Page 1 of 29
OG4.1 | Fetal and Placental Development — SDL Guide
Learning Objectives
- Describe the major stages of embryonic and fetal development from fertilisation through the fetal period, including key gestational milestones
- Explain the gross and microscopic anatomy of the placenta, including chorionic villi structure, cotyledons, and the maternal and fetal circulations
- Describe the physiological functions of the placenta — gas and nutrient exchange, endocrine production (hCG, hPL, progesterone, oestrogens), and barrier properties
- Identify the key factors that influence fetal growth and development — genetic, maternal nutritional, placental, circulatory, hormonal, teratogenic, and disease-related
- Explain how understanding fetal and placental development underpins clinical management of IUGR, placental insufficiency, fetal dating, drug use in pregnancy, and Rh sensitisation
INSTRUCTIONS
This module builds the foundational embryology and placental science that underlies the entire field of obstetrics. You will explore how a single fertilised cell becomes a term fetus, how the placenta forms and functions as the life-support interface between mother and baby, and what biological factors determine how well the fetus grows. A thorough understanding of these concepts is essential before you can reason about intrauterine growth restriction, placental insufficiency, safe prescribing in pregnancy, or the pathophysiology of pre-eclampsia.
References
- DC Dutta's Textbook of Obstetrics, 9th edition — Chapters 3–5 (Placenta, Fetal Development) (textbook)
- Williams Obstetrics, 25th edition — Chapters 5–6 (Implantation and Placentation, Fetal Development) (textbook)
- Langman's Medical Embryology, 14th edition — Chapters 3–5 (Second Week, Third Week, Organogenesis) (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 28-year-old primigravida at 32 weeks presents with a uterine fundal height of only 26 cm — two centimetres below what is expected for gestation. Her antenatal ultrasound shows an estimated fetal weight on the 3rd centile with absent end-diastolic flow on umbilical artery Doppler. The placenta appears small and inserted close to the internal os. Her obstetrician orders intensified surveillance and counsels her that the baby's growth is compromised, likely due to the placenta not performing its job adequately. Every decision made over the coming weeks — when to deliver, how to monitor the baby, what investigations to order — depends on the clinician's deep understanding of how the placenta normally functions and what goes wrong when it fails. Where did this placenta come from? How is it supposed to work? And what exactly has gone wrong? These are the questions this module will answer.
WHY THIS MATTERS
Fetal and placental development is not a purely academic subject confined to the first trimester. It is the scientific bedrock of almost every obstetric decision you will make. Dating a pregnancy depends on knowing fetal growth milestones. Interpreting a 20-week anomaly scan requires knowing which structures should be visible and when they form. Counselling a patient who inadvertently took a drug in early pregnancy requires knowing the critical windows of organogenesis. Managing intrauterine growth restriction demands understanding how uteroplacental blood flow normally sustains the fetus. Prescribing any drug in pregnancy requires knowing which molecules cross the placental barrier and how. Preventing or managing Rh alloimmunisation rests on understanding the fetomaternal circulation. Competency OG4.1 asks you to describe and discuss all of this — and the knowledge from this module will recur in virtually every week of your clinical obstetric training.
RECALL
Before proceeding, recall the following from your Year-1 Anatomy, Physiology, and Biochemistry:
- Gametogenesis and fertilisation — spermatogenesis produces haploid spermatozoa; oogenesis arrests at meiosis I and completes after fertilisation. Fertilisation occurs in the ampulla of the uterine tube.
- Cell division types — mitosis (somatic, maintaining chromosome number) vs meiosis (gametes, halving to haploid). After fertilisation, the zygote divides by mitosis.
- Ovarian cycle and corpus luteum — the corpus luteum of the ovary produces progesterone and oestradiol to maintain the endometrium; if implantation occurs, hCG rescues it.
- Embryonic germ layers — ectoderm (skin, nervous system), mesoderm (muscle, bone, cardiovascular), endoderm (gut, liver, lung) formed during gastrulation in week 3.
- Haemoglobin structure — fetal haemoglobin (HbF, α₂γ₂) has a higher oxygen affinity than adult HbA (α₂β₂) due to reduced 2,3-DPG binding — a key fact for understanding placental gas exchange.
These concepts form the platform for everything that follows.
Why Fetal and Placental Development Matters Clinically
The clinical relevance of fetal and placental development extends far beyond the first trimester and pervades the entire specialty of obstetrics and gynaecology. To manage a pregnancy safely, a clinician must be able to date the pregnancy accurately — and that depends on knowing what the embryo or fetus looks like at each gestational week. The crown-rump length (CRL) measurable on ultrasound at 11–13 weeks provides the most accurate gestational age estimate, but only because we know precisely how large the fetus is at that age. Every antenatal chart, every growth scan centile, and every biophysical profile draws on a vast body of knowledge about what normal fetal development looks like, week by week.
When a fetus is small — when the estimated weight falls below the 10th centile for gestation — the clinician must determine whether this represents a normally small baby (constitutional) or a growth-restricted baby with placental insufficiency. This distinction, which determines whether intensive surveillance and early delivery are warranted, is impossible to make without understanding how the placenta normally functions. Similarly, when a structural anomaly is found at the 20-week morphology scan, the clinician's interpretation of its severity, likely cause, and prognosis depends on knowing which organ systems form during which weeks of the embryonic period and how teratogens interact with those critical windows.
Prescribing safety in pregnancy is another domain where this basic science is operationally essential. Some drugs cross the placental barrier freely, others are actively excluded, and some — thalidomide being the historical example — cause catastrophic structural defects when given at a specific embryonic week. Drug transfer depends on molecular weight, protein binding, lipid solubility, and active transport — all placental properties grounded in its anatomy and physiology.
Finally, Rh sensitisation — the formation of anti-D antibodies in an Rh-negative mother carrying an Rh-positive fetus — can occur only because fetal red blood cells occasionally cross into the maternal circulation through microscopic placental defects. Understanding the anatomy of the fetoplacental interface explains both why sensitisation is possible and why prophylactic anti-D immunoglobulin prevents it by clearing fetal cells before memory B-cell clones form.
All of these clinical scenarios share a common thread: without a solid grounding in the embryology of the fetus and the anatomy and physiology of the placenta, clinical decision-making in obstetrics lacks its scientific foundation.
Basic Embryology: From Fertilisation to the Fetal Period
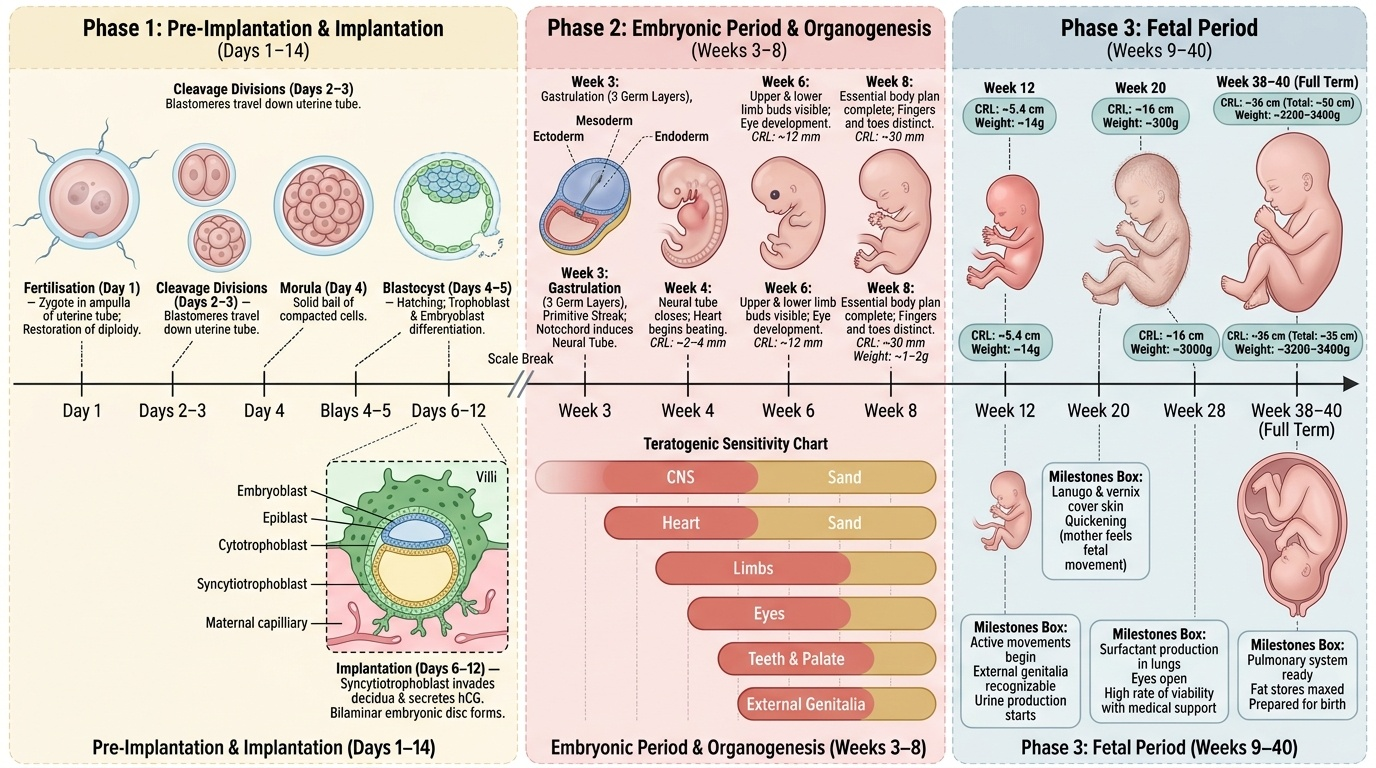
Human development from fertilisation to birth spans approximately 266 days from conception, or 280 days from the last menstrual period (LMP) when the conventional gestational dating system is used. The first eight weeks after fertilisation constitute the embryonic period, during which the fundamental body plan is established and all major organ systems are laid down. From week 9 to delivery is the fetal period, characterised primarily by growth, maturation, and specialisation of structures that were established in the embryonic period.
Provided image
Fertilisation occurs in the ampullary portion of the uterine tube, typically within 24 hours of ovulation. The haploid spermatozoon penetrates the corona radiata and zona pellucida of the secondary oocyte. The cortical reaction immediately prevents polyspermy. Fertilisation triggers the completion of meiosis II in the oocyte, restoring the diploid chromosome number in the zygote and establishing chromosomal sex.
The zygote undergoes a series of mitotic cleavage divisions — first to a 2-cell, then 4-cell, 8-cell stage — as it travels along the uterine tube over the next 3 days. By day 4, it forms the morula (solid ball of 16+ blastomeres). By day 4–5, fluid accumulates between the cells to form the blastocyst, which consists of an outer trophoblast layer (precursor to the placenta) and an inner cell mass or embryoblast (precursor to the embryo proper).
Implantation begins on approximately day 6–7 and is complete by day 10–12. The blastocyst sheds its zona pellucida, adheres to the uterine endometrium (now decidualised), and the trophoblast invades the decidua. The trophoblast rapidly differentiates into the inner cytotrophoblast (cellular, mitotically active, Langhans cells) and the outer syncytiotrophoblast (multinucleated syncytium, invasive, hormonally active). It is the syncytiotrophoblast that begins secreting human chorionic gonadotrophin (hCG) from implantation, rescuing the corpus luteum and preventing menstruation.
Weeks 1–2 see the establishment of the bilaminar embryonic disc (epiblast and hypoblast), the amniotic cavity, and the primary yolk sac. Week 3 is the week of gastrulation — the trilaminar embryonic disc (ectoderm, mesoderm, endoderm) is formed, the notochord induces neural plate formation, and the primitive streak defines the body axis. The cardiovascular system begins to develop in week 3, with the heart tube beating by the end of week 3.
The organogenesis phase (weeks 3–8) is when each major organ system takes form from the three germ layers. This is the period of highest teratogen vulnerability:
- Weeks 3–4: neural tube closure (risk: anencephaly, spina bifida from folate deficiency or valproate), heart begins septation, limb buds appear
- Weeks 5–6: upper and lower limb buds develop, eye and ear primordia form, palate begins formation
- Weeks 6–8: face, palate, and external genitalia form; gonads differentiate
- Week 8 end: embryo has recognisably human features; all major organ systems established
By the end of week 8, the embryo is approximately 3 cm in CRL and weighs about 1 g.
IMPORTED POINT: The all-or-nothing period (weeks 0–2 post-fertilisation) is when the embryo either recovers fully from an insult (total recovery potential due to pluripotent cells) or fails to implant — but major structural defects are NOT the expected outcome of teratogen exposure at this earliest stage.
IMPORTED POINT: From week 9 onward, the organism is called a fetus. The fetal period is dominated by growth and maturation rather than organogenesis.
IMPORTED POINT: Key fetal period milestones to know:
| Gestational Week | CRL / Weight | Key Developments |
|---|---|---|
| 10 weeks | ~3.5 cm CRL | All major organs formed; external genitalia differentiating |
| 12 weeks | ~5.5–6 cm CRL; ~14 g | Urine production begins; intestines return to abdomen; sex identifiable |
| 16 weeks | ~12 cm CRL; ~100 g | Active fetal movements felt by mother (quickening in primigravidas ~18–20 wk); lanugo present |
| 20 weeks | ~16 cm CRL; ~300 g | Midpregnancy anomaly scan; vernix caseosa; myelination begins |
| 24 weeks | ~21 cm CRL; ~600 g | Limit of viability; lung alveoli forming; surfactant production begins |
| 28 weeks | ~25 cm CRL; ~1000 g | Eyes open; viable with intensive care; RDS risk if preterm delivery |
| 32 weeks | ~28 cm CRL; ~1700 g | Rapid brain growth; skull softens; subcutaneous fat deposits |
| 36 weeks | ~32 cm CRL; ~2500 g | Near-term; surfactant adequate; head engagement may occur |
| 40 weeks | ~36 cm CRL; ~3300–3400 g | Term; mature lung; ossification centres of distal femur and proximal tibia present |
IMPORTED POINT: The ossification centre of the distal femoral epiphysis appears at approximately 36 weeks and that of the proximal tibial epiphysis at approximately 40 weeks — forensically and clinically useful for estimating fetal maturity at birth or in perinatal death.
IMPORTED POINT: The embryology timeline:
SELF-CHECK
A woman reports she took a short course of a potentially teratogenic drug during the first 10 days after her last menstrual period, which is approximately 3–4 days post-fertilisation. Which of the following best describes the expected outcome?
A. High risk of major structural malformation affecting heart or limbs
B. All-or-nothing effect — the embryo either survives normally or fails to implant
C. Risk is highest for neural tube defects specifically
D. The drug poses no risk at any stage of the first trimester
Reveal Answer
Answer: B. All-or-nothing effect — the embryo either survives normally or fails to implant
Weeks 0–2 post-fertilisation represent the 'all-or-nothing' period. The embryo at this stage consists of totipotent/pluripotent cells; if damaged, compensation is possible or implantation fails. Major organ-specific structural defects (limb, heart, neural tube) require exposure during organogenesis (weeks 3–8). Option C is wrong because neural tube vulnerability peaks at weeks 3–4 of development, not at day 3–4 post-fertilisation.
Placental Anatomy: Structure and Circulations
The placenta is the vital organ of pregnancy, serving simultaneously as the fetal lung, gut, kidney, liver, and endocrine gland. It forms from the interaction of the trophoblast (fetal tissue) and the decidua (transformed endometrium, maternal tissue). Understanding its anatomy at the gross and microscopic level is prerequisite to understanding its physiology and the basis of placental pathologies such as placenta praevia and placenta accreta.
At term, the normal placenta is a disc-shaped organ approximately 15–20 cm in diameter and 2–3 cm thick, weighing approximately 500 g — roughly one-sixth of the newborn's weight. It has a fetal surface (smooth, covered by amniotic membrane, with the umbilical cord inserting at or near the centre in a normal central insertion) and a maternal surface (irregular, divided into 15–30 lobules called cotyledons by grooves corresponding to septa that project from the basal decidua).
At the microscopic level, the structural unit of the placenta is the chorionic villus. Primary stem villi branch progressively through secondary and tertiary generations to produce the vast surface area (approximately 10–14 m² at term) required for effective exchange. Each villus is covered on its outer surface by the syncytiotrophoblast — a continuous multinucleated layer without intercellular junctions, formed by fusion of cytotrophoblast cells. The syncytiotrophoblast is the hormonally active, invasive, and exchange-active layer in direct contact with maternal blood in the intervillous space. Beneath it lies the cytotrophoblast (Langhans cells) — discrete, mitotically active mononuclear cells that serve as the progenitor pool for the syncytiotrophoblast; these become progressively less prominent after 24 weeks as the villous barrier thins. The villous core contains loose connective tissue (villous stroma) and fetal capillaries that carry fetal blood and converge on umbilical vessels.
The intervillous space is the lake of maternal blood in which the chorionic villi are bathed. Maternal blood enters this space via the spiral arteries — the terminal branches of the uterine arcuate arteries. In normal pregnancy, the syncytiotrophoblast and extravillous cytotrophoblast cells remodel the spiral arteries beginning in the first trimester, transforming them from muscular, high-resistance vessels into wide-bore, low-resistance conduits. This remodelling is essential for adequate uteroplacental blood flow; failure of spiral artery remodelling is the pathological basis of pre-eclampsia and some cases of IUGR.
The fetal circulation through the placenta runs as follows: deoxygenated fetal blood travels from the fetus via two umbilical arteries (which spiral around the single umbilical vein within the umbilical cord, embedded in protective Wharton jelly) to the fetal capillaries of the chorionic villi. After gas and nutrient exchange, oxygenated blood returns to the fetus via the single umbilical vein. A useful memory rule: arteries carry Away from the fetus (deoxygenated), vein Ventures toward the fetus (oxygenated) — the reverse of the systemic convention.
The umbilical cord at term is approximately 50–60 cm long and 1–2 cm in diameter. A single umbilical artery (SUA) is associated with an increased risk of fetal renal and cardiovascular anomalies and warrants a detailed anomaly scan.
IMPORTED POINT: Diagrams to orient your understanding:
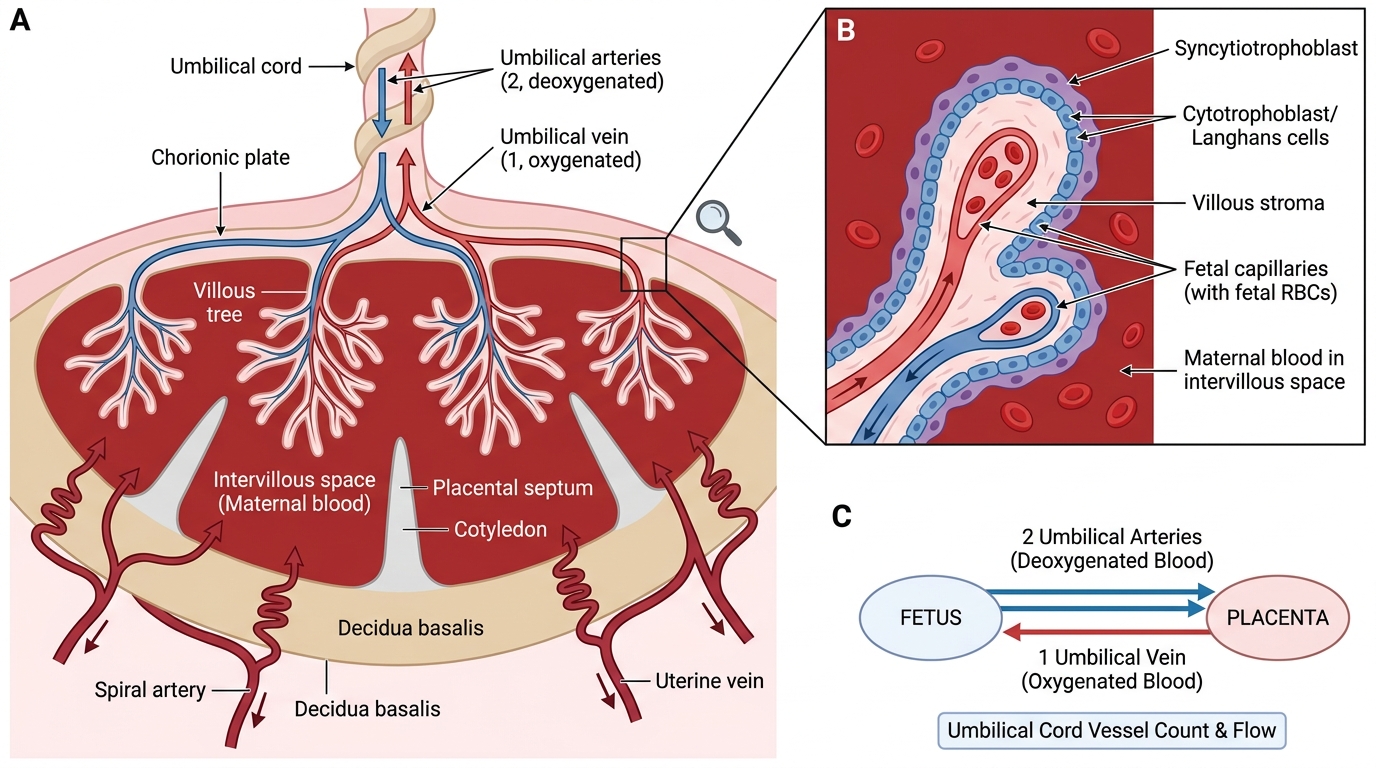
Mature Placenta: Cross-Section, Chorionic Villus, and Umbilical Blood Flow
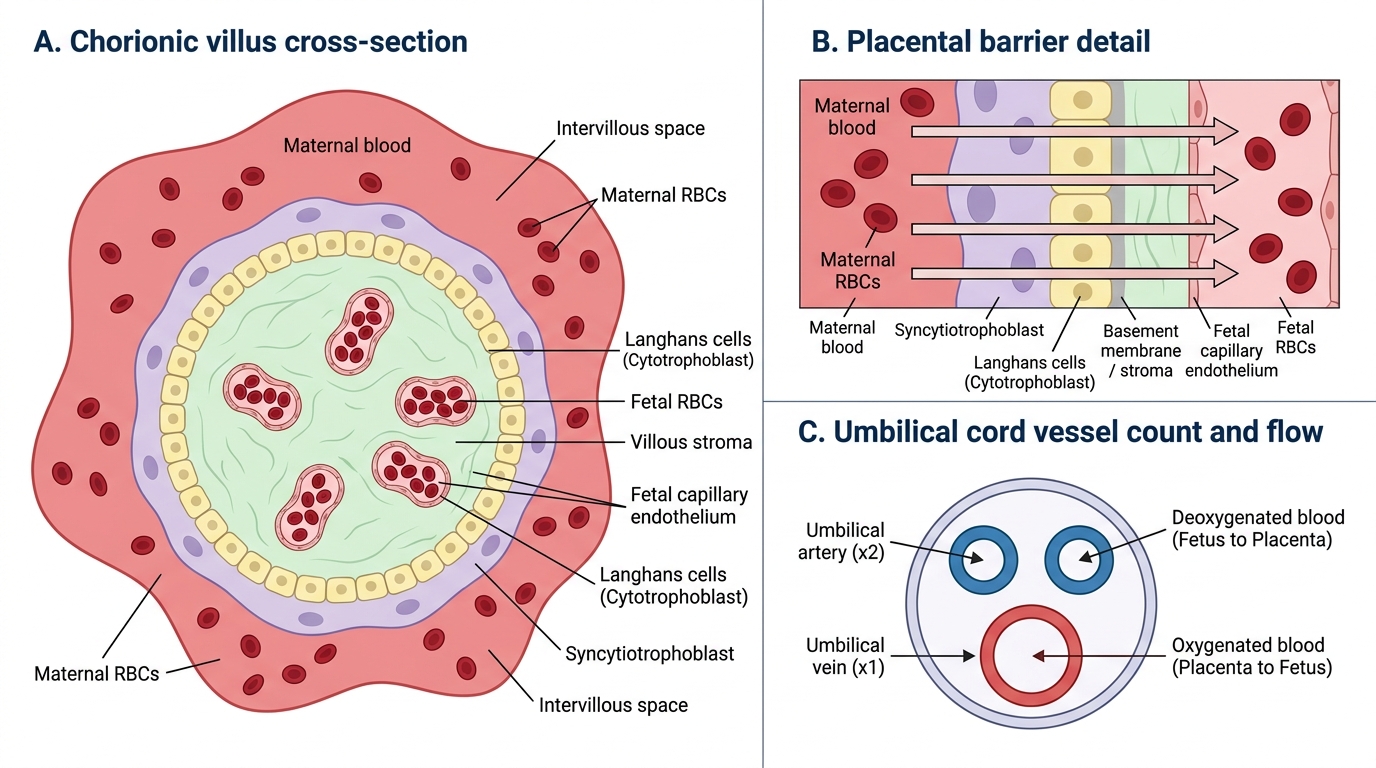
Microscopic Structure of a Chorionic Villus
SELF-CHECK
In the umbilical cord, which of the following correctly describes the vessel count and the direction of blood flow?
A. Two veins carry oxygenated blood from the placenta to the fetus; one artery carries deoxygenated blood from the fetus
B. Two arteries carry deoxygenated blood from the fetus to the placenta; one vein carries oxygenated blood from the placenta to the fetus
C. One artery carries oxygenated blood to the fetus and one vein carries deoxygenated blood away from the fetus
D. Three arteries carry mixed blood in both directions, making counting unreliable
Reveal Answer
Answer: B. Two arteries carry deoxygenated blood from the fetus to the placenta; one vein carries oxygenated blood from the placenta to the fetus
The normal umbilical cord contains two arteries and one vein. The arteries carry deoxygenated, nutrient-depleted fetal blood from the fetus to the placenta. The single umbilical vein carries oxygenated, nutrient-rich blood from the placenta back to the fetus. This is the reverse of the systemic circulation convention where arteries are oxygenated — an important point to remember. A single umbilical artery (SUA) is a significant finding associated with renal and cardiac fetal anomalies.