Page 13 of 30
OG8.5 | Pelvic Assessment and CPD Evaluation — SDL Guide (Part 2)
Interpreting Pelvimetry Findings and Diagnosing CPD
Interpreting the pelvimetry findings requires converting the measured diagonal conjugate to the clinically important obstetric conjugate and then synthesising all findings to reach a classification of pelvic adequacy relative to the expected fetal presenting part size. This interpretation step is where the procedural skill of pelvimetry is translated into a clinical decision — and it is where examination candidates most commonly make errors, either by forgetting to subtract 1.5–2 cm when converting DC to OC, or by interpreting individual measurements in isolation without integrating the pelvic type (android pelvis with borderline measurements is more concerning than gynaecoid pelvis with the same measurements). The classification framework below provides a structured approach: it is not a set of rigid cut-offs but a guide that must be combined with gestational age, estimated fetal weight, engagement status, and the woman's obstetric history before a management plan is reached.
Provided image
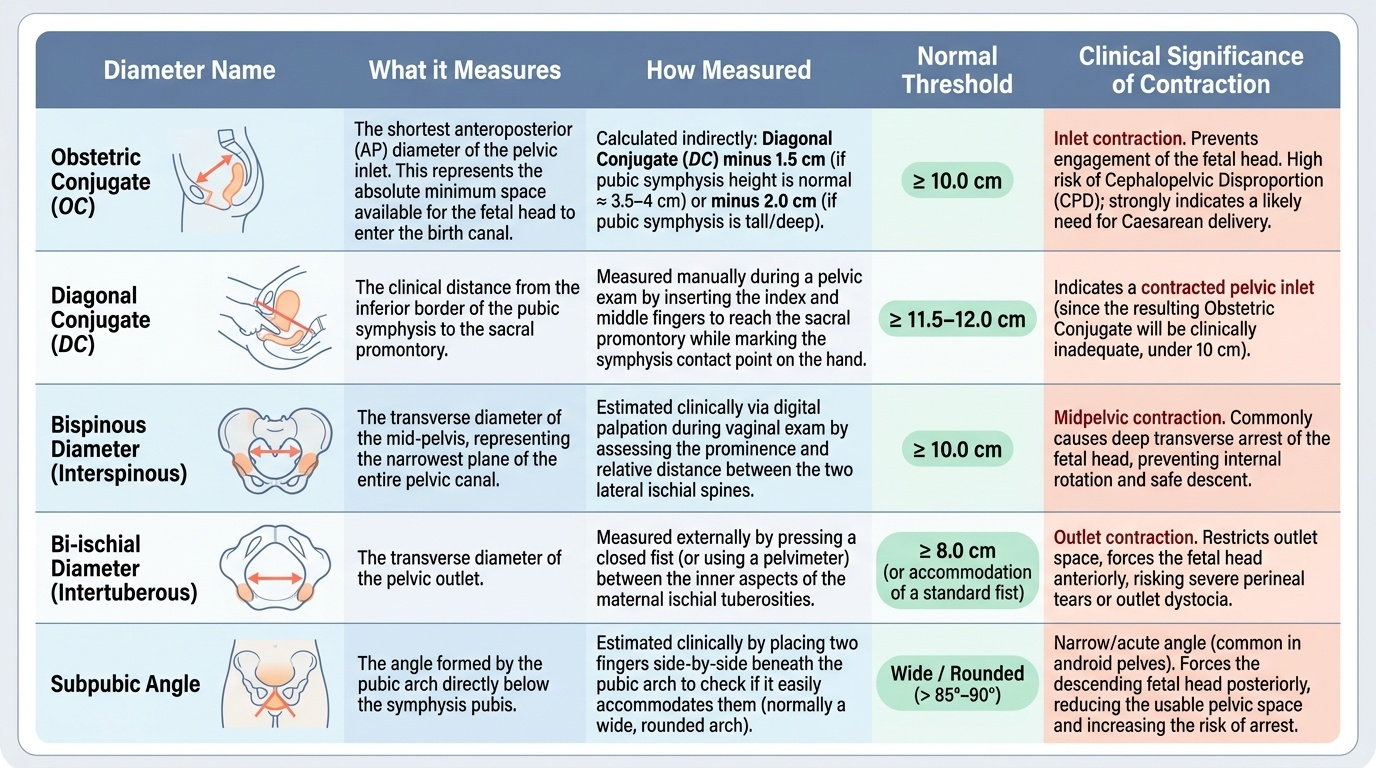
Converting diagonal conjugate to obstetric conjugate:
The obstetric conjugate (OC) is the shortest anteroposterior diameter of the pelvic inlet — the minimum space available for the fetal head at the inlet. It cannot be measured directly because the sacral promontory is not accessible to a finger from the anterior direction. The clinical approximation is:
- Obstetric conjugate = Diagonal conjugate − 1.5 cm (if pubic symphysis height is normal ≈ 3.5–4 cm)
- Obstetric conjugate = Diagonal conjugate − 2 cm (if pubic symphysis is tall/deep, more common in women with android-type pelvis)
- In practice, subtracting 1.5–2 cm is used and interpreted in range: a DC of 12 cm → OC of 10–10.5 cm (borderline/normal); a DC of 11 cm → OC of 9–9.5 cm (contracted inlet)
Classification of CPD:
- No CPD (adequate pelvis): OC ≥10 cm, bispinous ≥10 cm, bi-ischial ≥8 cm, normal subpubic angle — vaginal delivery is anticipated to be possible with appropriate fetal position
- Borderline CPD: measurements within 1 cm of thresholds, or one borderline + normal others — trial of labour with close monitoring is appropriate
- Suspected CPD: OC 8–10 cm, or bispinous <10 cm with prominent ischial spines + android pelvis characteristics — consider trial of labour with senior oversight or elective LSCS depending on estimated fetal weight and obstetric history
- Absolute CPD: OC <8 cm — vaginal delivery of a term fetus is not possible; elective caesarean section is indicated
Additional clinical factors in CPD assessment:
- Estimated fetal weight (EFW): a smaller fetus (EFW 2.8 kg) may achieve vaginal delivery through a pelvis that would obstruct with a macrosomic fetus (EFW 4.2 kg)
- Moulding and asynclitism: the fetal skull bones can overlap at the sutures (moulding) by up to 1 cm, effectively reducing the presenting diameter — this is a physiological compensatory mechanism
- Engagement: if the fetal head is engaged at term in a primigravida (head has descended below the pelvic brim), the inlet measurements are functionally adequate
- Pelvic type: android pelvis is the most unfavourable; gynaecoid the most favourable, even with borderline measurements
SELF-CHECK
A primigravida at term has a pelvic assessment that reveals: diagonal conjugate 11.5 cm, markedly prominent ischial spines, a closed fist does not fit easily between the ischial tuberosities (estimated bi-ischial diameter 7 cm), and a narrow subpubic angle. Which level(s) of the pelvis is/are contracted?
A. Inlet only
B. Outlet and midplane only
C. Midplane and outlet — the inlet is borderline to normal
D. No contraction — all measurements are within the normal range
Reveal Answer
Answer: C. Midplane and outlet — the inlet is borderline to normal
Diagonal conjugate 11.5 cm → obstetric conjugate approximately 9.5–10 cm — this is borderline/low normal for the inlet (threshold 10 cm). However, markedly prominent ischial spines indicate midplane contraction (bispinous diameter <10 cm), and a bi-ischial diameter of 7 cm (threshold ≥8 cm) combined with a narrow subpubic angle indicates outlet contraction. This pelvis has a normal to borderline inlet but contracted midplane and outlet — the android pelvis pattern. This is clinically important because even if the fetal head negotiates the inlet, it may arrest at the midplane or outlet, making a delayed diagnosis of CPD in second-stage labour a significant risk.
Applied Decision-Making: Managing Suspected or Confirmed CPD
The management of CPD requires integrating pelvimetry findings with multiple clinical variables to arrive at the safest delivery plan for mother and fetus. No single pelvimetric measurement determines the delivery mode in isolation — the decision emerges from a combination of pelvic dimensions, estimated fetal weight, gestational age, parity, fetal presentation and position, and the strength and regularity of uterine contractions. This reflects the 'three P's' framework: the passage (pelvis) is assessed by pelvimetry, but the passenger (fetus) and the powers (contractions) must also be adequate for vaginal delivery.
Absolute CPD (OC <8 cm):
Elective lower segment caesarean section (LSCS) is indicated before the onset of labour. The risk of maternal and fetal harm from obstructed labour far outweighs the risks of planned caesarean delivery. The decision should be made by 36–38 weeks gestation in conjunction with a senior obstetrician.
Borderline or suspected CPD (OC 8–10 cm):
Trial of labour is the standard management — allowing the woman to enter spontaneous labour and monitoring progress closely. The trial of labour proceeds with the following conditions:
- Continuous CTG monitoring from the active phase
- Senior obstetrician review every 2 hours in active labour
- Expectation of normal progress (1 cm/hour after 4 cm in active phase)
- Threshold for abandoning the trial: arrested labour at any phase despite adequate uterine contractions; evidence of fetal compromise; developing caput succedaneum and moulding without descent
- Emergency LSCS if the trial of labour fails (documented as 'failed trial of labour' or 'failure to progress secondary to suspected CPD')
The trial of labour is contra-indicated in:
- Absolute CPD (OC <8 cm)
- Previous uterine rupture
- Classical (upper segment) caesarean scar (vertical uterine scar)
- Fetal malpresentation that is unfavourable for vaginal delivery (e.g., brow presentation, face presentation with mentoposterior)
Role of imaging in borderline CPD:
CT pelvimetry provides more precise measurements than clinical pelvimetry and is used in specialist centres for truly borderline cases. However, most obstetric decisions do not require CT — clinical judgement combined with ultrasound EFW is sufficient. X-ray pelvimetry is no longer recommended due to fetal radiation exposure.
CLINICAL PEARL
The most practical screening tool for pelvic adequacy before detailed pelvimetry is the woman's own height and obstetric history. Height <150 cm is associated with an increased risk of contracted pelvis and should trigger formal pelvimetry at 36 weeks. In a primigravida, engagement of the fetal head at term (confirmed by Leopold's third grip — head not freely ballotable) is a useful functional indicator that the inlet is adequate — if the head has entered the pelvis, the inlet has accepted it. However, non-engagement in a primigravida does not confirm CPD — it should prompt pelvimetry, not automatic caesarean section. The clinical pearl is: engagement = inlet probably adequate; non-engagement = investigate further.
Self-Assessment: Pelvic Assessment and CPD
Pelvimetry is a skill assessed in your DOAP station — you will be asked to demonstrate the technique on an obstetric pelvic model, interpret the measurements, and describe your management plan. The questions below consolidate both the technical and clinical reasoning elements of this competency, targeting the level of performance expected in an SH (Should Demonstrate Hands-on) competency assessment. An SH assessment means you must not only describe the technique verbally but also perform it correctly on the model — your hand position for the diagonal conjugate, the way you identify the sacral promontory, how you mark the measuring point on your hand, and how you state the result and calculate the obstetric conjugate. Reviewers in DOAP stations particularly watch for: correct patient/model positioning, systematic coverage of all three pelvic levels (inlet, midplane, outlet), and the ability to integrate findings into a management recommendation that is appropriate for the obstetric context. The questions below consolidate both the technical and clinical reasoning elements of this competency. Attempt each question as if you are at the DOAP station: describe the technique as you would perform it, state the measurements as you would record them, and give the management as you would advise a patient.
Self-check questions for structured review:
- Describe the step-by-step technique of measuring the diagonal conjugate. What structure do you need to reach with your examining finger, and how is the measurement taken from the hand?
- A diagonal conjugate of 10.5 cm is measured. What is the estimated obstetric conjugate? How would you classify this pelvis and what delivery plan would you recommend?
- Name the four Caldwell-Moloy pelvic types. Which is the most favourable for vaginal delivery, and which features make the android pelvis the least favourable?
- At what point in labour, and with what specific findings, would you decide that a trial of labour for borderline CPD should be abandoned?
- State the normal threshold for each of the following: (1) obstetric conjugate, (2) diagonal conjugate, (3) bispinous diameter, (4) bi-ischial diameter.
SELF-CHECK
A 22-year-old primigravida at 38 weeks has a height of 148 cm and a non-engaged fetal head (freely mobile on Leopold's third grip). Her pelvic assessment shows: diagonal conjugate 13 cm, ischial spines slightly prominent, bi-ischial diameter 8.5 cm, and normal subpubic angle. What is the most appropriate management?
A. Immediate elective caesarean section as her short stature and non-engaged head confirm CPD
B. Trial of labour with close monitoring — the pelvimetry findings are within normal limits despite the clinical risk factors
C. Induce labour immediately using oxytocin to test pelvic adequacy
D. Order an X-ray pelvimetry before making any management decision
Reveal Answer
Answer: B. Trial of labour with close monitoring — the pelvimetry findings are within normal limits despite the clinical risk factors
Despite the clinical risk factors (height 148 cm, non-engaged head), the pelvimetry findings are within normal limits: diagonal conjugate 13 cm → obstetric conjugate approximately 11–11.5 cm (normal ≥10 cm); slightly prominent ischial spines (borderline, not markedly prominent); bi-ischial diameter 8.5 cm (normal ≥8 cm); normal subpubic angle. This is a borderline-normal pelvis — the appropriate management is trial of labour with close monitoring, NOT immediate caesarean section. Short stature and non-engagement are risk factors that prompted pelvimetry, not diagnoses of CPD. X-ray pelvimetry (D) is no longer recommended. Inducing with oxytocin (C) without a delivery plan is not the same as a supervised trial of labour with defined abort criteria.