Page 19 of 30
OG8.9 | Stillbirth Evaluation — SDL Guide
Learning Objectives
- Define stillbirth using the India/NMC definition (≥28 weeks or ≥1000 g) and distinguish it from abortion and neonatal death (OG8.9)
- Describe the clinical presentation of stillbirth — fresh vs macerated, antepartum vs intrapartum
- Enumerate and classify causes of stillbirth using the ReCoDe framework
- Outline the investigation protocol for a stillbirth and describe the management plan including induction of labour and bereavement care
INSTRUCTIONS
Stillbirth is a profoundly significant event for families and a sensitive indicator of antenatal and intrapartum care quality. India's stillbirth rate of approximately 13.9 per 1,000 total births (SRS 2020) remains one of the highest in Asia, with a large fraction preventable through better ANC surveillance and intrapartum monitoring. As a final-year student you must understand how to define, classify, investigate, and manage a stillbirth — and how to support a grieving family with sensitivity and clinical accuracy.
References
- DC Dutta's Textbook of Obstetrics, 10th ed., Ch. 26 (Intrauterine Fetal Death) (textbook)
- Williams Obstetrics, 26th ed., Ch. 35 (Stillbirth) (textbook)
- FOGSI Good Clinical Practice Recommendations — Stillbirth (2018) (guideline)
- Lancet Stillbirth Series 2016 — Global, regional, and national estimates of stillbirth rates in 2015 (journal)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 28-year-old multigravida at 36 weeks of gestation presents to the labour room stating she has not felt her baby move for two days. On auscultation with a Pinard stethoscope, no fetal heart sounds are heard. Doppler ultrasound confirms absence of fetal cardiac activity. Her husband is outside. The fetus appears macerated on ultrasound. How do you confirm the diagnosis, inform the family, initiate investigation, and plan management?
WHY THIS MATTERS
Stillbirth is one of the most emotionally devastating outcomes in obstetric practice, and simultaneously one of the most preventable in a significant proportion of cases. India contributes a disproportionately large share of the global stillbirth burden — the Sample Registration System (2020) estimates a national stillbirth rate of approximately 13.9 per 1,000 total births, which despite improvement over two decades, remains substantially higher than the global target of ≤12 per 1,000 by 2030 (Every Newborn Action Plan). A key distinction: intrapartum stillbirths (fresh stillbirths occurring during labour) are largely preventable with adequate skilled birth attendance and fetal monitoring, while antepartum stillbirths reflect failures in antenatal surveillance for placental insufficiency, maternal disease, and fetal anomaly. Understanding causes, investigation pathways, and management is central to final-year MBBS clinical examinations (written, viva, and practical) and to your practice as an intern on a labour ward.
RECALL
Before proceeding, recall: (1) Definitions — term = 37–42 weeks; preterm <37 weeks; abortion = fetal loss before 20 weeks or <500 g. Stillbirth occupies the range between abortion and neonatal death. (2) From og3-surveillance: fetal kick count monitoring and Doppler velocimetry are the primary tools for antepartum fetal surveillance — reduced fetal movements are the commonest presenting symptom of a stillbirth. (3) From OG pharmacology: DIC (disseminated intravascular coagulation) is a serious complication of prolonged retention of a dead fetus in utero — coagulation screening is mandatory before induction. (4) From OG2/OG3: placental structure and its role in oxygen and nutrient transfer — placental insufficiency is a leading pathway to antepartum stillbirth.
Clinical Presentation of Stillbirth
Stillbirth most commonly presents with the mother reporting absent or markedly reduced fetal movements — a symptom that must always be taken seriously and investigated urgently. Other presenting scenarios include: a routine ANC visit at which fetal heart sounds cannot be detected; onset of labour with no fetal heart heard on admission; or incidental detection on antenatal ultrasound. The presenting complaint of absent fetal movements is present in the majority of antepartum stillbirths, which is why systematic fetal kick count monitoring and a clear protocol for responding to maternal concern about reduced movements are cornerstones of antenatal care.
Definition — India/NMC context: A stillbirth is defined as the birth of a baby at ≥28 weeks of gestation OR ≥1000 g birth weight with no signs of life (no breathing, no heartbeat, no definitive movement). This threshold distinguishes stillbirth from abortion (loss <20 weeks or <500 g per Indian context) and from neonatal death (death after live birth). The WHO global definition for international comparison also uses ≥28 weeks or ≥1000 g. Note: the WHO extended research definition uses ≥22 weeks or ≥500 g — this is NOT the definition used for official birth registration in India.
Clinical classification by maceration state:
- Fresh stillbirth: No maceration — skin intact, colour normal or slightly discoloured. Suggests death occurred recently (within 12–24 hours) or during labour (intrapartum stillbirth). The body structure is preserved. Fresh stillbirths are a particularly important quality indicator because the majority are preventable with intrapartum monitoring.
- Macerated stillbirth: Maceration present — death occurred ≥12–24 hours before delivery, typically antepartum. Features of maceration include: skin discolouration (brownish-green), skin slippage (epidermis peeling), overlapping skull bones (Spalding's sign on X-ray — due to brain liquefaction and skull collapse), softening of the fetus, foul odour if prolonged. Maceration progresses over days and provides a rough guide to the time interval since death.
Confirmation of stillbirth: Bedside Pinard stethoscope auscultation and handheld Doppler are the first steps. Confirmation MUST be by real-time ultrasound showing absence of fetal cardiac activity — this is the definitive standard, and is especially important before communicating the diagnosis to the family. A single brief scan by a trained operator is sufficient; the scan also assesses placenta, liquor, and fetal position. Never diagnose stillbirth on auscultation alone in a clinical or medico-legal setting.
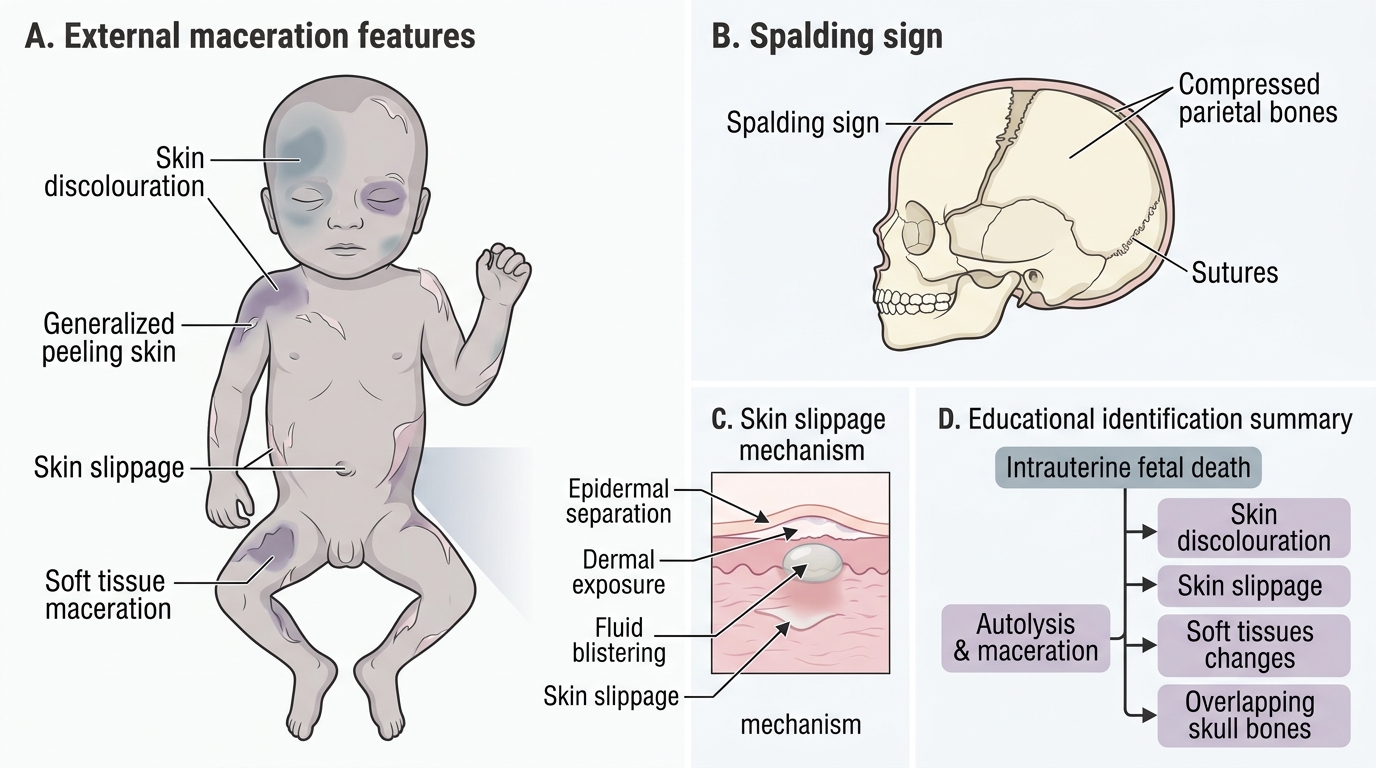
Maceration Features in Stillbirth
Pathophysiology and Basis — Mechanisms and Causes
Understanding the mechanisms and causes of stillbirth is essential for two reasons: it informs the investigation that must follow every stillbirth, and it identifies the preventable fraction that can be reduced through better antenatal and intrapartum care. In approximately 25–30% of cases, no definitive cause is found even after full investigation — these are classified as unexplained stillbirths. However, systematic evaluation using a structured framework nearly doubles the rate of identified causes compared to clinical impression alone.
Mechanisms of fetal death: The final common pathway in the vast majority of stillbirths is fetal hypoxia — insufficient oxygen delivery to the fetal brain and vital organs. The route to hypoxia varies by cause: acute hypoxia (abruption, cord prolapse, sinus bradycardia during obstructed labour) causes rapid death in hours; chronic hypoxia from placental insufficiency causes progressive growth restriction and eventually stillbirth over days to weeks. A minority die from non-hypoxic mechanisms: overwhelming fetal infection, severe structural anomaly incompatible with life, or fetomaternal haemorrhage leading to severe fetal anaemia.
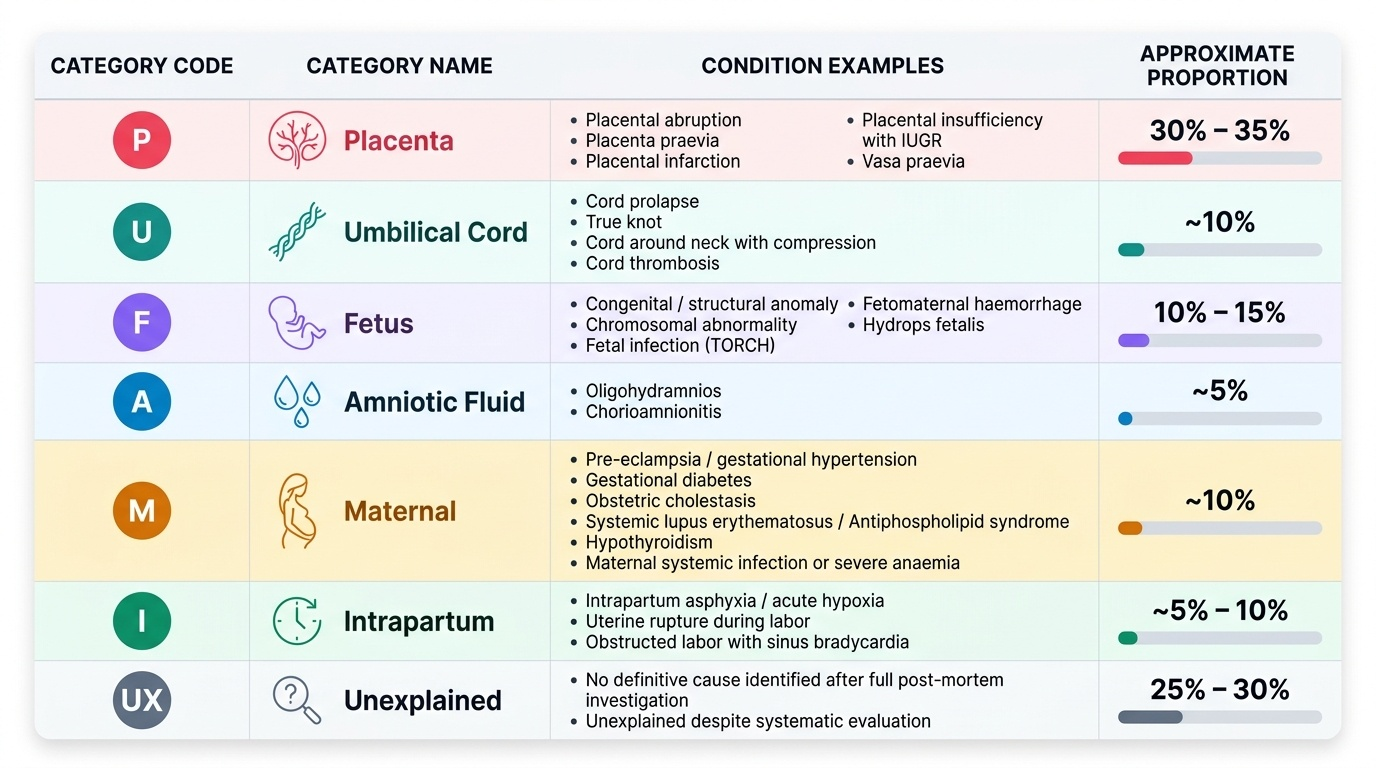
The ReCoDe (Relevant Condition at Death) classification system is the most widely used framework for classifying stillbirth causes. It categorises the most relevant condition present at the time of death rather than the immediate mechanism of death — this makes it more useful for prevention than pathology-based systems. ReCoDe categories:
- Group P (Placenta): Placental abruption, placenta praevia, placental infarction, vasa praevia, placental insufficiency with IUGR — the most common identified cause category in high-income countries and a major contributor in India.
- Group U (Umbilical cord): Cord prolapse, true knot, cord around neck with compression, cord thrombosis — responsible for approximately 10% of stillbirths.
- Group F (Fetus): Congenital anomaly, chromosomal abnormality, fetal infection (TORCH — toxoplasma, rubella, CMV, herpes, others), fetomaternal haemorrhage, hydrops fetalis.
- Group A (Amniotic fluid): Oligohydramnios, chorioamnionitis.
- Group M (Maternal): Pre-eclampsia/hypertension, gestational diabetes with poor control, obstetric cholestasis, systemic lupus, hypothyroidism, antiphospholipid syndrome, maternal infection, anaemia.
- Group I (Intrapartum): Acute hypoxia during labour — uterine rupture, cord prolapse, shoulder dystocia, prolonged obstructed labour. These are the preventable intrapartum deaths.
- Group N (Neonatal condition): A minority — where a neonatal condition was the primary cause.
- Group U (Unexplained): No condition identified despite full investigation.
Epidemiological context in India: The majority of stillbirths in India are antepartum (estimated 75–80%), with intrapartum stillbirths constituting the remaining 20–25%. Leading causes in the Indian context include placental causes (abruption, insufficiency), maternal hypertensive disorders, antepartum haemorrhage, congenital anomalies, and infection. A significant preventable fraction relates to undetected or poorly managed IUGR, pre-eclampsia, and intrapartum asphyxia.
Provided image
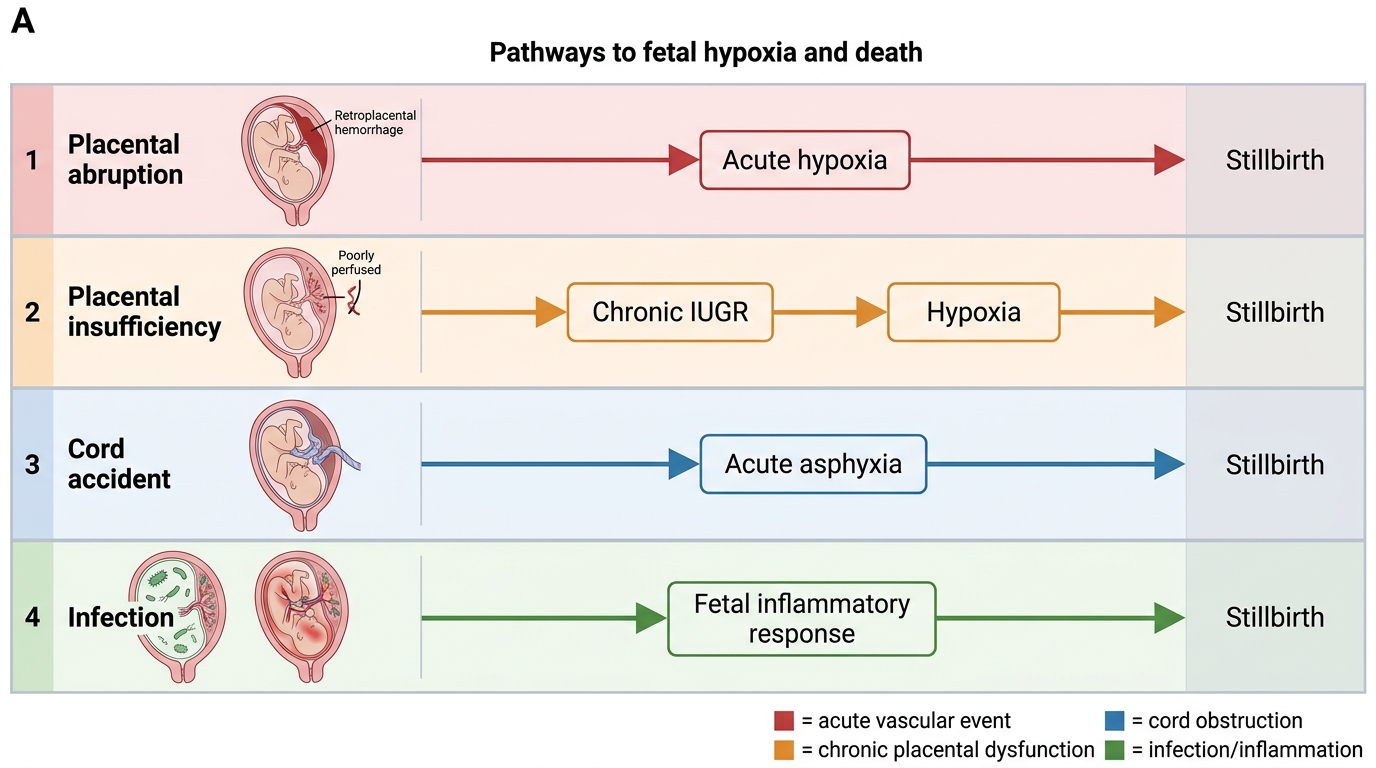
Mechanisms Leading to Stillbirth
SELF-CHECK
A woman delivers a stillborn baby at 30 weeks. The skin is slipping, the colour is brownish-green, and there is a foul odour. What classification applies, and what does this imply about the likely timing?
A. Fresh stillbirth — death occurred within the last few hours, likely intrapartum
B. Macerated stillbirth — death occurred ≥12–24 hours before delivery, likely antepartum
C. Neonatal death — the fetus showed brief signs of life after delivery
D. Abortion — the gestational age is below the stillbirth threshold
Reveal Answer
Answer: B. Macerated stillbirth — death occurred ≥12–24 hours before delivery, likely antepartum
Maceration features — skin slippage, discolouration, softening, foul odour — indicate that fetal death occurred at least 12–24 hours before delivery, making this an antepartum (not intrapartum) stillbirth. Fresh stillbirth has no maceration and suggests recent or intrapartum death. At 30 weeks (≥28 weeks) this meets the India stillbirth definition (not abortion). There is no mention of signs of life, so it is not a neonatal death.
Diagnosis and Investigation — Stillbirth Evaluation
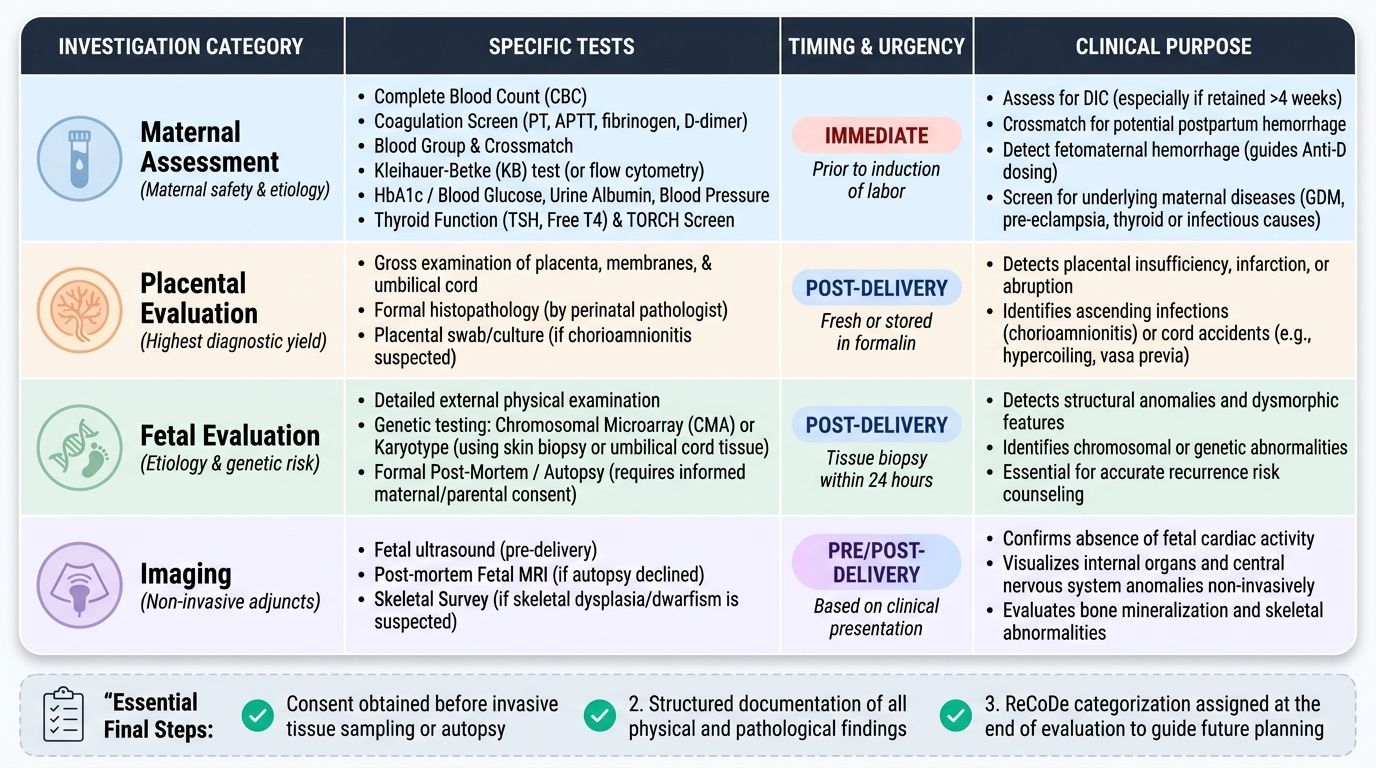
Once stillbirth is confirmed on ultrasound, a systematic investigation protocol should be initiated. The goals of investigation are three-fold: to identify a cause (which informs recurrence risk counselling), to detect conditions requiring immediate maternal management (most importantly DIC), and to provide the family with clear answers that facilitate grieving and future pregnancy planning. Not all investigations are available at every level of care — a district hospital may not be able to perform chromosomal microarray or formal autopsy — but a core minimum should always be pursued regardless of resource setting. Equally important is documentation: every finding must be recorded in a structured way and used to assign a ReCoDe category at the end of the evaluation. Investigations are divided into four tiers based on urgency and purpose: immediate maternal safety, placental examination, fetal examination, and selected specialised tests.
Step 1 — Immediate maternal assessment:
- Full blood count and coagulation screen (PT, APTT, fibrinogen, D-dimer): A retained dead fetus releases thromboplastin, which can precipitate DIC — a potentially life-threatening coagulopathy — especially if the fetus has been retained for >4 weeks. Coagulation screening is mandatory before induction of labour.
- Blood group and crossmatch: In case haemorrhage occurs during delivery.
- Kleihauer-Betke test (or flow cytometry for fetal cells): Detects fetomaternal haemorrhage — significant in Rh-negative women (anti-D immunoglobulin indication) and as a cause in its own right.
- Blood glucose, urine albumin, BP: To identify underlying maternal disease (GDM, pre-eclampsia).
Step 2 — Placental investigation:
- Gross examination of placenta at delivery: Weight, completeness, infarcts, retroplacental clot (abruption), cord length and insertion, knots, colour changes.
- Histopathological examination of placenta: The single most informative investigation in stillbirth evaluation. Should be performed in ALL stillbirths where available. Identifies villous infarction (placental insufficiency), chorioamnionitis (infection), fetal thrombotic vasculopathy, and vascular lesions.
Step 3 — Fetal investigation (with consent):
- External examination of stillborn: Dysmorphic features suggesting chromosomal abnormality or structural syndrome; weight and length (for gestation-specific growth assessment).
- Post-mortem examination (autopsy): Ideally should be offered and consent obtained; identifies internal structural anomalies and organ pathology that external examination misses. In practice, families often decline; virtual (MRI-based) autopsy is an emerging alternative where available.
- Karyotype or chromosomal microarray: From fetal skin/placental sample. Indicated when dysmorphic features are present, or as part of a comprehensive evaluation. Microarray has higher diagnostic yield for copy number variants.
- TORCH infection screen (maternal and/or fetal): Serology for toxoplasma, rubella, CMV, herpes, syphilis, hepatitis B.
- Thyroid function (maternal): Hypothyroidism is an underdiagnosed cause of stillbirth in India.
Step 4 — Thrombophilia screen (selected cases):
Antiphospholipid antibody syndrome (lupus anticoagulant, anticardiolipin, anti-β2-glycoprotein) is associated with recurrent stillbirth and placental thrombosis. Test in women with recurrent loss or clinical features of antiphospholipid syndrome.
Documentation: All findings must be systematically documented. Assign a ReCoDe category once investigations are complete. The investigation findings form the basis for the post-delivery counselling session.
Provided image
SELF-CHECK
A woman delivers a macerated stillbirth at 38 weeks. The retained fetus had been dead for an estimated 3 weeks. Which investigation is MOST urgently required before induction of labour?
A. TORCH serology
B. Fetal karyotype
C. Coagulation screen (PT, APTT, fibrinogen)
D. Placental histopathology
Reveal Answer
Answer: C. Coagulation screen (PT, APTT, fibrinogen)
Prolonged retention of a dead fetus (especially >4 weeks) releases thromboplastin, which can trigger DIC — a potentially fatal coagulopathy. Coagulation screening (PT, APTT, fibrinogen, D-dimer) is the most urgent maternal investigation before proceeding to induction. TORCH serology and karyotype are part of a comprehensive post-delivery investigation but are not urgent pre-induction tests. Placental histopathology is examined after delivery.