Page 17 of 23
OG9.6 | Hyperemesis Gravidarum — SDL Guide (Part 2)
Complications: Wernicke's Encephalopathy and Other Risks
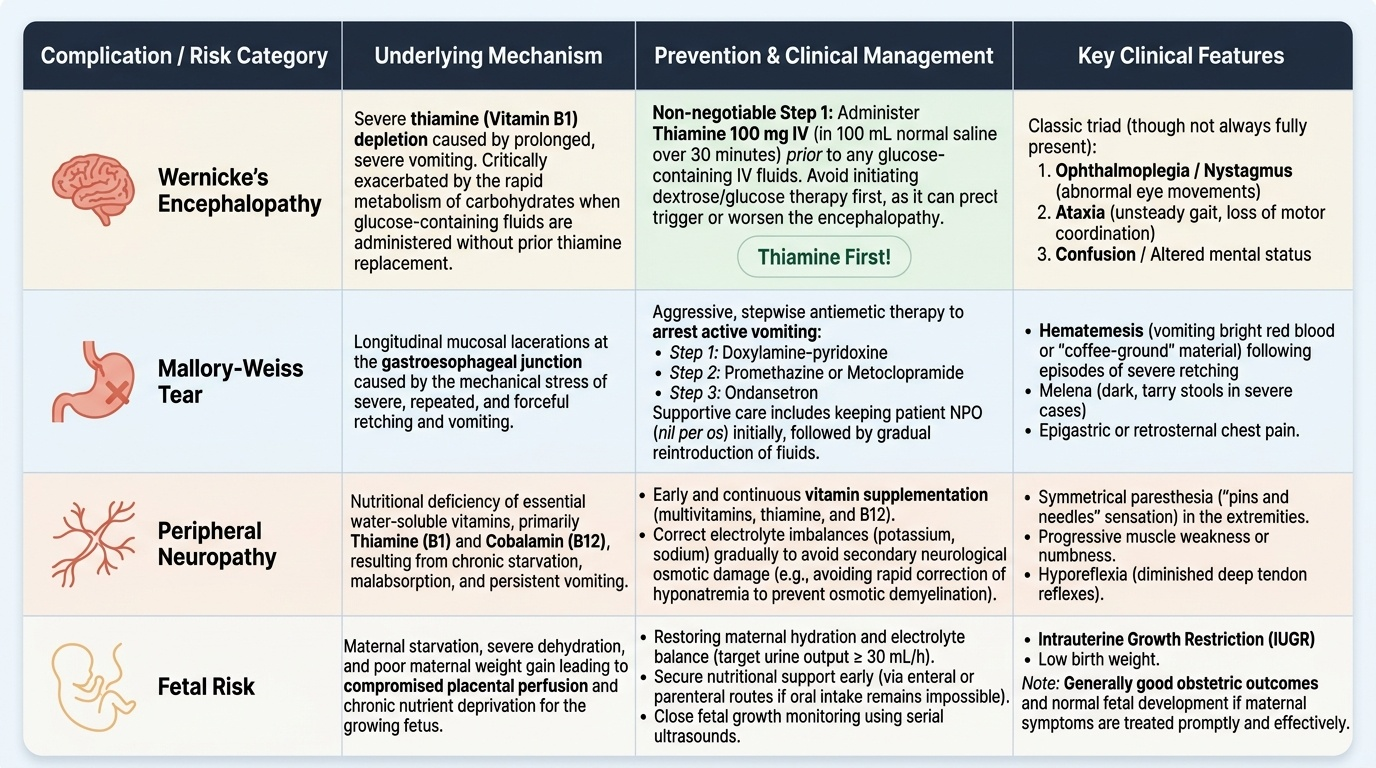
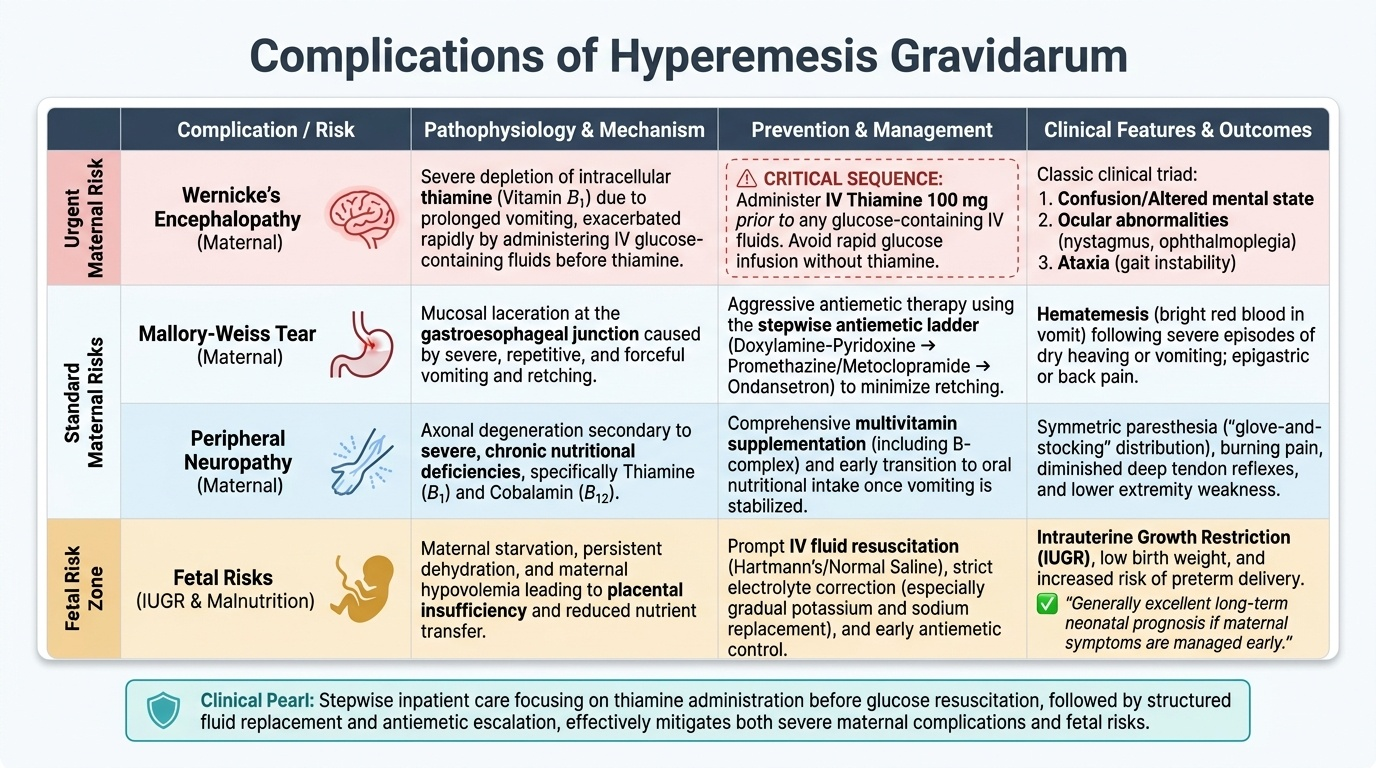
The complications of untreated or inadequately managed hyperemesis gravidarum span maternal neurological, structural, and haematological domains, and extend to fetal wellbeing.
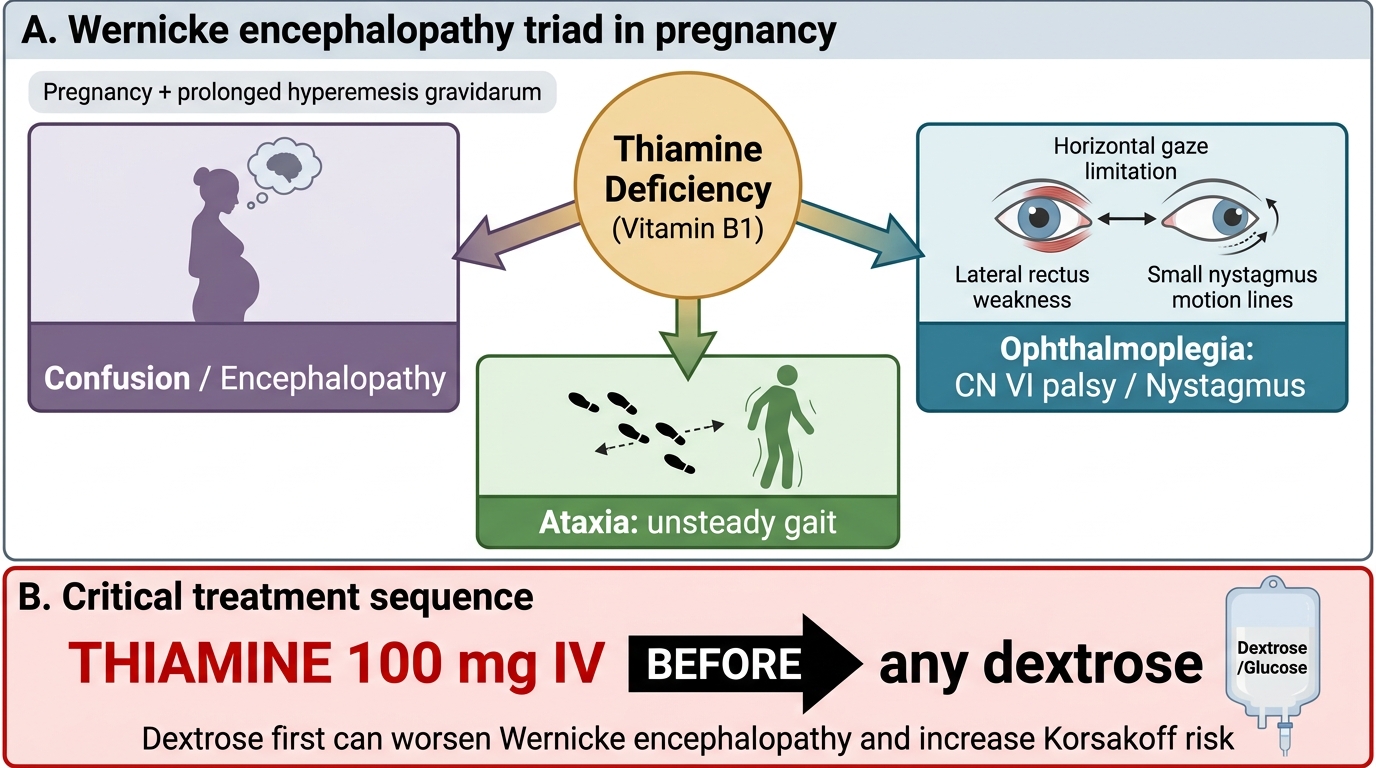
Wernicke's encephalopathy is the most serious and most preventable complication of HG. It results from thiamine (vitamin B1) deficiency in the context of prolonged vomiting and inadequate intake. Thiamine stores are exhausted within 2–3 weeks of poor intake. The classic triad of Wernicke's encephalopathy consists of: (1) confusion and altered consciousness (encephalopathy); (2) ophthalmoplegia — typically lateral rectus palsy (cranial nerve VI) causing diplopia, or nystagmus; and (3) gait ataxia from cerebellar and vestibular pathway involvement. All three features are rarely present simultaneously — any one should trigger urgent thiamine replacement. If untreated, Wernicke's progresses to Korsakoff's syndrome (irreversible amnesic psychosis with confabulation). The critical prevention principle bears repeating: 100 mg thiamine IV must be given before any dextrose-containing infusion. Infusing dextrose in a thiamine-depleted state rapidly depletes the last thiamine reserves and precipitates acute encephalopathy within hours.
Mallory-Weiss tears are longitudinal lacerations at the gastro-oesophageal junction caused by the mechanical shearing forces of repetitive, forceful retching. They typically present as haematemesis (blood-streaked vomiting) in the setting of severe HG. Most are self-limiting, but rarely, a full-thickness tear (Boerhaave syndrome) can occur and constitutes a surgical emergency.
Electrolyte complications. Severe hypokalaemia (serum K <2.5 mEq/L) can cause profound skeletal muscle weakness, cardiac arrhythmias, and rhabdomyolysis. Severe hyponatraemia, if corrected too rapidly, risks osmotic demyelination syndrome — a cerebellar and brain-stem demyelinating injury. Both require careful, monitored correction.
Venous thromboembolism (VTE). Pregnancy is already a hypercoagulable state (increased clotting factors, reduced protein S, venous stasis). Dehydration and immobility in HG compound this risk substantially. Women admitted with HG have a significantly elevated risk of deep vein thrombosis (DVT) and pulmonary embolism (PE) and should receive thromboprophylaxis with low-molecular-weight heparin (LMWH) once they are mobile — or immediately if prolonged immobility is anticipated.
Fetal impact. In most cases of HG, fetal outcomes are reassuringly normal. However, severe, prolonged HG with marked nutritional depletion is associated with intrauterine growth restriction (IUGR), low birth weight, and rarely premature birth. Adequate nutritional support (enteral or parenteral nutrition in refractory cases) is essential to optimise fetal outcome.
Wernicke Encephalopathy in Hyperemesis Gravidarum
SELF-CHECK
A woman with severe hyperemesis gravidarum for 3 weeks develops confusion, nystagmus, and unsteady gait. The most immediately correct management is:
A. CT head to exclude intracranial haemorrhage before starting any treatment
B. Urgent correction of hypokalaemia before anything else
C. 100 mg thiamine IV immediately, before any dextrose-containing fluid
D. Start 5% dextrose infusion quickly to correct hypoglycaemia first
Reveal Answer
Answer: C. 100 mg thiamine IV immediately, before any dextrose-containing fluid
The clinical triad — confusion, nystagmus/ophthalmoplegia, and ataxia — in the setting of prolonged HG is Wernicke's encephalopathy until proven otherwise. Treatment is immediate IV thiamine (100 mg in 100 mL normal saline) BEFORE any glucose or dextrose. Giving dextrose first would consume the patient's remaining thiamine reserves and precipitate acute Wernicke's / Korsakoff progression. This is the single most important clinical sequence to know.
Management: Stepwise Inpatient Care
Management of confirmed hyperemesis gravidarum requiring hospitalisation is systematic and follows a clear sequence of priorities. The goals are to restore hydration and electrolyte balance, arrest further thiamine depletion, suppress vomiting sufficiently to allow oral intake to resume, prevent thromboembolism, and support fetal nutrition.
Provided image
Step 1: Secure IV access and administer thiamine first. As soon as IV access is established, the first medication is thiamine 100 mg IV (in 100 mL normal saline over 30 minutes). This is non-negotiable and must precede any glucose-containing fluid. Only after thiamine has been given should IV fluid resuscitation commence.
Step 2: IV fluid and electrolyte replacement. The preferred IV fluid is Hartmann's solution (Ringer's lactate) or normal saline (0.9% NaCl). Glucose-containing fluids should be avoided until thiamine has been given. Potassium chloride (KCl) is added to each bag according to the degree of hypokalaemia — typically 20–40 mEq/L, and never as a bolus. Hyponatraemia, if present, must be corrected gradually (no faster than 10–12 mmol/L per 24 hours) to avoid osmotic demyelination. Fluid requirements are guided by urine output (target ≥30 mL/h), serum electrolytes, and clinical response.
Step 3: The antiemetic ladder. Antiemetics are given in a stepwise progression, starting with safer options and escalating when needed.
- First step — doxylamine-pyridoxine (Vitamin B6 10 mg + doxylamine 10 mg): This combination is the established first-line pharmacological antiemetic for NVP and early HG, with the most reassuring fetal safety data. It is licensed in Canada and the USA for this indication and widely recommended in international guidelines. It is available as a combination preparation.
- Second step — promethazine or metoclopramide: Promethazine (a first-generation H1-antihistamine, phenothiazine derivative) 12.5–25 mg IV/IM/PO every 4–6 hours is a commonly used antiemetic in HG in India and is effective, though it causes sedation. Metoclopramide (a dopamine D2 antagonist) 10 mg IV/IM/PO 8-hourly is also used; the risk of extrapyramidal side effects (acute dystonia, akathisia) limits its use to <5 days at a time.
- Third step — ondansetron: Ondansetron (a selective 5-HT3 receptor antagonist) 4–8 mg IV/IM/PO 8-hourly is effective second-line or add-on therapy in refractory HG. Safety concerns in the first trimester have been debated (conflicting data on oral cleft risk), and it should be used when the benefits outweigh the risks, typically after other antiemetics have been tried. It prolongs the QTc interval at higher doses; ECG monitoring is prudent. It is not considered first-line because of these pregnancy-specific safety questions.
- Fourth step — corticosteroids: Methylprednisolone (16 mg IV 8-hourly for 3 days, then oral taper) is reserved for truly refractory HG after all other measures have failed. It carries teratogenic concerns (oral cleft risk) and should not be used before 10 weeks of gestation. It is a treatment of last resort.
Step 4: Additional therapeutic measures. Histamine H2-receptor antagonists (e.g., ranitidine) or proton pump inhibitors (e.g., omeprazole) reduce gastric acid secretion and reflux oesophagitis, which compounds nausea. Ginger (1 g/day oral) has Level I evidence for mild-to-moderate NVP reduction and can be used alongside pharmacotherapy. Thromboprophylaxis with LMWH (e.g., enoxaparin 40 mg SC once daily) is initiated once the woman is mobilising or during prolonged admission. Compression stockings are used from admission. Nutritional support: if the woman cannot tolerate enteral feeds after 3–4 days of treatment, nasogastric tube feeding should be considered; in the most severe refractory cases, total parenteral nutrition (TPN) via a central line is required.
Discharge criteria. The woman can be discharged when she can tolerate oral fluids and at least a light diet, when ketonuria has cleared, when electrolytes are normalised, and when she is no longer dehydrated. She must be given clear written advice on when to return (persistent vomiting, inability to drink, further weight loss) and community antiemetics.
Provided image
SELF-CHECK
A 25-year-old woman at 8 weeks gestation is hospitalised with hyperemesis gravidarum. She has been vomiting for 10 days, has 3+ ketonuria, serum K 3.1 mEq/L, and serum Na 131 mEq/L. The medical officer writes orders for 5% dextrose with 20 mEq KCl at 125 mL/h. As the treating intern, what is the FIRST correction you should make to this order?
A. Increase the KCl to 40 mEq/L before starting the bag
B. Change 5% dextrose to Hartmann's solution AND add thiamine 100 mg IV before any fluid
C. Add ondansetron 4 mg IV as a separate order
D. Start normal saline immediately without waiting for any additional drug
Reveal Answer
Answer: B. Change 5% dextrose to Hartmann's solution AND add thiamine 100 mg IV before any fluid
Two errors need correction: (1) Dextrose-containing fluid should not be given before thiamine — it risks precipitating Wernicke's encephalopathy. (2) The preferred IV fluid is Hartmann's solution or 0.9% normal saline. The correct first action is to change the fluid to Hartmann's/NaCl AND give thiamine 100 mg IV before starting the drip. Adding KCl 20 mEq/L is fine but not the primary safety correction here.
Self-Assessment: Integrating the HG Framework
Having worked through the full clinical picture of hyperemesis gravidarum, use this section to consolidate your understanding through an integrated clinical scenario before proceeding to the closing quiz and reflection.
Consider a 24-year-old primigravida at 11 weeks gestation who is referred from primary care with a three-week history of unrelenting vomiting. She has lost 4.5 kg from a booking weight of 72 kg (6.25% loss), has been unable to drink water for 48 hours, and her urine dipstick today shows 3+ ketones and specific gravity 1.025. Her blood results show: Na 129 mEq/L, K 2.8 mEq/L, ALT 68 U/L, TSH 0.01 mIU/L, fT4 24 pmol/L, thyroid antibodies negative. Ultrasound shows a single live intrauterine pregnancy at 11 weeks with no features of molar pregnancy.
Applying the diagnostic framework from this SDL: she meets all three criteria for hyperemesis gravidarum — weight loss >5%, ketonuria ≥2+, and electrolyte disturbance. The mildly elevated ALT is an expected finding in severe HG (hepatic steatosis from nutritional depletion) and does not indicate primary liver disease here. The suppressed TSH with elevated fT4 in the absence of antibodies, goitre, or eye signs is gestational transient thyrotoxicosis — no antithyroid treatment is needed; repeat TFTs at 20 weeks.
For management, the admission sequence is: (1) thiamine 100 mg IV in 100 mL normal saline over 30 minutes before any IV fluid; (2) Hartmann's solution with potassium supplementation (20–40 mEq/L KCl, never bolus), correcting Na at no more than 10–12 mmol/L per 24 hours given the hyponatraemia; (3) antiemetics starting with doxylamine-pyridoxine, escalating as needed; (4) LMWH thromboprophylaxis given the dehydration and hospital admission; (5) daily monitoring of urine ketones, electrolytes, and fluid balance until resolution. Discharge when she tolerates oral fluids, ketonuria has cleared, and electrolytes are normalised.
CLINICAL PEARL
The thiamine-before-dextrose rule is the single most important clinical sequence in hyperemesis gravidarum management. Thiamine (vitamin B1) is essential for pyruvate dehydrogenase and therefore for the entry of pyruvate into the Krebs cycle. In a thiamine-depleted, starved woman, infusing glucose (dextrose) drives pyruvate accumulation and precipitates acute Wernicke's encephalopathy within hours. Wernicke's presents as the classic triad of confusion, ophthalmoplegia (typically lateral rectus palsy or nystagmus), and ataxia — but only one or two features may be present at first. Treat with thiamine 100 mg IV before the dextrose bag, every time, without exception. If you suspect Wernicke's is already developing, give thiamine immediately and concurrently — do not wait for investigations.
Second pearl — gestational transient thyrotoxicosis is not Graves' disease. Up to 60% of women with HG have a suppressed TSH. The absence of thyroid antibodies, goitre, and eye signs, plus the correlation with hCG peak, identifies gestational transient thyrotoxicosis — a self-limiting phenomenon that requires no treatment and resolves spontaneously as hCG falls. Starting carbimazole in this setting is an avoidable, potentially harmful error.