Page 22 of 29
OG7.1 | Maternal Physiological Changes in Pregnancy — SDL Guide (Part 3)
Gastrointestinal and Endocrine Changes
The gastrointestinal system is profoundly affected by both the hormonal milieu of pregnancy and the mechanical pressure of the enlarging uterus, producing symptoms that range from near-universal morning sickness to rare but serious complications such as intrahepatic cholestasis. Endocrine and metabolic changes reflect the metabolic demands of the feto-placental unit and create the substrate for gestational diabetes.
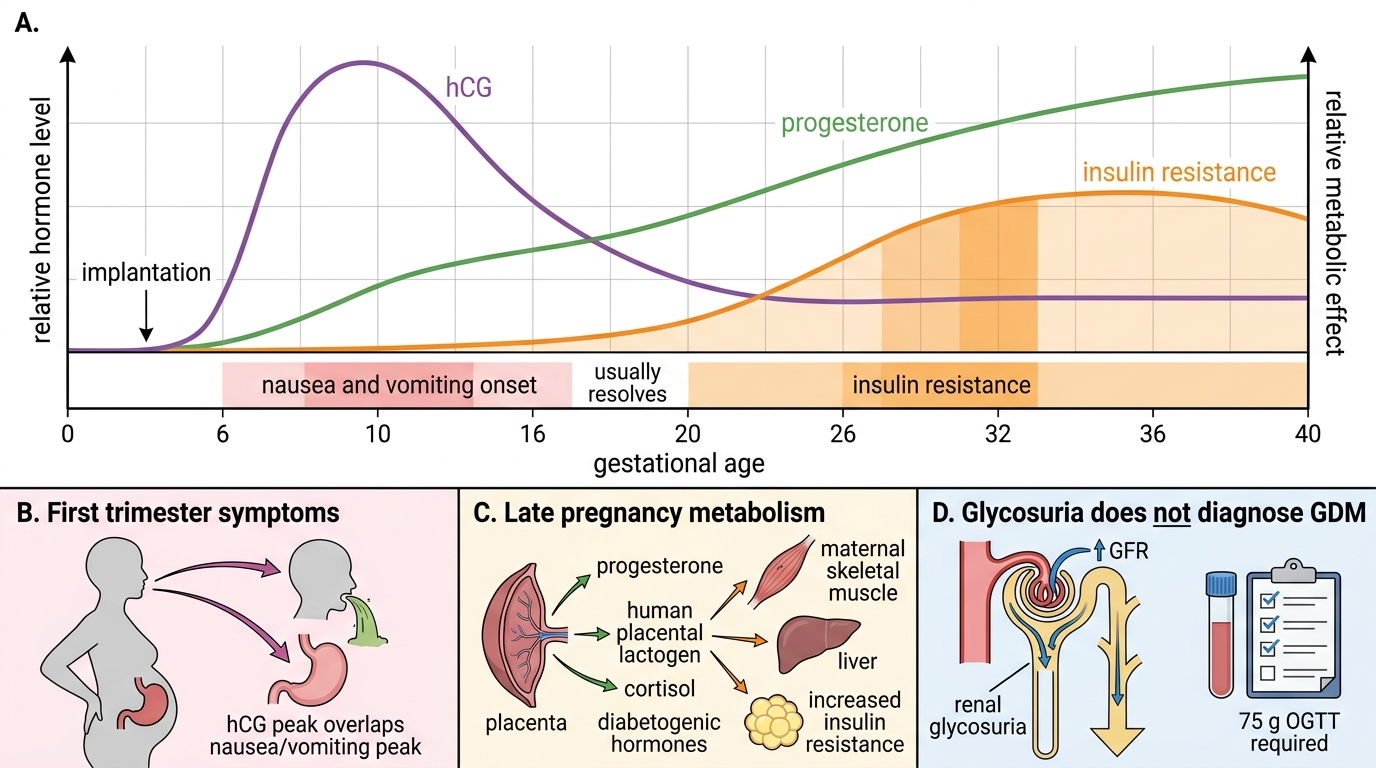
Nausea and vomiting of pregnancy (NVP) — colloquially "morning sickness" though it can occur at any time — affects 50–80% of pregnant women, typically beginning at 6 weeks, peaking at 8–12 weeks, and resolving by 14–16 weeks in most cases. The primary driver is human chorionic gonadotrophin (hCG): NVP severity correlates with hCG levels (it is most severe in molar pregnancy and twin pregnancy, both of which produce very high hCG). Serotonin (5-HT₃) and vestibular stimulation also contribute. Hyperemesis gravidarum — severe, persistent vomiting with weight loss >5%, ketonuria, and electrolyte imbalance — affects approximately 1% of pregnancies and requires hospitalisation.
The lower oesophageal sphincter (LOS) tone falls progressively during pregnancy under progesterone's smooth muscle relaxant effect. Combined with delayed gastric emptying (also progesterone-mediated) and the mechanical upward displacement of the stomach by the uterus, this produces gastro-oesophageal reflux (heartburn), affecting up to 70–80% of pregnant women, worsening in the third trimester. The risk of aspiration during anaesthesia (Mendelson's syndrome) is increased — a key reason why pregnant women requiring general anaesthesia are treated as having a full stomach.
Constipation is extremely common (affects ~40%), driven by progesterone-mediated reduction in colonic motility and increased water absorption from the colon, as well as iron supplementation. Haemorrhoids frequently develop or worsen due to increased venous pressure from the gravid uterus compressing the inferior vena cava and pelvic veins.
Thyroid function changes: oestrogen stimulates the liver to produce more thyroid-binding globulin (TBG), raising total T₄ and T₃ levels. Free T₄ and TSH remain essentially within normal range in an uncomplicated pregnancy (hCG has weak TSH-like activity, slightly suppressing TSH in the first trimester). Testing thyroid function requires trimester-specific reference ranges.
Insulin resistance increases progressively during the second and third trimesters, driven by human placental lactogen (hPL), progesterone, oestrogen, and cortisol. This is physiological — it diverts glucose toward the fetus by making maternal tissues less responsive. In women with adequate pancreatic beta-cell reserve, compensatory hyperinsulinaemia maintains normoglycaemia. In women with limited reserve, this insulin resistance unmasks gestational diabetes mellitus (GDM), explaining why GDM typically presents in the third trimester when insulin resistance peaks.
Metabolic rate and weight gain: basal metabolic rate increases by approximately 15–20% by the third trimester. Total weight gain in a normal-BMI woman is 11.5–16 kg (IOM 2009 guidelines), distributed approximately as: fetus (~3.3 kg), placenta (~0.7 kg), amniotic fluid (~0.8 kg), uterus (~0.9 kg), breasts (~0.4 kg), blood volume (~1.5 kg), extracellular/interstitial fluid (~2.0 kg), and fat stores (~3.5 kg).
Pregnancy Hormone Timeline and Clinical Correlations
SELF-CHECK
A 26-year-old woman at 24 weeks gestation has a urine dipstick positive for glucose (2+). Her random blood sugar is 95 mg/dL. What is the most appropriate next step?
A. Reassure — glycosuria with a normal random blood sugar confirms gestational diabetes is excluded
B. Start insulin — glycosuria at this gestation always indicates gestational diabetes
C. Perform a formal OGTT (75 g) as per DIPSI or IADPSG criteria — glycosuria in pregnancy is physiological and does not reliably reflect blood glucose
D. Repeat urine dipstick in 4 weeks — one positive result is insufficient
Reveal Answer
Answer: C. Perform a formal OGTT (75 g) as per DIPSI or IADPSG criteria — glycosuria in pregnancy is physiological and does not reliably reflect blood glucose
Physiological glycosuria is common in pregnancy because the increase in GFR exceeds tubular reabsorptive capacity — glucose spills into the urine even at normal blood glucose levels. A urine dipstick cannot reliably diagnose or exclude GDM. Formal OGTT (75 g glucose, using DIPSI: 2-hour value ≥140 mg/dL; or IADPSG: fasting ≥92, 1-hour ≥180, 2-hour ≥153 mg/dL) is required.
Mechanisms and Determinants of Physiological Adaptation
The physiological changes of pregnancy are not random — they are orchestrated by a specific set of hormones produced primarily by the placenta and corpus luteum, each acting on defined molecular targets in multiple organ systems. Understanding the hormonal drivers enables the clinician to reason about why changes occur when they do and why some changes are more pronounced in some pregnancies than others.
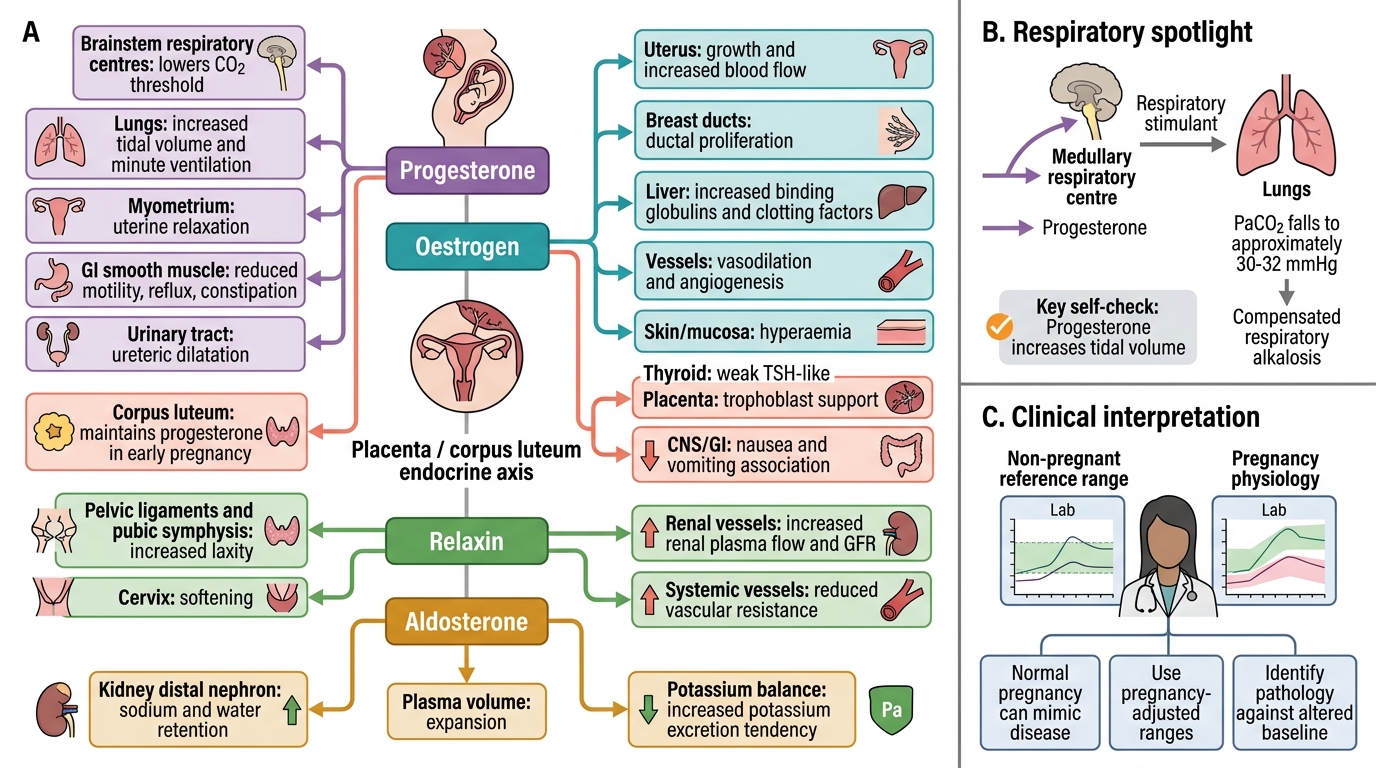
Progesterone is the master regulator of pregnancy physiology. Produced first by the corpus luteum and then primarily by the placenta after 8–10 weeks (the luteoplacental shift), progesterone levels rise throughout pregnancy to reach ~150 ng/mL at term. Its actions are ubiquitous: smooth muscle relaxation (uterine quiescence, LOS relaxation, constipation, ureteral dilation), respiratory stimulation (increased TV and minute ventilation), thermogenesis (the elevated basal temperature of the luteal phase), and immunological tolerance of the fetal allograft. Progesterone is the dominant driver of GI symptoms, respiratory alkalosis, and urological changes.
Oestrogen (primarily oestradiol and oestriol, the latter being uniquely placental) rises from the first trimester and reaches very high levels at term (~20–30 ng/mL oestradiol; oestriol from fetal adrenal-placental cooperation). Oestrogen drives uterine hypertrophy, breast ductal growth, genital vascular engorgement (Chadwick's sign), TBG synthesis, increased coagulation factor production, and sodium and water retention. It also upregulates oxytocin receptors near term, preparing the uterus for labour.
Human chorionic gonadotrophin (hCG) is produced exclusively by trophoblastic tissue. It peaks at approximately 8–10 weeks gestation (up to 100,000 mIU/mL) and then falls to a plateau of ~10,000–20,000 mIU/mL in the second trimester. Its primary role is corpus luteum maintenance to sustain progesterone production in early pregnancy. Its structural similarity to TSH (shared alpha subunit) accounts for first-trimester TSH suppression and gestational hyperthyroidism. hCG is also the primary driver of nausea and vomiting in the first trimester.
Human placental lactogen (hPL) rises progressively throughout pregnancy and is the primary mediator of insulin resistance in the second and third trimesters. It acts as a counter-insulin hormone, mobilising maternal free fatty acids and amino acids and diverting glucose to the fetus — a form of fetal sparing at the cost of maternal glucose intolerance.
Relaxin is produced by the corpus luteum and placenta. It softens the pubic symphysis and sacroiliac joints (allowing pelvic expansion for delivery), reduces uterine contractility, and contributes to renal vasodilation (partially responsible for the rise in GFR in early pregnancy).
Aldosterone and the renin-angiotensin-aldosterone system (RAAS) are activated from early pregnancy, promoting sodium and water retention to expand plasma volume. Despite 10-fold increases in aldosterone, the expected hypertension is counteracted by progesterone's natriuretic effect and the vasodilatory action of oestrogen and nitric oxide.
The haemodynamic mechanism of cardiac output rise deserves emphasis. The primary stimulus is the development of the uteroplacental circulation — a large, low-resistance arteriovenous shunt that increases venous return and activates baroreceptors to stimulate CO. Progesterone and nitric oxide reduce SVR, lowering afterload and further increasing CO. Increased erythropoietin (from the placenta and maternal kidneys) drives red cell mass expansion, which alongside plasma volume expansion maintains tissue oxygen delivery despite lower haemoglobin concentration.
Pregnancy Hormones and Target-Organ Effects
SELF-CHECK
Which hormone is primarily responsible for the increased tidal volume and respiratory alkalosis seen in pregnancy?
A. Oestrogen — drives vascular growth and fluid retention
B. Progesterone — acts as a respiratory stimulant lowering the CO₂ threshold
C. hCG — peaks in the first trimester and drives early respiratory changes
D. hPL — mediates metabolic changes including respiratory drive
Reveal Answer
Answer: B. Progesterone — acts as a respiratory stimulant lowering the CO₂ threshold
Progesterone is a potent respiratory stimulant that acts on central respiratory centres, lowering the threshold for CO₂-driven ventilation. This drives the characteristic increase in tidal volume (40%) and minute ventilation (30–50%) of pregnancy, resulting in a fall in PaCO₂ to ~30–32 mmHg — compensated respiratory alkalosis. This effect explains why breathlessness is near-universal in pregnancy even in the absence of cardiopulmonary disease.
Clinical and Applied Significance
The physiological changes of pregnancy translate directly into a set of clinical rules for interpreting investigations, counselling patients, and making therapeutic decisions. A clinician who applies non-pregnant reference ranges to pregnant women will systematically over-investigate normal findings and under-diagnose pathology that presents against a shifted baseline. This section consolidates the key applied principles that directly govern everyday obstetric decision-making — from reading a blood result to positioning a patient in labour.
Every system covered in this module contributes at least one clinically critical shift in what counts as a normal value. Haematology, renal function, coagulation, blood pressure, blood gases, and urine testing all require pregnancy-specific interpretation. Errors in these domains lead to either unnecessary investigation and patient anxiety, or missed diagnoses with potential for serious harm. The principles below are the minimum clinical framework a final-year student must internalise before entering obstetric practice.
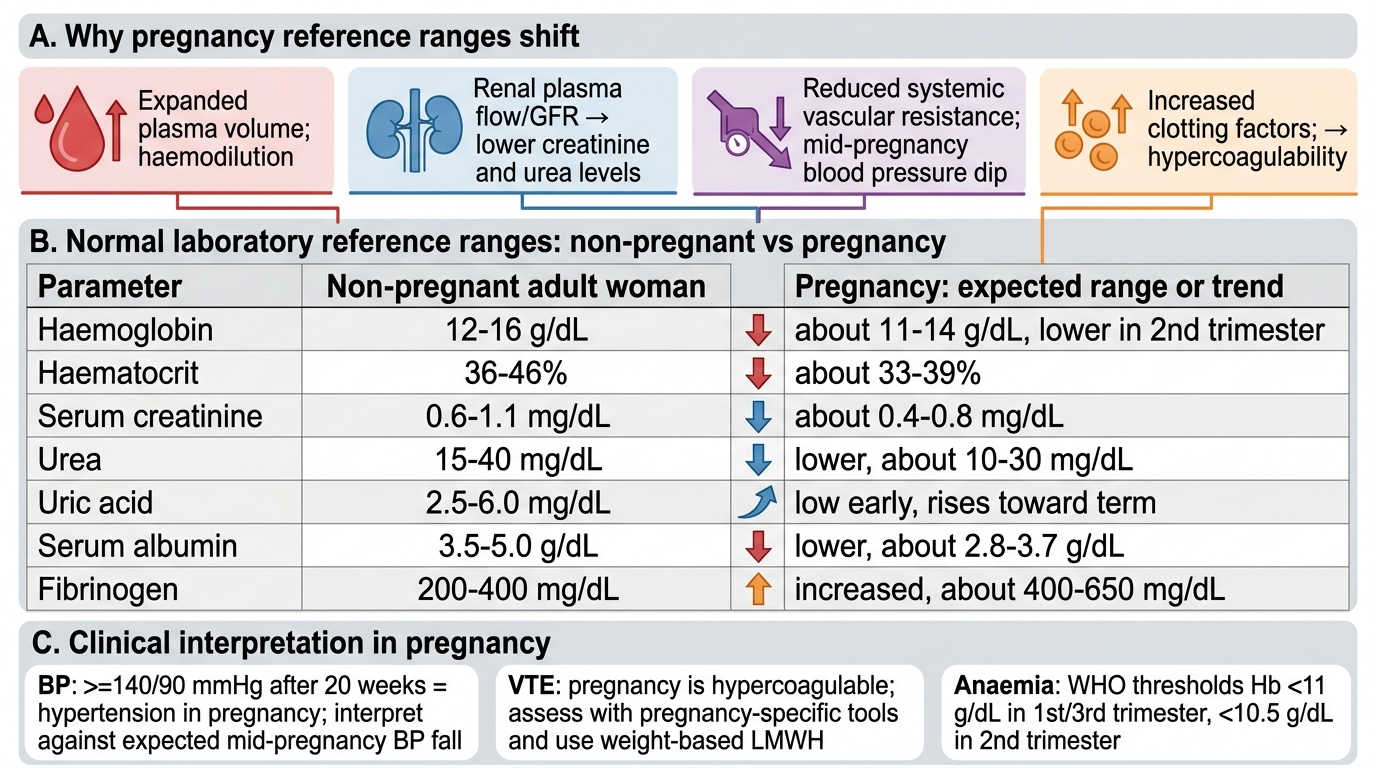
Laboratory interpretation in pregnancy: virtually every biochemical and haematological parameter has a pregnancy-specific reference range. The key shifts to internalise are:
| Parameter | Non-pregnant norm | Pregnant norm | Clinical implication |
|---|---|---|---|
| Haemoglobin | 12–16 g/dL | ≥11 g/dL (WHO — 1st/3rd trimester) | Hb 10.5–11 g/dL is borderline; below 11 g/dL needs evaluation |
| Haematocrit | 36–48% | 32–36% at nadir | Physiological dilution; don't treat unless symptomatic or below WHO threshold |
| Serum creatinine | 0.6–1.0 mg/dL | 0.4–0.6 mg/dL | Creatinine ≥0.9 mg/dL in pregnancy = significant impairment |
| Serum urea | 2.5–6.5 mmol/L | 2.0–4.0 mmol/L | Falls due to hyperfiltration |
| Serum albumin | 3.5–5.0 g/dL | 3.0–4.5 g/dL | Falls due to dilution; do not misinterpret as malnutrition |
| Fibrinogen | 2–4 g/L | 4–6 g/L at term | Elevated — protective but contributes to hypercoagulability |
| WBC | 4,000–11,000/µL | 9,000–16,000/µL | Physiological neutrophilia; leukocytosis in labour up to 25,000 normal |
Pregnancy-Adjusted Laboratory Reference Ranges
Blood pressure interpretation: because SVR falls and blood pressure drops physiologically in mid-pregnancy, a BP of 130/80 mmHg at 20 weeks is not the reassuring normal it would appear to be in a non-pregnant patient — it may represent early hypertensive disease if the patient's pre-pregnancy BP was 100/70. Conversely, a BP of 125/80 mmHg at 36 weeks may be normal for a woman whose baseline was 120/75. The key rule is: any BP ≥140/90 mmHg after 20 weeks constitutes hypertension in pregnancy (pre-eclampsia threshold), and it is defined against the backdrop of expected physiological hypotension — not against non-pregnant norms.
VTE risk: the hypercoagulable state of pregnancy means that VTE is the leading cause of direct maternal death in developed countries. Risk assessment should incorporate pregnancy-specific VTE risk tools (RCOG/SOGC), not Caprini scores designed for non-pregnant surgical patients. Low-molecular-weight heparin (LMWH) dosing is higher in pregnancy due to expanded volume of distribution and increased renal clearance — doses are weight-based and adjusted in renal impairment (using pregnancy-specific creatinine thresholds).
Anaemia diagnosis: the WHO haemoglobin thresholds for pregnancy (11 g/dL in 1st and 3rd trimester, 10.5 g/dL in 2nd trimester) exist because the physiological dilutional nadir occurs at approximately 28 weeks. Haemoglobin below these thresholds requires evaluation — the cause may be iron deficiency (most common), folate deficiency, or haemoglobinopathy. A low MCV with low serum ferritin confirms iron deficiency; a normal MCV with low haemoglobin in the second trimester is most often physiological dilutional anaemia. The two must be distinguished before prescribing high-dose iron, which has its own gastrointestinal side effects and is unnecessary in purely dilutional anaemia.
Aortocaval compression after 20 weeks mandates that patients awaiting obstetric procedures not be kept supine for prolonged periods. The standard recommendation is left lateral tilt of at least 15° (a wedge under the right hip). Failure to do this can reduce uteroplacental blood flow and precipitate fetal distress even in an otherwise uncomplicated procedure.
Drug dosing in pregnancy: increased GFR means renally-cleared drugs may have shorter half-lives and require dose increases (e.g., ampicillin, cephalosporins in pyelonephritis treatment). Increased plasma volume increases the volume of distribution of water-soluble drugs. Reduced serum albumin alters protein binding of highly bound drugs. These pharmacokinetic shifts mean that standard non-pregnant dosing may be subtherapeutic for some drugs in pregnancy.
CLINICAL PEARL
The most dangerous mistake in obstetric medicine is applying non-pregnant reference ranges to pregnant women. Three specific examples cost lives: (1) creatinine — a value of 0.9 mg/dL triggers no concern on a standard laboratory report, but in pregnancy it represents near-halving of normal GFR and should prompt urgent renal evaluation; (2) haemoglobin — a value of 11.5 g/dL is normal by non-pregnant standards but should be evaluated in a third-trimester patient if symptoms suggest iron deficiency, since the physiological nadir has passed; (3) PaCO₂ — a value of 40 mmHg is textbook normal outside pregnancy but represents significant CO₂ retention in a term patient, who should be running at ~30–32 mmHg. Always apply pregnancy-specific reference ranges — and if in doubt, ask: 'Is this a normal finding for a woman of X weeks gestation?'