow the uterine cavity — the surgeon makes a subtle arc rather than a straight-line insertion. In a retroverted uterus (present in approximately 20% of women), the corpus tilts posteriorly: instruments must be directed anteriorly initially, or the surgeon may first correct the retroversion by pressing on the fundus abdominally. Failure to assess uterine position before instrumentation is one of the most common contributors to uterine perforation, particularly at the fundus or isthmus where the wall is thinnest.
The endometrial lining in early pregnancy is converted to decidua — a thick, vascular, glandular layer that supports implantation. At the implantation site, chorionic villi of the placenta interdigitate with the decidua. The evacuation cannula and its rotational suction must strip this vascular interface: the characteristic gritty sensation felt by the operator as the cannula moves against the decidualised cavity wall confirms that evacuation is proceeding in the correct tissue plane. Loss of this gritty sensation and entry into a larger, sudden space may indicate perforation.
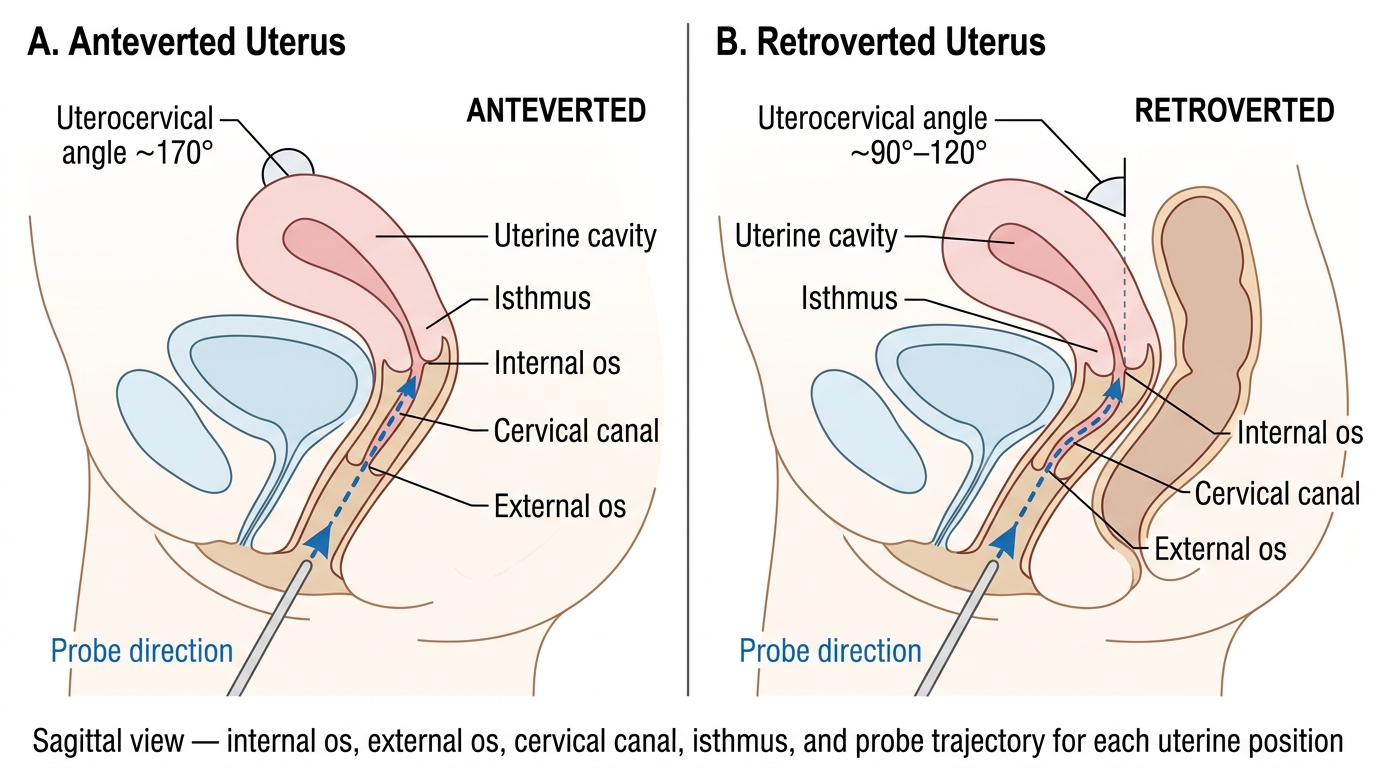
Uterine Position and Probe Direction: Anteverted vs. Retroverted
Technique: Cervical Preparation and Suction Evacuation
The technique of first-trimester evacuation follows a systematic sequence. As an observing student, your goal is to internalise each step's purpose and identify decision points where the surgeon pauses to assess safety. The two primary modalities — manual vacuum aspiration (MVA) and electric vacuum aspiration (EVA) — both use negative pressure to aspirate uterine contents, but differ in their power source, portability, and context of use.
MVA uses a handheld 60 mL syringe with a locking valve to generate approximately 0.6 atmospheres of negative pressure; the aspirated material is collected in the syringe barrel. MVA is suitable up to approximately 12 weeks and is highly portable — it can be used in settings without continuous electricity. EVA uses a powered suction pump; the negative pressure is higher and continuous, making it faster but requiring an electrical supply. EVA is commonly used in operating theatres for gestations up to 12–14 weeks.
The procedure follows these stages:
- Consent, counselling, and contraceptive plan — the woman has given written informed consent; contraceptive counselling is completed before the procedure (copper IUCD CuT 380A can be inserted immediately post-evacuation).
- Positioning — lithotomy position; Sims speculum inserted to expose the cervix under good lighting.
- Cervical preparation — misoprostol 400 µg vaginally or sublingually, 2–4 hours before the procedure, softens and partially dilates the cervix, reducing the force needed for Hegar dilatation and the risk of cervical laceration. For pregnancies below 8 weeks, priming may not be mandatory.
- Tenaculum application — a single-toothed tenaculum is applied to the anterior lip of the cervix at 12 o'clock to stabilise it and correct the uterine axis by gentle traction. This is associated with a brief cramping sensation.
- Sounding the uterus — a uterine sound is passed gently through the internal os to measure uterine depth and confirm the axis; this step is sometimes omitted if ultrasound has already been performed immediately beforehand.
- Cervical dilatation — graduated Hegar dilators (sizes 4 through 8–10, depending on gestational age) are passed sequentially to dilate the internal os without forcing. The surgeon uses the minimal size that allows cannula passage.
- Cannula insertion and evacuation — the MVA/EVA cannula (diameter in mm roughly equals gestational age in weeks) is introduced to the fundus, suction activated, and the cannula rotated 360° while moving in and out through the cavity. The gritty sandpaper sensation confirms productive contact with decidua and villi.
- End-point recognition — evacuation is complete when: the operator feels increased resistance (empty uterine walls appose the cannula), a reddish frothy fluid (without tissue) appears in the cannula, and the uterus contracts around the cannula.
- Post-evacuation uterine check — uterine size is re-assessed by external palpation; it should have reduced to appropriate non-gravid dimensions.
| Feature | MVA | EVA |
|---|---|---|
| Suction source | Handheld 60 mL syringe | Electric pump |
| Max negative pressure | ~0.6 atm | ~0.7–0.8 atm |
| Gestational age range | Up to ~12 weeks | Up to ~12–14 weeks |
| Portability | High (no electricity needed) | Low |
| Noise | Silent | Audible |
| Preferred setting | PHC, field, power-scarce facilities | Hospital OT |
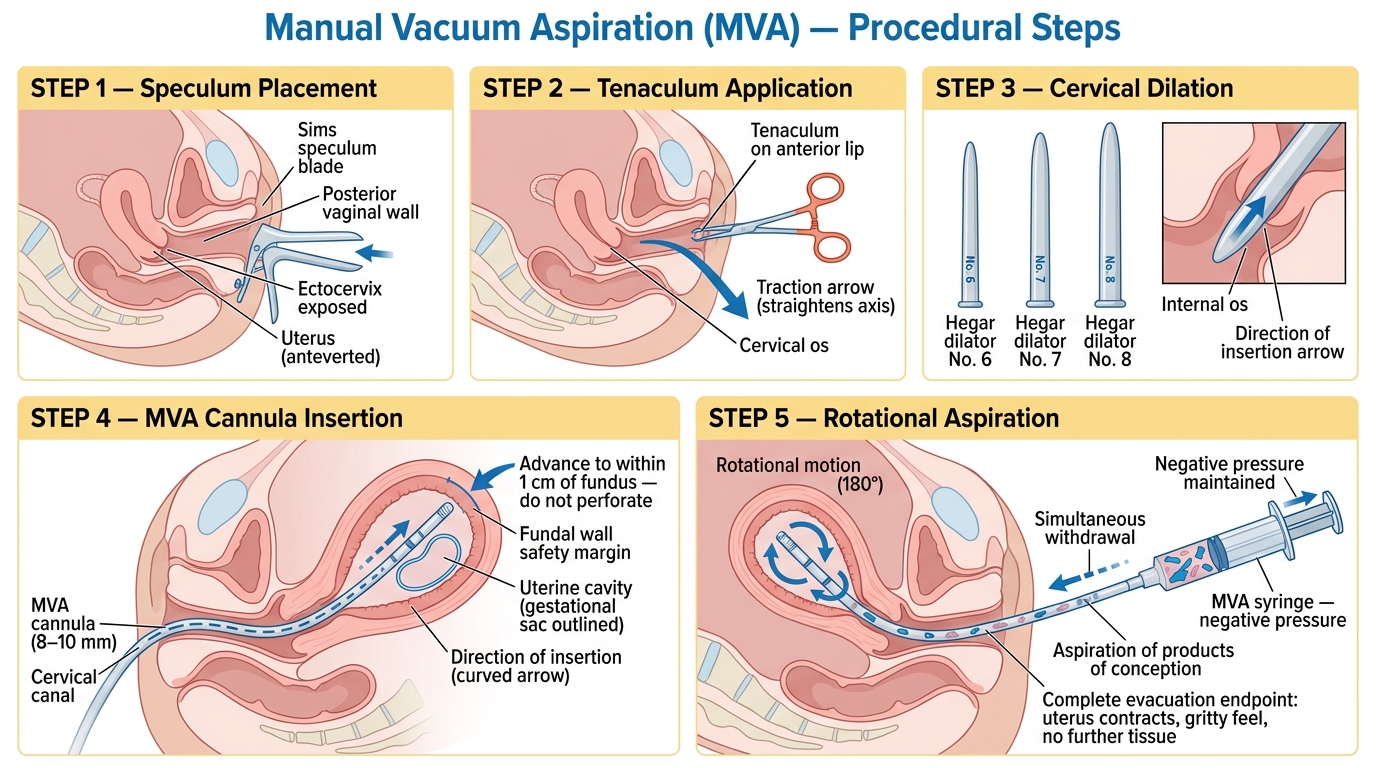
Manual Vacuum Aspiration (MVA) — Step-by-Step Procedural Diagram
SELF-CHECK
Under the MTP Act 2021, which of the following women requires the written opinion of TWO registered medical practitioners for termination of pregnancy?
A. A 28-year-old woman at 10 weeks gestation requesting MTP for contraceptive failure
B. A 16-year-old minor at 22 weeks with a confirmed foetal cardiac anomaly
C. A 35-year-old woman at 18 weeks with gestational diabetes
D. A 25-year-old woman at 8 weeks with documented depression affecting her mental health
Reveal Answer
Answer: B. A 16-year-old minor at 22 weeks with a confirmed foetal cardiac anomaly
The 2021 amendment permits MTP from 20–24 weeks with TWO RMPs' opinion only for specified categories, including minors. At 22 weeks, this 16-year-old minor qualifies for the two-RMP provision. The other three scenarios involve gestations under 20 weeks or conditions that may warrant MTP under the one-RMP provision; they do not require the two-RMP pathway unless gestational age exceeds 20 weeks.