Page 22 of 30
OG8.10 | Post-Caesarean Pregnancy — SDL Guide
Learning Objectives
- Describe the clinical significance of a uterine scar in subsequent pregnancies and the epidemiological context of rising caesarean rates
- Explain the pathophysiology of uterine scar healing, the structural differences between lower-segment and classical CS incisions, and the mechanism of uterine rupture
- Evaluate a post-caesarean pregnancy: take a directed history, assess scar type and inter-delivery interval, identify TOLAC eligibility and contraindications
- Counsel a woman on TOLAC vs ERCS using evidence-based success predictors, rupture risk figures, and shared decision-making principles
- Describe intrapartum management of TOLAC including continuous CTG monitoring, recognition of impending uterine rupture, and emergency response
- Outline the indications, timing, and complications of Elective Repeat Caesarean Section (ERCS) including placenta accreta spectrum risk in multiple repeat CS
INSTRUCTIONS
India's caesarean section rate has risen sharply — in many urban centres it exceeds 40% of all deliveries. This means a growing cohort of women presenting for their next pregnancy with a uterine scar. The choice between attempting vaginal birth (TOLAC/VBAC) and planning an elective repeat caesarean (ERCS) is one of the most consequential counselling decisions in obstetrics: it balances the risks of uterine rupture against the short- and long-term morbidity of repeat surgery, and must account for the woman's parity, scar type, facility capabilities, and reproductive goals. This module equips you to assess, counsel, and manage post-caesarean pregnancies safely and systematically.
References
- Dutta DC. Textbook of Obstetrics, 9th ed. New Central Book Agency, 2018. Ch 35 (Caesarean Section) (textbook)
- Williams Obstetrics, 25th ed. McGraw-Hill, 2018. Ch 31 (Prior Cesarean Delivery) (textbook)
- RCOG Green-top Guideline No. 45: Birth After Previous Caesarean Birth, October 2015 (guideline)
- ACOG Practice Bulletin No. 205: Vaginal Birth After Cesarean Delivery, February 2019 (guideline)
- FOGSI Good Clinical Practice Recommendations: Caesarean Section, 2018 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Mrs Kavitha is 27 years old, G2P1, at 36 weeks gestation. She delivered her first baby by emergency caesarean section 3 years ago for fetal distress after 8 hours of active labour. That baby weighed 3.1 kg and is now healthy. Today at antenatal clinic she asks you: 'Doctor, can I have a normal delivery this time? My neighbour had a normal delivery after CS but my mother says it is too dangerous.' Her ultrasound shows a cephalic singleton, the lower uterine segment measures 3.2 mm on ultrasound, and her pelvis was assessed as adequate at the previous ANC visit. How do you counsel her — and what are the clinical factors that will shape your answer?
WHY THIS MATTERS
Post-caesarean pregnancy management is not a niche subspecialty skill — it is a routine clinical scenario you will encounter in every obstetric posting as India's CS rate continues to climb. Understanding TOLAC, VBAC, and ERCS has direct patient-safety consequences: offering TOLAC to an ineligible woman risks catastrophic uterine rupture; denying it to an eligible woman increases surgical morbidity and future placenta accreta risk. The NMC competency OG8.10 requires you to describe and discuss cases of post-caesarean pregnancy and their management — this module builds exactly that clinical reasoning framework.
RECALL
Before proceeding, bring to mind what you already know: (1) The anatomy of the lower uterine segment — how it differs from the upper segment in muscle thickness, vascularity, and contractility. (2) The layers of the uterine wall — endometrium/decidua, myometrium, serosa — and how surgical incision through all three heals. (3) The standard lower-segment caesarean section (LSCS) technique — the Pfannenstiel or midline abdominal incision, the low-transverse uterine incision, and why this site was chosen over the upper-segment classical approach. (4) Factors that make a pelvis adequate for vaginal delivery — conjugates, diameters, pelvic types. These form the anatomical and physiological substrate for everything in this module.
Clinical Presentation and Context of Post-Caesarean Pregnancy
A post-caesarean pregnancy is any pregnancy occurring in a woman who has had one or more previous caesarean deliveries. The defining clinical question — can this woman deliver vaginally, and if so safely? — arises at the first antenatal visit and must be resolved with counselling that is both evidence-based and personalised. To understand why this decision matters, we must first appreciate the epidemiological backdrop.
India's national caesarean rate was approximately 21.5% at the time of the last National Family Health Survey (NFHS-5, 2019–2021), but rates in private hospitals and urban centres routinely exceed 40–50%. Globally, the WHO estimates more than 21% of all births are now by caesarean. This exponential rise means that in any busy obstetric unit, a substantial proportion of women presenting for antenatal care — sometimes 30–40% of multiparous women — will have at least one previous CS scar. The consequences compound with parity: a woman who has had two caesareans faces a different risk profile from one who has had one, and a woman who has had three or more is at high risk for placenta accreta spectrum (PAS) — a potentially life-threatening complication of adherent placentation.
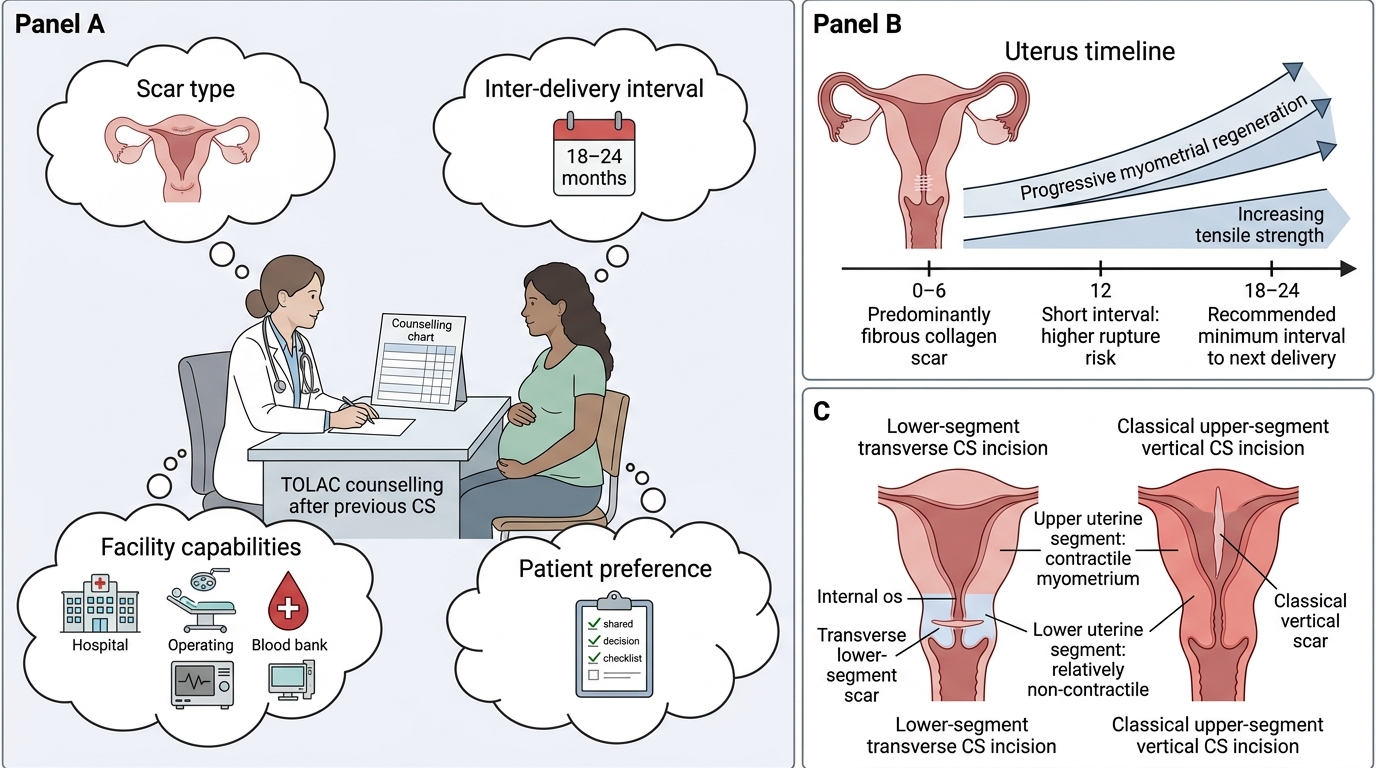
The fundamental clinical scenario has three components: (1) the scar itself — what type of uterine incision was made, how long ago, and whether it healed uneventfully; (2) the current pregnancy — presentation, gestational age, estimated fetal weight, placental location, and obstetric pelvis; and (3) the institutional context — whether 24-hour emergency caesarean, anaesthetic, and neonatal intensive care services are available, because TOLAC is only safe where immediate surgical backup exists.
At the first antenatal visit, directed history should establish: number and type of previous caesarean incisions, indication(s) for previous CS (was the indication non-recurrent, such as fetal distress, or recurrent, such as cephalopelvic disproportion?), any previous vaginal deliveries (before or after the CS), inter-delivery interval, and any peri-operative complications. The operative notes of the previous CS, if available, are invaluable — they confirm scar type and any intraoperative findings that may affect subsequent labour.
TOLAC Counselling After Previous Caesarean Section
The inter-delivery interval deserves particular emphasis. The minimum recommended time from previous CS to the next delivery is 18–24 months (some guidelines say ≥18 months from delivery, others ≥24 months from delivery — state the source when counselling). The rationale is biological: uterine scar tissue is predominantly fibrous collagen for the first 6 months after surgery; adequate tensile strength requires sufficient myometrial regeneration, which takes at least 18 months. A short interpregnancy interval — especially less than 12 months — is independently associated with increased risk of uterine rupture in subsequent labour.
Pathophysiology — The Uterine Scar and Its Consequences
The safety of TOLAC depends fundamentally on the biology and geometry of the uterine scar. Not all caesarean scars are equal — the type of incision determines the risk of rupture in a way that is among the most dramatic risk gradients in obstetrics.
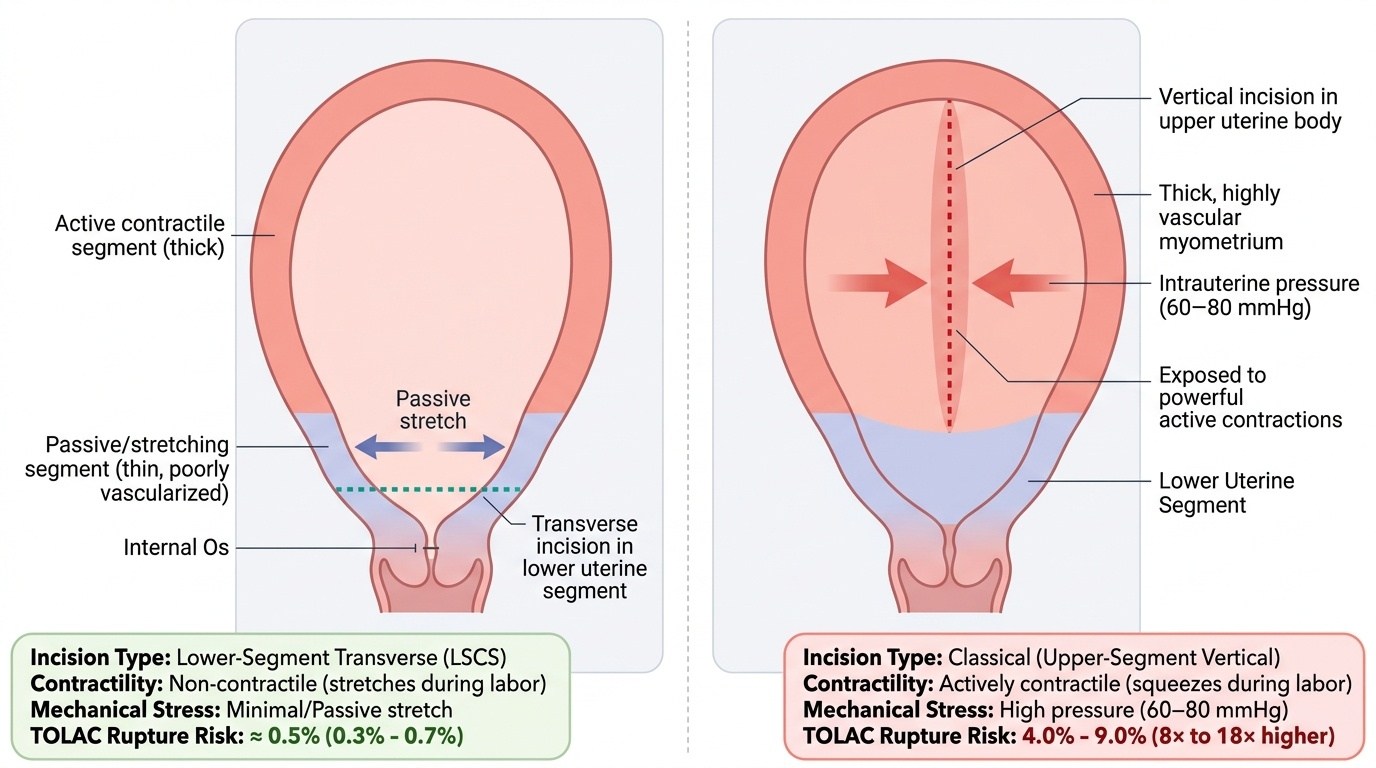
Scar healing biology: When the uterine myometrium is incised at caesarean section, it heals by fibrosis. In an uncomplicated repair, collagen-rich scar tissue initially fills the defect over 6–8 weeks, but over 12–24 months some myometrial regeneration may occur, restoring partial tensile strength. However, the scar site is always structurally weaker than intact myometrium — it lacks the elasticity and contractile reserve of normal muscle. During a subsequent labour, uterine contractions generate intrauterine pressures of up to 60–80 mmHg; the scar must withstand this repeated mechanical stress throughout active labour.
Provided image
Lower-segment transverse (LSCS) scar — the modern standard. The lower uterine segment is thin, poorly vascularised, and relatively non-contractile. A transverse incision here heals well because it is not subjected to the full force of upper-segment contractions during labour. The lower segment stretches (effaces) rather than contracts, so the scar is under less mechanical stress. The result is a uterine rupture risk of approximately 0.5% (0.3–0.7%) with TOLAC — a risk low enough that TOLAC is considered a reasonable and safe option in eligible women.
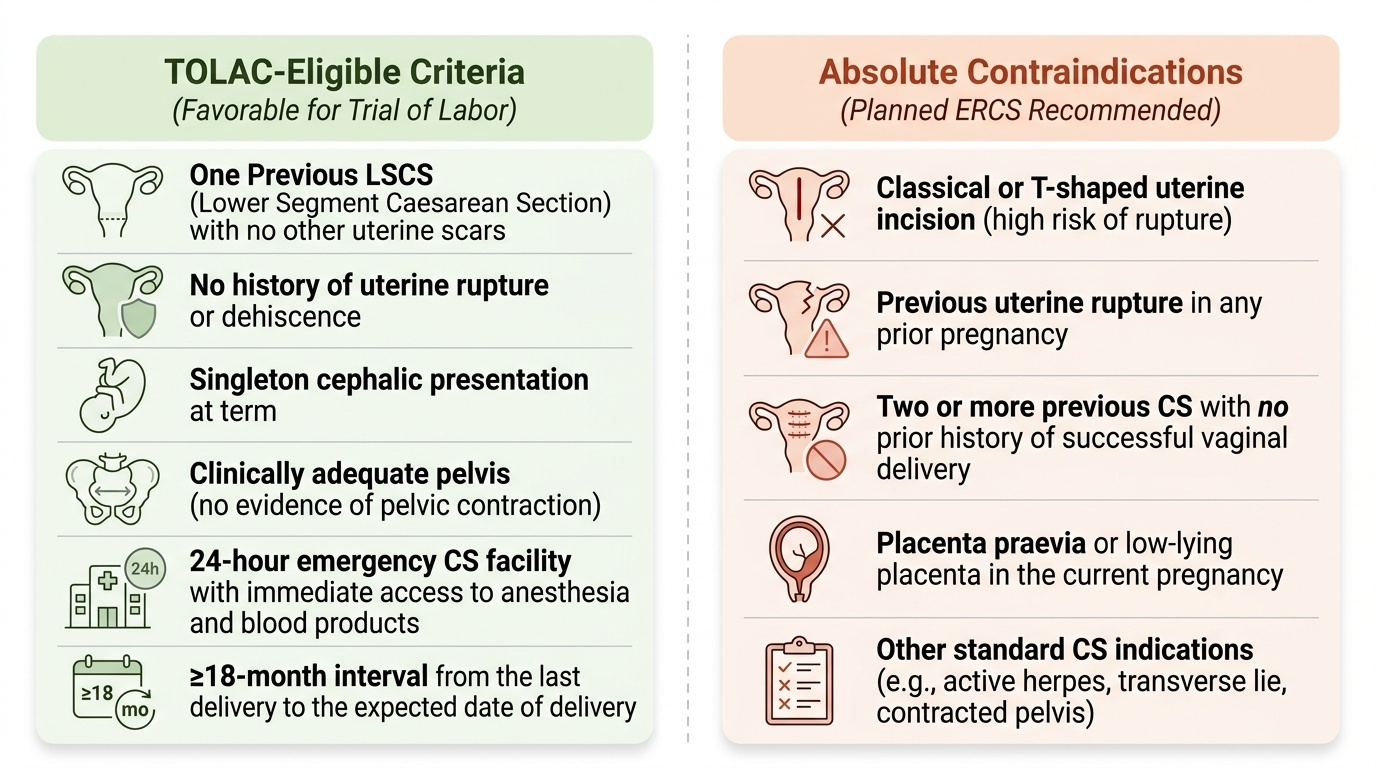
Classical (upper-segment vertical) scar — now reserved for specific indications such as transverse lie with ruptured membranes, extreme prematurity with an undeveloped lower segment, or anterior placenta praevia. The upper uterine body is thick, highly vascular, and actively contractile. A vertical incision through this segment creates a scar that is exposed to powerful contractions with every uterine contraction in labour. The structural consequence is dramatic: the rupture risk is 4–9% with TOLAC — 8 to 18 times higher than an LSCS scar. This is why a classical uterine scar is an absolute contraindication to TOLAC.
Inverted-T and J-incision scars — created when a transverse lower-segment incision is extended upward (T) or laterally (J) to deliver a difficult baby — carry an intermediate risk of approximately 4–9%, similar to classical, and are also contraindications to TOLAC. Low-vertical (De Lee) incisions, made in the lower segment but vertically, carry somewhat higher risk than transverse lower-segment incisions and are generally considered contraindications as well.
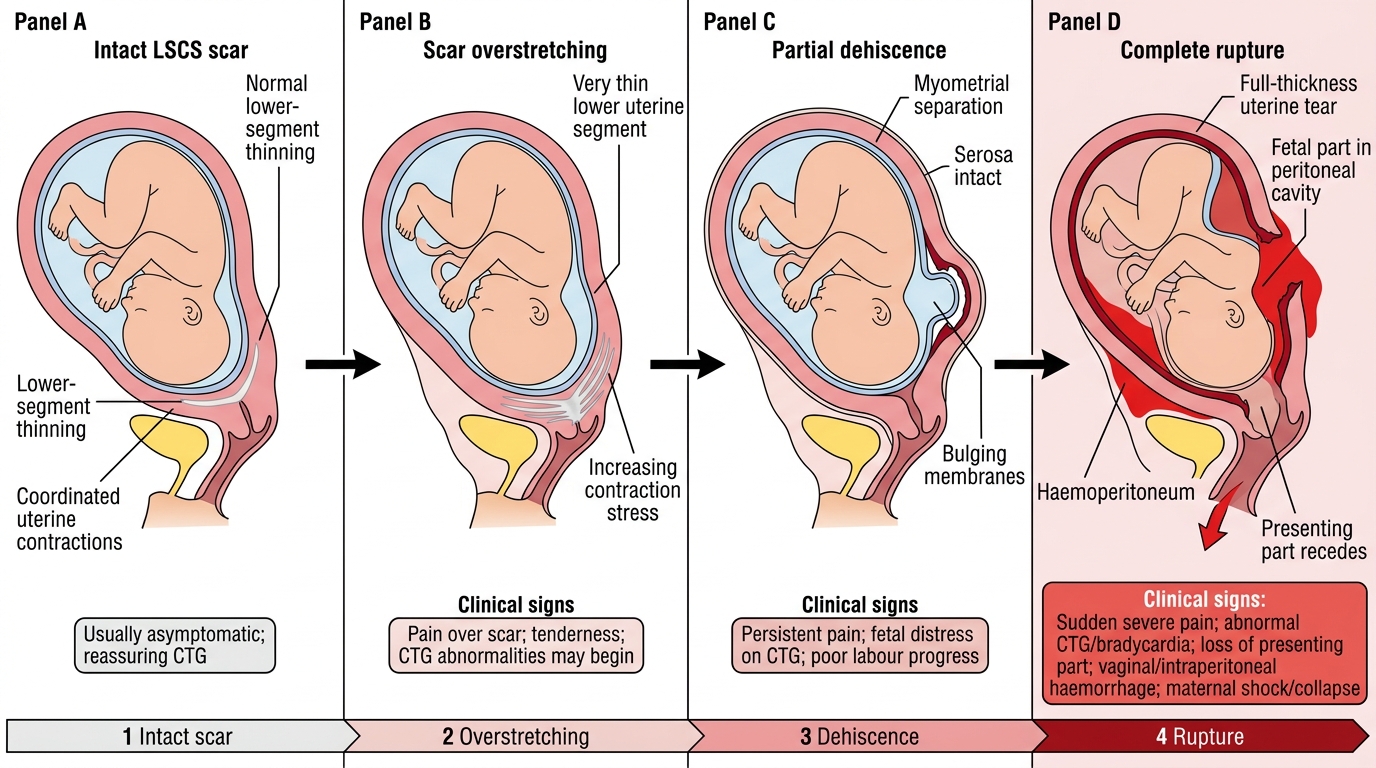
Uterine rupture vs dehiscence: These are distinct entities with very different clinical significance. Uterine rupture is a complete disruption of all layers of the uterine wall — myometrium, peritoneum (serosa), and decidua — allowing fetal parts or the umbilical cord to extrude into the peritoneal cavity. It is a surgical emergency with a fetal mortality of 50–75% and significant maternal mortality from haemorrhage. Uterine dehiscence is an incomplete separation of the scar, typically confined to the myometrium with the visceral peritoneum (serosa) intact; the fetus remains within the uterus. Dehiscence may be asymptomatic or present with mild scar tenderness, and is often discovered incidentally at repeat CS. Clinically distinguishing the two intrapartum requires a high index of suspicion.
Pathophysiology of Uterine Scar Rupture During Labour
Diagnosis and Assessment — Evaluating the Post-CS Pregnancy
Systematic assessment of the post-caesarean pregnancy begins at the first antenatal visit and integrates clinical history, physical examination, and targeted investigations to arrive at a delivery plan before labour onset. Leaving this decision to the labour ward is a preventable safety failure.
History (directed): The most important historical elements are: (1) Number of previous CS — each additional caesarean incrementally increases the risk of scar complications, adhesions, and placenta accreta spectrum. Two or more previous CS significantly narrows TOLAC eligibility. (2) Type of uterine incision — elicit whether lower-segment transverse, classical, or other; operative notes are the most reliable source, but the patient should be told at the time of CS and the type documented in the discharge summary. (3) Indication for previous CS — a non-recurrent indication (e.g., fetal distress, cord prolapse, malpresentation that has now self-corrected) is favourable; a recurrent indication (e.g., documented cephalopelvic disproportion, bony pelvis abnormality, or failure to progress despite oxytocin augmentation) strongly favours ERCS. (4) Inter-delivery interval — time from last CS to the expected date of delivery in this pregnancy; minimum 18 months is generally recommended. (5) Any previous vaginal delivery — a prior VBAC or vaginal delivery before the CS is the single strongest predictor of VBAC success.
Physical examination: Abdominal scar assessment (Pfannenstiel vs midline); uterine size, presentation, and engagement; clinical pelvimetry. A contracted pelvis or clinical evidence of absolute cephalopelvic disproportion is a contraindication to TOLAC regardless of scar type.
Investigations: The key investigation specific to scar assessment is lower uterine segment (LUS) thickness by ultrasound. Measured transabdominally or transvaginally in the third trimester, a full-thickness LUS of:
- ≥3.5 mm — generally reassuring; scar likely intact and of reasonable thickness
- 2.0–3.4 mm — borderline; warrants careful clinical assessment and caution
- <2.0 mm — thin scar; associated with increased risk of rupture; many clinicians advise ERCS
Important caveat: LUS thickness measurement has significant operator variability and is not a standalone criterion for ERCS — it is one element of the overall risk assessment, not a binary decision tool.
Provided image
Institutional prerequisites for TOLAC: TOLAC is only safe where 24-hour emergency caesarean capability — including on-site anaesthetic and theatre teams — is immediately available. Facilities without this capability must refer post-caesarean women for confinement to an appropriately equipped centre. This is not optional — the time window from rupture to delivery (and haemostasis) for fetal salvage is typically 10–37 minutes.
SELF-CHECK
A woman with a previous classical uterine scar requests TOLAC. The most appropriate response is:
A. Agree to TOLAC if her Bishop score is ≥8 at term
B. Agree to TOLAC only if her inter-delivery interval is ≥24 months
C. Decline TOLAC and counsel for elective repeat caesarean section
D. Offer TOLAC with continuous CTG monitoring and standby theatre
Reveal Answer
Answer: C. Decline TOLAC and counsel for elective repeat caesarean section
A classical (upper-segment vertical) uterine scar is an absolute contraindication to TOLAC because the rupture risk is 4–9% — approximately 8–18 times higher than a lower-segment transverse scar. No cervical score, inter-delivery interval, or monitoring arrangement makes TOLAC safe with a classical scar. ERCS is mandatory.