Page 2 of 30
OG8.1 | Antenatal Care Objectives and Risk Screening — SDL Guide (Part 2)
Identifying High-Risk Pregnancies: Screening Criteria and Classification
Risk screening is the process by which a clinician identifies pregnant women whose pregnancy characteristics predict a greater probability of adverse outcomes compared with the general obstetric population. This is not a diagnostic exercise — it is a probabilistic triage designed to match intensity of surveillance to likelihood of complication. The inverted pyramid is operationalised through systematic risk-factor assessment at every ANC contact, because a woman's risk classification is dynamic: it can change at any visit as new findings emerge. A woman who is classified as low-risk at booking may develop hypertension at 28 weeks, or be found to carry a malpresenting fetus at 36 weeks, transforming her risk status and her management plan. Systematic, structured screening at every contact — not a single triage at booking — is what makes this process clinically meaningful and what the inverted pyramid requires.
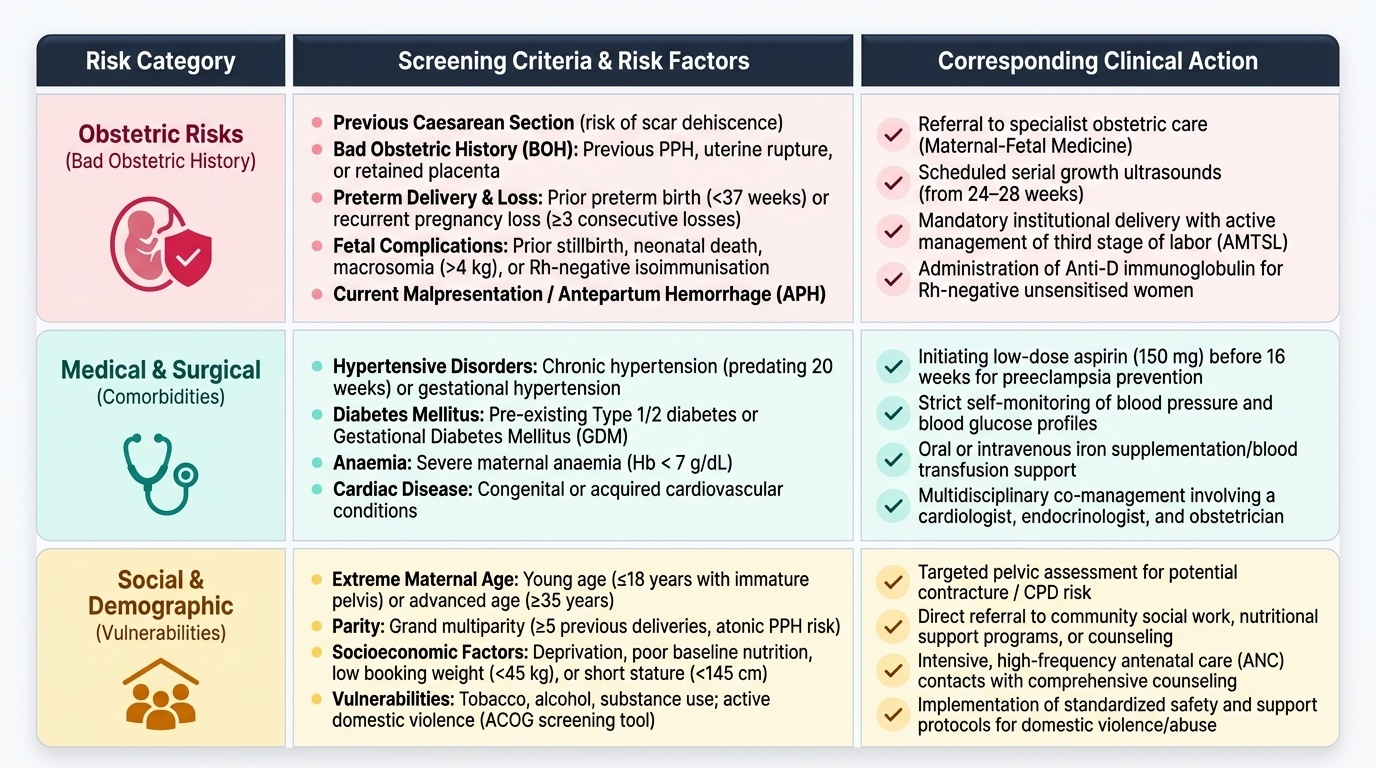
High-risk factors are conventionally grouped into four categories, each reflecting a distinct mechanism by which adverse outcomes are generated:
1. Demographic and social risk factors:
- Age <18 years (immature pelvis, nutritional deficiencies, anaemia, high rates of preterm birth and low birth weight)
- Age >35 years (increased risk of chromosomal anomalies, hypertensive disorders, gestational diabetes, placenta praevia)
- Grand multiparity (≥5 previous deliveries): atonic PPH, malpresentation, obstructed labour risk
- Socioeconomic deprivation, poor nutrition, < 45 kg body weight at booking, height <145 cm (pelvic contracture risk)
- Tobacco, alcohol, substance use; domestic violence (screen systematically using ACOG screening tool)
2. Obstetric history risk factors (the 'bad obstetric history'):
- Previous caesarean section (uterine scar, risk of scar dehiscence and placenta accreta)
- Previous PPH, retained placenta, uterine rupture
- Previous preterm birth (<37 weeks), recurrent pregnancy loss (≥3 consecutive losses before 20 weeks)
- Previous stillbirth or perinatal death of unexplained cause
- Previous macrosomic baby (>4 kg), diabetic pregnancy, or baby with congenital anomaly
- Rh-negative blood group with unsensitised or sensitised status (isoimmunisation risk)
3. Medical and surgical comorbidities:
- Hypertensive disorders: chronic hypertension (predates 20 weeks or pre-pregnancy), renal disease, systemic lupus erythematosus
- Diabetes mellitus (pre-gestational type 1 or type 2) — much higher risk than gestational diabetes alone
- Cardiac disease (rheumatic heart disease commonest in India; functional class NYHA III/IV = very high risk)
- Severe anaemia (Hb <7 g/dL), thalassaemia trait with partner at risk
- Epilepsy, thyroid disorders, autoimmune conditions, chronic lung disease
4. Current pregnancy findings:
- Multiple pregnancy (twins, triplets): higher risk across all categories
- Antepartum haemorrhage (any bleeding after 20 weeks)
- Malpresentation after 36 weeks (breech, transverse lie)
- IUGR or fetal growth restriction (EFW <10th centile)
- Severe hyperemesis gravidarum (dehydration, electrolyte imbalance)
- Polyhydramnios or oligohydramnios
Provided image
A woman identified as high-risk at any contact requires a documented escalation plan: increased frequency of ANC visits, additional investigations (Doppler, NST, BPP, ophthalmology referral for hypertension), and timely referral to the appropriate level of care.
SELF-CHECK
A 38-year-old woman presents for her first ANC visit at 10 weeks. She has had two previous caesarean sections and reports that her haemoglobin at her last delivery three years ago was 9 g/dL. Which of the following risk factor categories does this represent?
A. Demographic risk only
B. Medical comorbidity only
C. Obstetric history risk and demographic risk
D. Current pregnancy finding only
Reveal Answer
Answer: C. Obstetric history risk and demographic risk
Age 38 years (>35) is a demographic risk factor. Two previous caesarean sections constitute an obstetric history risk factor (uterine scar, increased risk of placenta praevia/accreta and scar dehiscence). The previous low haemoglobin (9 g/dL in pregnancy = Hb <11 g/dL threshold) suggests a predisposition to iron deficiency anaemia — both a medical/obstetric history risk. This woman has multiple risk factors and should be classified as high-risk requiring enhanced surveillance.
Applied Practice: Counselling, Danger Signs and Referral Decisions
The clinical encounter does not end with risk stratification — it transitions into action. For the low-risk pregnant woman, action means structured health promotion counselling covering nutrition, supplementation adherence, physical activity and rest, perineal hygiene, and most critically, danger sign education. For the high-risk woman, action means a documented management plan communicated to the woman, her family and the receiving facility. In both cases, the quality of this translational step — from assessment to action — is what determines whether the objectives of ANC are actually achieved at the individual level. A perfect risk assessment that is not acted upon has no clinical value; a well-counselled low-risk woman who recognises a danger sign and seeks care promptly converts a potential maternal death into a safely managed complication.
Danger signs in pregnancy are symptoms or signs that indicate a potentially life-threatening complication requiring immediate medical assessment. Every pregnant woman must be counselled on these at each ANC visit, and her family members should be included in the counselling wherever possible. The cardinal danger signs are:
- Severe headache with or without visual disturbance — suggestive of severe pre-eclampsia (CNS manifestation)
- Blurred vision, floaters, or sudden visual loss — pre-eclampsia or eclampsia imminent
- Severe epigastric or right upper quadrant pain — HELLP syndrome (haemolysis, elevated liver enzymes, low platelets)
- Sudden or heavy vaginal bleeding — antepartum haemorrhage (abruption or praevia); note that any painless bleeding after 20 weeks must raise the suspicion of placenta praevia and mandates no per-vaginal examination
- Decreased or absent fetal movements — perceived cessation of fetal movements requires urgent assessment (NST/BPP)
- Generalised oedema particularly of the face and hands — pre-eclampsia
- High fever with or without rigors — intrauterine infection, malaria, urinary tract infection
- Convulsions — eclampsia until proven otherwise; call emergency services immediately
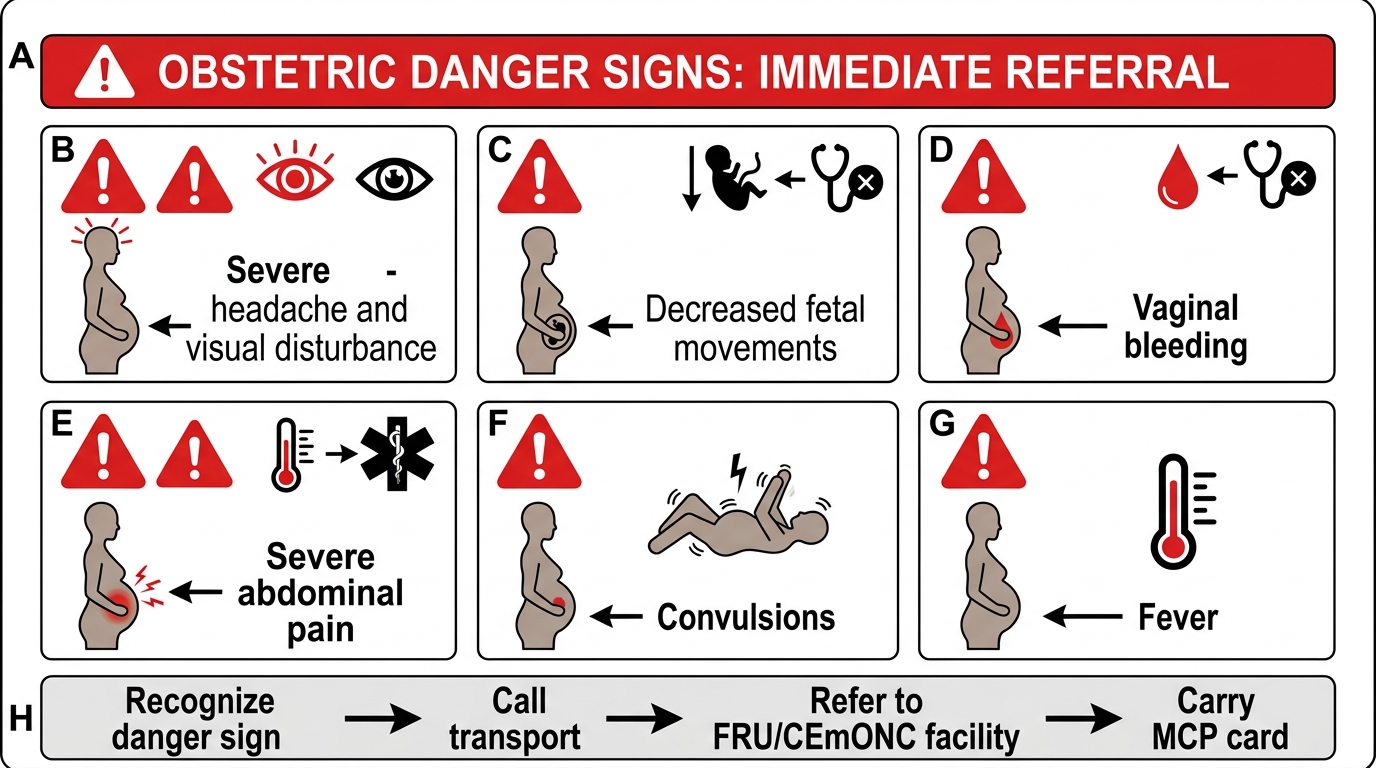
Obstetric Danger Signs Requiring Immediate Referral
Birth preparedness and complication readiness (BPCR) counselling is mandated by the MOHFW as a component of every ANC visit from the third trimester onward. The BPCR framework ensures that a pregnant woman and her family have identified: a skilled birth attendant and facility, a transport route and alternative, a blood donor of compatible group (or registered at a local blood bank), and a financial plan for emergency expenses. Evidence from India and sub-Saharan Africa demonstrates that BPCR counselling reduces the first and second 'three delays' — the delay in deciding to seek care and the delay in reaching the facility — that account for the majority of preventable maternal deaths.
Documentation in the Mother and Child Protection (MCP) card (the Indian national ANC record) is both a clinical and medicolegal requirement. Every finding, intervention, counselling topic and referral must be entered. The MCP card travels with the woman and enables continuity of care across different providers.
CLINICAL PEARL
The 'inverted pyramid' is not just a teaching diagram — it is a referral protocol. In practice, when you identify a high-risk factor at any ANC visit, ask yourself three questions: (1) Can this risk be managed at this facility level? (2) Does this woman need a higher-frequency visit schedule? (3) Does she need referral now, or at a defined gestational age? A woman with a previous caesarean section in her second trimester may be managed locally until 32 weeks, then referred to a centre with surgical capability for delivery planning. A woman who develops a BP of 150/100 mmHg at 28 weeks needs same-day specialist assessment — the pyramid escalates her immediately. Practise making this three-question decision at every ANC encounter.
Self-Assessment: ANC Objectives and Risk Screening
Consolidating the core concepts of this module requires you to move beyond passive recall toward active application. The ANC framework is not a list of facts to memorise but a clinical reasoning scaffold — the ability to explain why each objective exists, why each visit has its specific content, and why each risk factor warrants escalation, is what distinguishes a competent ANC clinician from one who merely completes a checklist. Use the structured review below to identify any gaps in your understanding before you proceed to bedside clinical sessions where these skills will be demonstrated and assessed. True competency in ANC means that when you encounter a pregnant woman in any setting — community health centre, district hospital or tertiary referral facility — you automatically and systematically apply the five ANC objectives, the visit schedule, and the risk-screening framework without prompting.
Key self-check areas — attempt each before reading reference material:
- Can you enumerate all five objectives of ANC and explain the clinical rationale for each?
- Can you describe the WHO 8-contact model and distinguish it from India's minimum 4-visit schedule?
- Can you identify at least two high-risk factors from each of the four categories (demographic, obstetric history, medical, current pregnancy)?
- Can you recite the IFA and calcium supplementation regimens correctly, including doses and duration?
- Can you list the eight cardinal danger signs and explain the underlying complication each represents?
- Can you draw the inverted pyramid and explain at which level each risk category receives care?
SELF-CHECK
A woman at 28 weeks gestation is prescribed calcium supplementation as part of routine ANC. What is the recommended dose and indication?
A. 500 mg elemental calcium once daily for general bone health
B. 1.5–2 g elemental calcium per day (from 20 weeks onward) for prevention of pre-eclampsia in low dietary calcium intake populations
C. 1 g elemental calcium per day for fetal bone development
D. 2.5 g elemental calcium per day beginning at 36 weeks for labour preparation
Reveal Answer
Answer: B. 1.5–2 g elemental calcium per day (from 20 weeks onward) for prevention of pre-eclampsia in low dietary calcium intake populations
Per WHO 2016 ANC recommendations, calcium supplementation at 1.5–2 g elemental calcium per day (given as 500 mg three times daily) is recommended from 20 weeks of gestation in areas where dietary calcium intake is low (a common scenario in India). The primary indication is reduction of the risk of pre-eclampsia, not general bone health or fetal bone development. The 36-week timing in option D is incorrect; supplementation begins at 20 weeks.